Download presentation
Presentation is loading. Please wait.

1
بسم الله الرحمن الرحيم

2
CASE

7
Sterptococci Gram Positive cocci, 0.5 to 1 μ in diameter, diplo -cocci or short or long chain Facultative anaerobe, Catalase Neg.

8
Taxonomy Haemolysis Serologic Biochemical Ecologic features Molecular genetics

9
Haemolysis

10
Group-Specifi c Substance (Lancefield Classification) Lancefield groups A – H and K – U For group A streptococci: rhamnose- N -acetylglucosamine; For group B: rhamnose-glucosamine polysaccharide For group C: rhamnose- N -acetylgalactosamine; For group D: glycerol teichoic acid containing d-alanine and glucose; For group F: glucopyranosyl- N -acetylgalactosamine
 Lancefield groups A – H and K – U For group A streptococci: rhamnose- N -acetylglucosamine; For group B: rhamnose-glucosamine polysaccharide For group C: rhamnose- N -acetylgalactosamine; For group D: glycerol teichoic acid containing d-alanine and glucose; For group F: glucopyranosyl- N -acetylgalactosamine")
11
Lancefield Groups Membrane Ag Groups A-H, K-V –Group A Strep. pyogenes –Group B Strep. agalactiae –Group C, F, G Strep equisimilis Strep zooepidemicus Strep anguinosus –Group D Strep bovis Strep equines –Group K Strep salivarius –Viridans Strep mutans Strep mitis Strep sanguis –Pneumococci

12
ٍ Sterptococci

13
Streptococcus pyogenes Causative agent of suppurative and non supurative diseases In liquid media: long chains Typing: Group specific Ag: N-Acetyl Glucose-amine, Rhamnose Type specific Ag: M and M like proteins, T protein M Prot: Acid and Heat stable, Trypsin labile T Protein: Trypsin Stable, acid and Heat labile

14
Pathogenesis 1- Adhesion to host cells: M, M like and Proteins, Lipo teichoic acid, Capsule 2- Invasion to Et cells: F, M, and M like proteins 3- Toxinogenecity: C5A peptidase, Streptokinase, O and S Lysins, Pyrogenic Exotoxins 4- Inhibition of Phagocytosis andOpsonisation: C5A peptidase, Streptolysins, Mprot., Capsule

15
Virulence Factors Cell Wall components 1- Lipoteichoic acid: Adhesion to ET cells and fibronectin 2-Mprotein: 150 serotypes in N-term., Anti phagocytic, Attach to H factor Attach to Fc, Fibrinogen 3- Capsular Polysaccharide

16
M protein In the absence of M type-specific antibodies, they are able to resist phagocytosis by polymorphonuclear leukocytes by inhibiting activation of the alternate complement pathway S pyogenes that lack M protein are not virulent. Immunity to infection with group A streptococci is related to the presence of type-specific antibodies to M protein. Group C and group G streptococci have genes homologous to the genes for M protein

17
M protein Purified streptococcal cell wall membranes induce antibodies that react with human cardiac sarcolemma Conserved antigenic domains on the class I M protein cross react with human cardiac muscle, and the class I M protein may be a virulence determinant for rheumatic fever.

18
Other Antigenic structures T Substance T substance is acid labile and heat labile Permits differentiation of certain types of streptococci by agglutination with specific antisera R protein Nucleoproteins Extraction of streptococci with weak alkali yields mixtures of proteins and other substances of little serologic specificity, called P substances, which probably make up most of the streptococcal cell body.

