Download presentation
Presentation is loading. Please wait.

1
The London Health Observatory: monitoring health and health care in the capital, supporting practitioners and informing decision-makers Born Equal? Inequalities in infant mortality in London Bobbie Jacobson, Director Caroline Bowles, Public Health Analyst

2
Born Equal? Our aims To review inequalities in infant mortality in London in relation to the National Public Service Agreement (PSA) target set by Government To analyse the contribution made by risk factors for infant mortality in London To review the potential for providing commissioners and providers with local intelligence for monitoring progress in local implementation
 target set by Government To analyse the contribution made by risk factors for infant mortality in London To review the potential for providing commissioners and providers with local intelligence for monitoring progress in local implementation.")
3
Infant Mortality: the Policy Context Many relevant overlapping policies including: –The National Service Framework (NSF) for children, young people and maternity services (DH, 2004), particularly standard 11 on maternity services setting improvements for 2014 –Every Child Matters (DFES, 2004) –Maternity Matters (DH, 2007) –Healthcare for London: A framework for Action (NHS London, 2007)
 for children, young people and maternity services (DH, 2004), particularly standard 11 on maternity services setting improvements for 2014 –Every Child Matters (DFES, 2004) –Maternity Matters (DH, 2007) –Healthcare for London: A framework for Action (NHS London, 2007)")
4
Infant Mortality: The Current Pattern of Inequality in London

5
The National Infant Mortality PSA Target By 2010 to reduce the inequalities in health outcomes by 10% as measured by infant mortality and life expectancy at birth –Starting with children under one year, by 2010 to reduce by at least 10 per cent the gap in mortality between the routine and manual groups* and the population as a whole. –*Routine and Manual (R&M): based on the occupation of the father and includes the following categories; lower supervisory, lower technical, semi-routine and routine occupations.
: based on the occupation of the father and includes the following categories; lower supervisory, lower technical, semi-routine and routine occupations..")
6
National Picture Comparison of the rate in the R&M group to the rate in the general population with a projection to the 2010 target

7
* Inside marriage and outside marriage/joint registration only. Classification into the R&M group is based on fathers occupation. Therefore, excludes sole registered births from both groups.

8
Data and Methods Looked at risk factors contributing to infant deaths e.g. characteristics of the mother and infant There are too few deaths in a year to look at linked infant mortality rates broken down by risk factor at the level of borough Therefore factors associated with infant mortality are investigated. Pilot analysis of potential use of Maternity Hospital Episode Statistics (HES) data (Gestation at first antenatal appointment) R&M groups are based on the fathers occupation. Therefore the target excludes sole registered births. This is a high risk group in London for infant mortality.
 data (Gestation at first antenatal appointment) R&M groups are based on the fathers occupation. Therefore the target excludes sole registered births. This is a high risk group in London for infant mortality..")
9
Sole registered births are identified as a high risk group in London, 8.9 infant deaths per 1,000 live births (2001-03), compared to 6.7 infant deaths per 1,000 live births to fathers in routine and manual occupations
, compared to 6.7 infant deaths per 1,000 live births to fathers in routine and manual occupations")
10
Key Risk Factors in London Correlations between the infant mortality risk factors and the infant mortality rate for London boroughs 2001-2003 Risk factorCorrelation coefficient Statistically significant Proportion of low birth-weight (<2500g) births.761Yes Proportion of very low birth-weight (<1500g) birth.722Yes Proportion of births to mothers born in at risk countries (West Africa, Caribbean Commonwealth and East Africa).653Yes Proportion of sole registered births.605Yes Proportion of births to mothers living in areas with over 40 IMD score.572Yes Proportion of births to mothers aged under 20 years old.446Yes Proportion of births to couples with the father in routine and manual occupations.402Yes Proportion of births to mothers aged over 40 years old.009No
 births.761Yes Proportion of very low birth-weight (<1500g) birth.722Yes Proportion of births to mothers born in at risk countries (West Africa, Caribbean Commonwealth and East Africa).653Yes Proportion of sole registered births.605Yes Proportion of births to mothers living in areas with over 40 IMD score.572Yes Proportion of births to mothers aged under 20 years old.446Yes Proportion of births to couples with the father in routine and manual occupations.402Yes Proportion of births to mothers aged over 40 years old.009No")
11
Tackling Health Inequalities locally An example from a sample of PCTs below:

