Download presentation
Presentation is loading. Please wait.

1
Respiratory Rate – The Forgotten Vital Sign Franklin Miller, MA, RRT Clinical Solutions Specialist Philips Healthcare

2
What are Vital Signs?

3
“Doing the same thing over and over again and expecting a different result.” Albert Einstein

4
What is the problem we are trying to solve? Avoiding to fall off a cliff Slowly drowning in quicksand

5
“People die unnecessarily every single day in our hospitals. It is likely that each clinician can provide an example of a patient who, in retrospect, should not have died during their hospitalization.” Institute for Healthcare Improvement “How-to-Guide: Rapid Response Teams” 5 The Challenge

6
Except for sudden catastrophic events, no patient in a hospital bed should be allowed to deteriorate to the point they stop breathing or their heart stops! Terri Wells, RN

7
Rapid Response Teams 7 Institute of Health Care Improvement (IHI) strategy included 6 initiatives in an effort to save 100,000 lives in U.S. Hospitals Number one on this list of initiatives was the deployment of a rapid response team. IHI recommendations 2004

8
Look of RRT Each facilities team is different Often single parameter initiated 8 Table 1. Rapid Response System Models ModelPersonnelDuties Medical Emergency Team Physicians (critical care or hospitalist) and nurses Respond to emergencies Critical Care Outreach Critical care physicians and nurses Respond to emergencies Follow up on patients discharged from ICU Proactively evaluate high-risk ward patients Educate ward staff Rapid Response Team Critical care nurse, respiratory therapist, and physician (critical care or hospitalist) backup Respond to emergencies Follow up on patients discharged from ICU Proactively evaluate high-risk ward patients Educate and act as liaison to ward staff
 and nurses Respond to emergencies Critical Care Outreach Critical care physicians and nurses Respond to emergencies Follow up on patients discharged from ICU Proactively evaluate high-risk ward patients Educate ward staff Rapid Response Team Critical care nurse, respiratory therapist, and physician (critical care or hospitalist) backup Respond to emergencies Follow up on patients discharged from ICU Proactively evaluate high-risk ward patients Educate and act as liaison to ward staff.")
9
Old Way to Intervene: Focus on CPR

10
“A new systematic review and meta-analysis (Chan et al 2010) of studies on rapid response teams (RRT’s) again concludes that the evidence fails to support a significant impact of RRT’s on mortality.” Chan PS, Jain R, Nallmothu BK, Berg RA, Sasson C. Rapid Response Teams: A Systematic Review and Meta-analysis. Arch Intern Med. 2010; 170(1): 18-26
:")
11
“Hospital Errors are the Third Leading Cause of Death in U.S., and New Hospital Safety Scores Show Improvements Are Too Slow”

12
Unexpected hospital deaths per day is equal to 33 airplane crashes per day

13
The Challenge Research indicates: Critical events are frequently preceded by one or more signs of physiological deterioration in commonly measured vital signs Subtle signs of deterioration appear 6 to 8 hours before an adverse event takes place.* * MET, Devita et al. Springer 2006 Despite our best intentions, patients suffer adverse events… Dr. Daryl A. Jones

14
Early Warning Scoring Perspective from the Institute for Healthcare Improvement 16 Recommends health care organizations implement a multi-parameter scoring system as part of their Rapid Response Team effort IHI recommendations 2011 “Such a system can help build reliability into the Rapid Response Team system and attempt to or try to guarantee that no at-risk patients are missed”, says the 5 Million Lives Campaign’s Kathy Duncan.