19
Virulence Factors 2- Extracellular components: PyrogenicToxins: SpeA, SpeB, SpeC, SpeF Superantigenic Causes the release of Il- 1, 2 and 6, TNF α and β and γ INF Specific and Non specific mitogen, myocardial and Hepatic necrosis and reduction of Ab synthesis Lysogenic, main virulence factor in Scarlet fever

20
Super Antigen

21
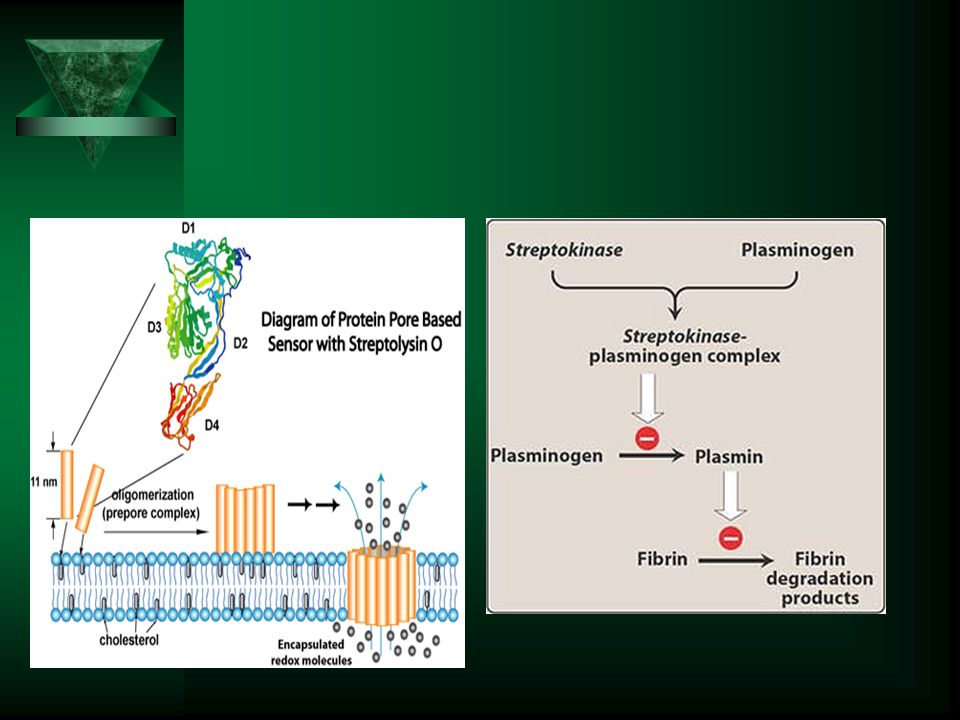
Virulence Factors 2- Extracellular components: Streptolysins SLO: Oxygen labile cytotoxins, Immunogenic, Inhibited by cholesterol, Pore forming SLS: Cell attached, non immunogenic, Oxygen stable Active on Cell membrane phospholipids Stimulate the release of lysosomal contents after engulfment, with subsequent death of the phagocytic cell Streptolysin S is produced in the presence of serum

22
Virulence Factors Streptokinases: A and B. Immunogen, In association with plasminogen activator : produces plasmin: lysis of blood cloth Streptodornase:Dnase: A –D, Immunogen C5a peptidase Hyaloronidase