12
Healthcare for London: Maternity and Newborn Care “Women’s social and medical needs should be assessed at an early stage….with their care based on these assessments” “GPs should communicate the importance of healthy living (diet exercise and stopping smoking) for conception and pregnancy and commission services to support women to adopt healthy lifestyles “A key aim would be to improve outcomes such as breastfeeding”
 for conception and pregnancy and commission services to support women to adopt healthy lifestyles A key aim would be to improve outcomes such as breastfeeding")
13
Commissioning effective interventions 3 NHS interventions were selected that: have a positive impact on infant mortality, are locally modifiable and can be monitored using routinely available data: 1.Smoking in pregnancy 2.Initiation of breastfeeding 3.Early booking of antenatal care Arbitrary cut-off points used in the absence of evidence based targets Data grouped into three bands of colour from the worse (red) to the better (green).
 to the better (green).")
14
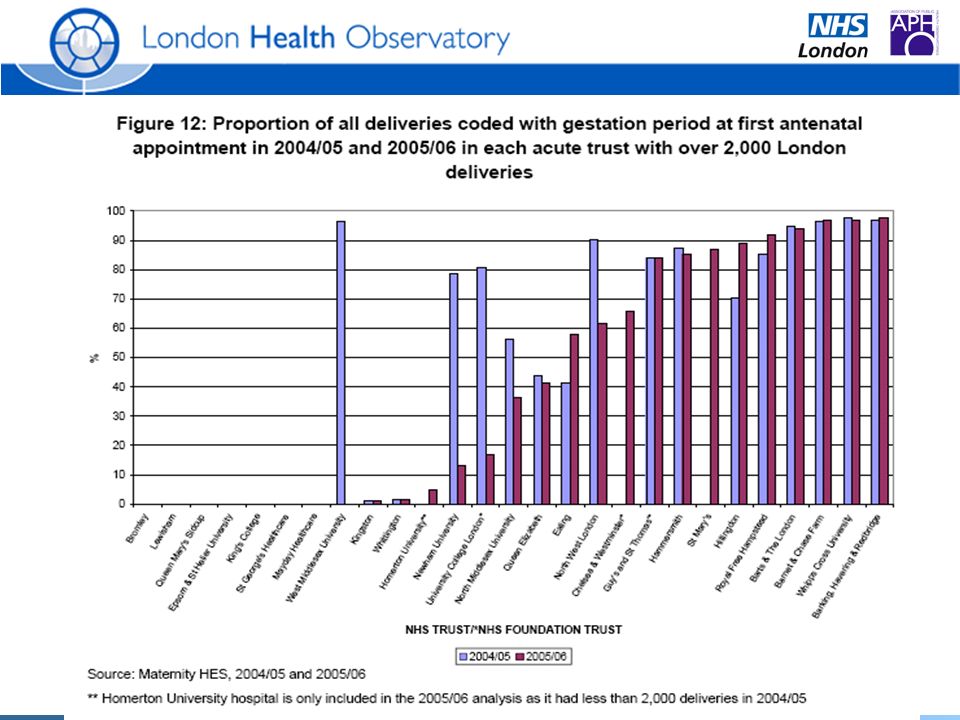
An example - access to antenatal care Early antenatal booking is likely to have a positive impact on infant mortality Ensuring women in R&M and Black and minority ethnic groups book early and are able to access antenatal care may help reduce infant mortality ‘Maternity Matters’ highlights the need for every woman to be supported by a midwife and that self-referral to a midwife as a choice will speed up and enable earlier access to maternity services Maternity Hospital Episode Statistics (HES) look at gestation period at first antenatal appointment –the later the gestation at first appointment the higher the risk
 look at gestation period at first antenatal appointment –the later the gestation at first appointment the higher the risk")
15
Shows proportion of deliveries coded with gestational age and who had booked an early first antenatal appointment (< 12 wks) for 2004/05 and 2005/06. Areas of poor data quality have been revealed and improving these will help to improve local monitoring of infant mortality. An example - access to antenatal care

16
Access to antenatal care Data quality and completeness is variable and is not adequate for monitoring across London as a whole. Only 45.3% of deliveries had gestation period electronically coded in 2005/06. In London PCTs this ranged from 0.6% to 96.5%, largely reflecting the pattern of completeness between different acute trusts Of the 27 London acute trusts (with 2,000 or more deliveries), 8 did not record any gestation period in maternity HES. This accounted for 26% of all London deliveries.
, 8 did not record any gestation period in maternity HES. This accounted for 26% of all London deliveries..")
17
Inequalities in Early antenatal Booking

19
Ethnic differences in access to Early Antenatal Booking

20
Key Messages for London There are unacceptable inequalities in infant mortality – better maternity services targeted at more deprived areas can save 41 lives every year Well targeted local action needs to be more widely focussed - ‘at risk’ deprived neighbourhoods have been identified in all but three of London boroughs. Focus is needed on tackling wider causes of infant mortality such as reducing child poverty, improving education and employment opportunities. There are a number of indicators that can be monitored to help provide better evidence to commissioners on local progress, including smoking in pregnancy, breast feeding and antenatal care. The utility of these indicators depends on gaining commitment of all local acute trusts to better collection and recording of routine information across all ethnic groups.

21
Born Equal? For further information and copies of the full report and briefing please visit: Website: www.lho.org.uk orwww.lho.org.uk Email: caroline.bowles@lho.nhs.ukcaroline.bowles@lho.nhs.uk

Similar presentations


















 1991-932008-10.>")