24
24

25
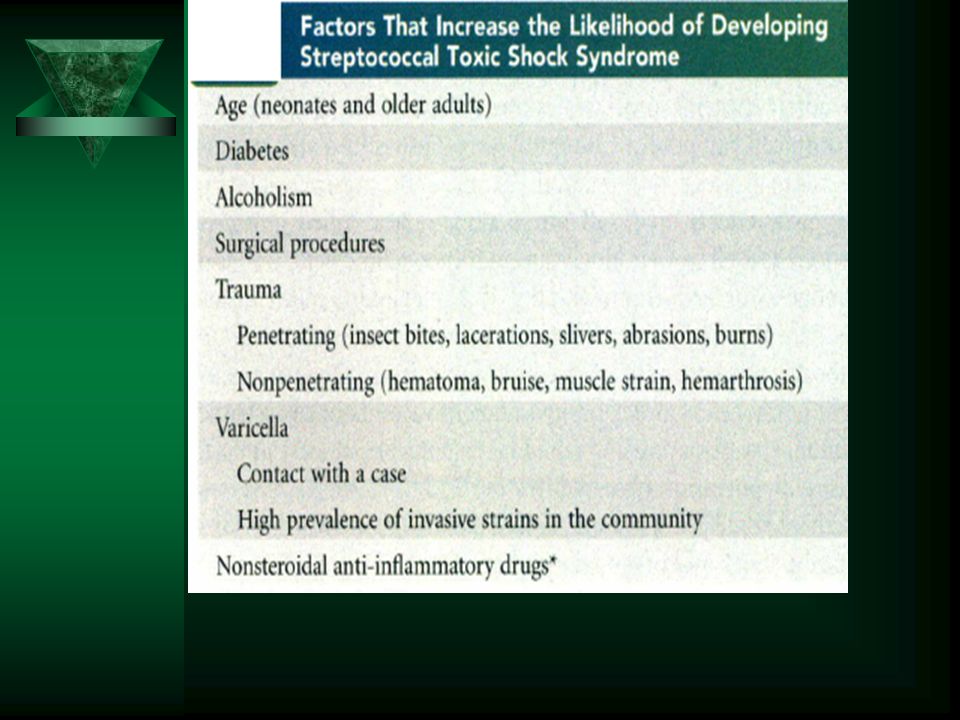
Epidemiology Transient colonization in upper respiratory tract and skin surface with disease caused by recently acquired strains(before protective antibodies are produced) Person-to-person spread by respiratory droplets (pharyngitis) or through breaks in skin after direct contact with infected person, fomite, or arthropod vector Individuals at higher risk for disease include children 5 to 15 years old (pharyngitis); children 2 to 5 years old with poor personal hygiene (pyoderma); patients with soft-tissue infection (streptococcal toxic shock syndrome); patients with prior streptococcal pharyngitis (rheumatic fever, glomerulonephritis) or soft-tissue infection (glomerulonephritis
 Person-to-person spread by respiratory droplets (pharyngitis) or through breaks in skin after direct contact with infected person, fomite, or arthropod vector Individuals at higher risk for disease include children 5 to 15 years old (pharyngitis); children 2 to 5 years old with poor personal hygiene (pyoderma); patients with soft-tissue infection (streptococcal toxic shock syndrome); patients with prior streptococcal pharyngitis (rheumatic fever, glomerulonephritis) or soft-tissue infection (glomerulonephritis")
26
Streptococcal Diseases

27
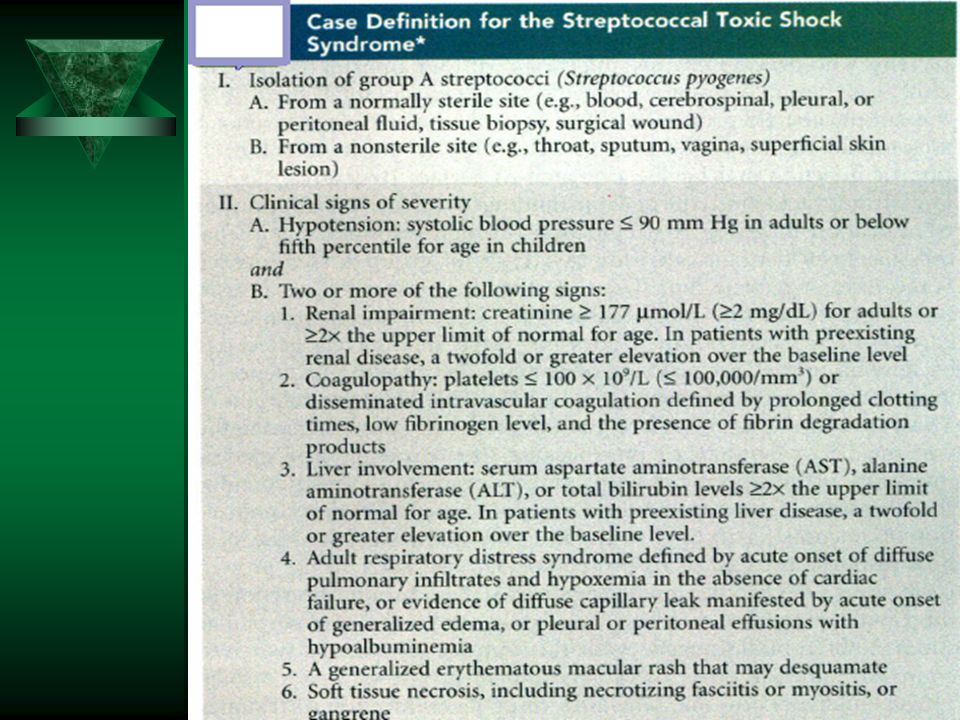
Suppurative Infections Pharyngitis Scarlet fever Pyoderma Erysipelas Cellulitis Necrotizing fasciitis Streptococcal toxic shock syndrome endometritis, wound infections, and urinary Puerperal fever Nonsuppurative Infections Rheumatic fever Acute glomerulonephritis :

28
Pharyngitis Malaise, feverishness, and headache Nausea, vomiting, and abdominal pain are common in children. Redness, edema, and lymphoid hyperplasia of the posterior portion of the pharynx, enlarged, hyperemic tonsils, patchy discrete tonsillopharyngeal exudates

29
Differential Features of Group A Streptococcus (GAS) and Viral Pharyngitis FindingsSuggestive of GAS Infection SYMPTOMS –Sore throat –Dysphagia –Fever –Headache –Abdominal pain –Nausea/vomiting SIGNS –Soft palate petechiae –Anterior cervical lymphadenopathy –Scarlet fever rash Findings Suggestive of Viral Infection SYMPTOMS –Cough –Running nose –Hoarse voice –Diarrhea SIGNS –Stomatitis –Conjunctivitis
 and Viral Pharyngitis FindingsSuggestive of GAS Infection SYMPTOMS –Sore throat –Dysphagia –Fever –Headache –Abdominal pain –Nausea/vomiting SIGNS –Soft palate petechiae –Anterior cervical lymphadenopathy –Scarlet fever rash Findings Suggestive of Viral Infection SYMPTOMS –Cough –Running nose –Hoarse voice –Diarrhea SIGNS –Stomatitis –Conjunctivitis")
30
Strawberry Tongue

31
Scarlet Fever

32
Scarlet fever Diffuse, erythematous, blanching, fine papular rash Exudative pharyngitis may occur, but this finding also is common with viral pharyngitis In infants, the only symptoms may be low-grade fever, fussiness, and decreased feeding.

33
Pyoderma (impetigo)
")
34
Erysiplas

35
Cellulitis Acute spreading inflammation of the skin and subcutaneous tissues, results from infection of burns, wounds, or surgical incisions but may also follow mild trauma. Local pain, tenderness, swelling, and erythema The process may extend rapidly to involve large areas of skin. Systemic manifestations: fever, chills, and malaise, lymphangitis, bacteremia, or both The lesion is not raised

36
Necrotising Faciitis

37
Multiple pyoderma lesions

40
Clinical Manifestation 1- Influenza-like prodrome: fever, chills, myalgias, nausea, vomiting, and diarrhea that precedes hypotension by 24 to 48 hours.Confusion in 55% of patients 2- Tachycardia, tachypnea, persistent fever and, in patients who subsequently have necrotizing fasciitis or myonecrosis, increasingly severe pain at the site of infection. 3- Sudden onset of shock and organ failure, hypotension

41
Puerperal fever endometritis

42
Rheumatoid Fever ARF presents as an acute febrile illness, with clinical manifestations that include arthritis, carditis, skin lesions, and neurologic disturbances The arthritis, occurring in 75% of patients who have ARF, is a migratory polyarthritis, affecting several joints in rapid succession, most commonly larger joints Treatment with nonsteroidal anti-inflammatory drugs (NSAIDs) or salicylates class I M protein types (e.g., types 1, 3, 5, 6, and 18)
 or salicylates class I M protein types (e.g., types 1, 3, 5, 6, and 18)")
43
Rheumatoid Fever The rate of isolation of GAS from the oropharynges of patients who have ARF is only between 10% and 20% Serologic testing, which demonstrates either elevated antibody titers or rising titers with serial testing, is used more often for confirmation of infection The streptozyme test measures five streptococcal antibodies : –antistreptolysin O (ASO), –antihyaluronidase(AHase), –antistreptokinase (ASKase), –Antinicotinamideadenine dinucleotidase (anti-NAD), –and antideoxyribonuclease B (anti-DNase B) antibodies.
, –antihyaluronidase(AHase), –antistreptokinase (ASKase), –Antinicotinamideadenine dinucleotidase (anti-NAD), –and antideoxyribonuclease B (anti-DNase B) antibodies.")
44
Jones criteria for the Diagnosis of Acute Rheumatic Fever Jones Criteria for the Diagnosis of Acute Rheumatic Fever Diagnosis: Requires 2 major criteria or 1 major and 2 minor criteria plus evidence of recent group A streptococcal infection MajorMinorEvidence of Recent GAS Infection Carditis Polyarthritis Chorea Erythema marginatum Subcutaneous nodules Fever Arthralgia Elevated acute phase reactants Prolonged PR interval Positive throat culture or RADT or Elevated or rising antistreptococcal antibody titers RADT_rapid antigen detection test

45
Aschoff bodies

46
Subcutaneous nodules

47
Erythema marginatum

48
TREATMENT OF ARF Treatment of ARF focuses on eradication of acute disease manifestations, and prophylaxis against future GAS infection to prevent recurrent ARF Eradication of GAS requires the same antibiotic regimens that are used to treat GAS pharyngitis In addition, household contacts should have throat cultures performed and be treated if the cultures are positive for GAS Aspirin, administered at 80 to 100 mg/kg per day and continued until all symptoms have resolved, is the major anti- inflammatory agent used for symptom relief.

49
Post streptococcal Glomerulonephritis Poststreptococcal glomerulonephritis (PSGN) is the most common cause of acute nephritis worldwide PSGN is caused by previous throat or skin infection with nephritogenic strains of GAS Although the exact mechanism is unclear, antigens of nephritogenic streptococci are believed to induce immune complex formation in the kidneys The latent period is 1 to 3 weeks following GAS pharyngitis and 3 to 6 weeks following GAS skin infection.
 is the most common cause of acute nephritis worldwide PSGN is caused by previous throat or skin infection with nephritogenic strains of GAS Although the exact mechanism is unclear, antigens of nephritogenic streptococci are believed to induce immune complex formation in the kidneys The latent period is 1 to 3 weeks following GAS pharyngitis and 3 to 6 weeks following GAS skin infection.")
50
Post streptococcal Glomerulonephritis Diagnosis requires clinical findings of acute nephritis in the setting of a recent GAS infection. If throat or skin cultures are negative, confirmation of a recent GAS infection may be obtained through serologic testing. Renal biopsy typically is not performed to confirm the diagnosis of PSGN M types 2, 42, 49, 56, 57, and 60 SpeB and a nephritis-associated plasmin receptor are very important in PSGN pathogenesis

51
TESTS Serologic testing: may be used to confirm GAS pharyngitis. –The antibody response occurs 2 to3 weeks after the onset of infection, –Serologic testing consists of measurements of antistreptococcal antibody titers, such as antistreptolysin O and antideoxyribonuclease B. Rapid antigen detection test (RADT): –RADT is suggested for initial use in patients who are likely to have GAS pharyngitis and in those whose throat culture results will not be available for more than 48 hours. –RADT has a specificity of 95% and greater and a sensitivity of 65% to 90%. –Low sensitivity Throat Culture: the gold standard, with 90% to 95% sensitivity
: –RADT is suggested for initial use in patients who are likely to have GAS pharyngitis and in those whose throat culture results will not be available for more than 48 hours. –RADT has a specificity of 95% and greater and a sensitivity of 65% to 90%. –Low sensitivity Throat Culture: the gold standard, with 90% to 95% sensitivity.")
52
Beta Haemolysis Bacitracin

53
TREATMENT GOALS Treatment of GAS pharyngitis has several goals: – reducing the incidence of suppurative and non suppurative complications, –reducing the duration and relieving symptoms and signs of infection, –and reducing transmission to others.

54
Treatment Pharyngitis: Penicillin G, Erythromycin, Azithromycin, FGC Impetigo: P. G. Erysipelas: Pen Necrotizing Fasciitis: P, Debridement STSS: Clindamycin, Penicillin

55
CASE

57
Differential Diagnosis

58
Streptococcus agalactiae Groupe B Ag: Rham. NAGA, Gal Type Ag: Capsular polysaccharide: 9 serotypes C protein-

59
Epidemiology Asymptomatic colonization of the upper respiratory tract and genitourinary tract Mother is without type-specific antibodies and has low complement levels No seasonal incidence Colonization in lower GI tract and vagina Ia, III and V are important serotypes Ia, Ib and III has terminal residue of sialic

60
What does group B Strep do? Colonisation –Asymptomatic and intermittent –Intestinal (<30% of adults) –Vaginal (<25% of women) Infection –Newborn babies –Adults: the elderly, pregnant/postpartum women, others with underlying disease
 –Vaginal (<25% of women) Infection –Newborn babies –Adults: the elderly, pregnant/postpartum women, others with underlying disease.")
61
Age-specific rates of group B Strep bacteraemia reports Source: Health Protection Report Vol. 5 No. 46 – 18 November 2011

62
Group B Strep infection “Early onset” 0-6 days (~75% cases) –90% show within 12 hours –Usually septicaemia and pneumonia –11% mortality, 7% morbidity –90% preventable IV Penicillin –Ia, III, V “Late onset” 7-90 days (~25% cases) –Usually meningitis and septicaemia –8% mortality, 21% morbidity (up to 50% with meningitis) –No current prevention: good hygiene/education –Vaccine: future hope for both late & early onset –III
 –90% show within 12 hours –Usually septicaemia and pneumonia –11% mortality, 7% morbidity –90% preventable IV Penicillin –Ia, III, V Late onset 7-90 days (~25% cases) –Usually meningitis and septicaemia –8% mortality, 21% morbidity (up to 50% with meningitis) –No current prevention: good hygiene/education –Vaccine: future hope for both late & early onset –III")
63
Group B Strep infection In Pregnant women: UTI, Amnionitis, Endometritis, Wound Infections In Non pregnant women and Men: Soft tissue infection, Bactremia, Urocepsis, Pneumonia, Bone and Joint Infection Ia and V

64
Known risk factors for EOGBS infection Previous GBS baby 10 x GBS bacteriuria current pregnancy 4 x Maternal intrapartum fever (>38 0 C) 3 x Preterm labour 3 x
 3 x Preterm labour 3 x")
65
Countries routinely screening pregnant women for GBS Australia Argentina Belgium Canada Czech Republic France Germany Hong Kong Italy Kenya Poland Spain Slovenia Switzerland USA

66
“Gold Standard” test for GBS carriage When? –35-37 weeks of pregnancy Where & who? –Low vagina & anorectal swab/s (no speculum) –Health care professional or pregnant woman What culture method? –Enriched Culture Medium (ECM) - 24-48 hours to grow –LIM, Todd Hewit broth Medium
 –Health care professional or pregnant woman What culture method. –Enriched Culture Medium (ECM) hours to grow –LIM, Todd Hewit broth Medium.")
67
Treatment, Prophylaxis Pen + Aminoglycoside Vanco Profilaxis: IV Ampicillin

68
PYR CAMP

69
Streptococcus-Like Organisms Leuconostoc –Resemble streptococci microscopically; colonies resemble viridans group or Enterococcus –Found in plants, vegetables, and dairy products Pediococcus –Found in nature; used in bioprocessing and biopreservation of foods such as cheese, meats, and vegetables –Rarely seen in human infections; has been associated with septicemia

70
Oral and Other Non-b-Haemolytic Streptococci Anginosus Group Streptococci Mitis Group Streptococci Bovis Group Streptococci Salivarius Group Streptococci Mutans Group Streptococci

71
Anginosus Group Streptococci Members of the oral flora and are found in the gastrointestinal and genital tracts and Three separate but closely related species: – Streptococcus anginosus Streptococcus constellatus Streptococcus intermedius Isolates of S. anginosus and S. constellatus may have Lancefield F, C, A or G antigens β-haemolytic strains but most are non-β-haemolytic

72
Mitis Group Streptococci Habitate: human oropharyngeal microflora Streptococcus sanguis Streptococcus mitis S. pneumoniae

73
Salivarius Group Streptococci Important component of the oral ecosystem because of the production of an extracellular fructose polysaccharide (levan) from dietary sucrose and the production of urease by some strains Streptococcus thermophilus
 from dietary sucrose and the production of urease by some strains Streptococcus thermophilus")
74
Mutans Group Streptococci Colonize the tooth surfaces of humans and certain animals and are associated with dental caries Eight serotypes or serovars (designated a–h) and six distinct species S. mutans

75
Bovis Group Streptococci Human S. bovis strains are divided into two biotypes based on their ability (biotype I) or inability (biotype II) to ferment mannitol.
 or inability (biotype II) to ferment mannitol..")
76
INFECTIONS CAUSED BY NON- b-HAEMOLYTIC STREPTOCOCCI Infective Endocarditis Abscesses Infections in the Immunocompromised Caries

77
LABORATORY DIAGNOSIS Specimens: blood, pus, wounds, skin swabs and biopsies, dental plaque, saliva and other oral sites Nonselective examples include blood agar 2, Columbia agar, fastidious anaerobic agar brain– heart infusion agar supplemented with 5% defibrinated horse or sheep blood

78
Questions?

79
نمونه سوالات علوم پايه

80
آزمايش CAMP برای تشخيص آزمايشگاهی کدام يک از گروه ها لانسفيلد استرپتوکوکوسی استفاده می شود الف - گروه A ب - گروه B ج - گروه G د - گروه D شهريور 85

81
آزمايش افتراقی جهت تشخِص استافيلوکوکوس ها از استرپتوکوکوس ها کدام است. الف - کاتالاز ب - اکسيداز ج - اوره آز د - کواگولاز اسفند 87 و...

82
تقسِم بندی معمول استرپتوکوکوس ها ( لانسفيلد ) بر اساس کدام خصوصیت زیر است الف - نوع هموليز ب - کربوهيدرات های ديواره سلول ج - پروتئين M د - پروتئين T اسفند 77
 بر اساس کدام خصوصیت زیر است الف - نوع هموليز ب - کربوهيدرات های ديواره سلول ج - پروتئين M د - پروتئين T اسفند 77")
83
عامل بيماری زرد زخم عبارت است از : الف - استافيلوکوکوس و ميکروکوکوس ب - استرپتوکوکوس و باسيلوس آنتراسيس ج - استافيلوکوکوس و استرپتوکوکوس د - استرپتوکوکوس و پنوموکوکوس اسفند 77

84
کدام يک از موارد زير در تقسيم بندی لانسفيلد در استرپتوکوکوس ها مورد استفاده قرار می گيرد الف - آنتی ژن کپسولی ب - پروتئين M ج - آنتی ژن های فلاژل د - کربوهيدرات C اسفند 87

Similar presentations


 Lawrence Pike.>")











 Definition: Rheumatic fever (RF) is an autoimmune disease affecting the heart and extra- cardiac.>")


 Cocci Chapters 22-24. Staphylococcus Major groups - coagulase (+) aureus vs. (-) others. External Structures Capsule - polysaccharide,>")

>")