16
EWS with Response Teams Hospitals that have implemented an EWS in addition to a RRT have seen anywhere from a 17% to 110% increase in RRT s depending on the algorithm used to trigger the RRT based on the EWS(Gardner-Thorpe, J et al (2006) Early warning scoring system proven to increase staff’s confidence in the communication of a patient’s medical condition (Liaw et al, 2011)
 Early warning scoring system proven to increase staff’s confidence in the communication of a patient’s medical condition (Liaw et al, 2011)")
18
What is the solution? Immediately react to an immanent threat Proactively mitigate the risk of a potential future threat

21
National Early Warning Score Royal College of Physicians 2012

22
22 Early Warning Scoring MEWS: Physiological changes detected by a number of parameters can provide a more obvious and specific clinical picture of deterioration or instability before any one of them alone could detect this. 3 < 70 <85% Heart Rate Systolic Blood pressure Respiration rate SpO2 Temperature Level of consciousness 2 <40 71-80 <8 <90% <35 Confused 1 41-60 81-100 35.1-36.5 0 61-90 101-139 9-14 36.6-37.4 Alert 1 91-110 140-169 15-20 37.5 Voice 2 111-130 170-199 21-29 Pain 3 >130 >200 >30 Uncons. Score

23
Methods for Collecting MEWS Paper Error prone EMR Latency, Latency, Latency RARELY is entering data into the EMR the 1st thing (or even 5th thing) on a caregivers list Someone has to be in front of the EMR and pulling up the EWS screen to review
 on a caregivers list Someone has to be in front of the EMR and pulling up the EWS screen to review")
24
Case Study National Teaching Institute 2013 Joanna Emmons, MSN, RN, ACNS-BC, CCNS, CCRN July, 2013 Confidential 79 year old male patient admitted with a CVA Evaluated and treated by neurology and neurosurgery Found to experience aspiration with swallowing and a PEG tube was placed Plans for discharge to rehab

25
AdmissionDay 2Day 2Day 3Day 3 RR16 (1)18 (1)28(2) HR7293(1)116 (1) SBP120140(1) Temp97.3 F97.2 F99.5 F NeuroVoice (1) MEWS246 Data from Joanna Emmons, MSN, RN, ACNS-BC, CCNS, CCRN Case Study 3 < 70 <85% Heart Rate Systolic Blood pressure Respiration rate SpO2 Temperature Level of consciousness 2 <40 71-80 <8 <90% <35 Confused 1 41-60 81-100 35.1-36.5 0 61-90 101-139 9-14 36.6-37.4 Alert 1 91-110 140-169 15-20 37.5 Voice 2 111-130 170-199 21-29 Pain 3 >130 >200 >30 Uncons.
18 (1)28(2) HR7293(1)116 (1) SBP120140(1) Temp97.3 F97.2 F99.5 F NeuroVoice (1) MEWS246 Data from Joanna Emmons, MSN, RN, ACNS-BC, CCNS, CCRN Case Study 3 < 70 <85% Heart Rate Systolic Blood pressure Respiration rate SpO2 Temperature Level of consciousness 2 < <8 <90% <35 Confused Alert Voice Pain 3 >130 >200 >30 Uncons.")
26
Case Study Day 4Day 4Day 5Day 5Day 6Day 6 RR24(2) 32 (3) HR120 (2)132 (2)140 (3) SBP100(1)98(1)96(1) Temp37.3 C37.8 C38.7 C (2) NeuroVoice (1) MEWS679 Data from Joanna Emmons, MSN, RN, ACNS-BC, CCNS, CCRN 3 < 70 <85% Heart Rate Systolic Blood pressure Respiration rate SpO2 Temperature Level of consciousness 2 <40 71-80 <8 <90% <35 Confused 1 41-60 81-100 35.1-36.5 0 61-90 101-139 9-14 36.6-37.4 Alert 1 91-110 140-169 15-20 37.5 Voice 2 111-130 170-199 21-29 Pain 3 >130 >200 >30 Uncons.
 32 (3) HR120 (2)132 (2)140 (3) SBP100(1)98(1)96(1) Temp37.3 C37.8 C38.7 C (2) NeuroVoice (1) MEWS679 Data from Joanna Emmons, MSN, RN, ACNS-BC, CCNS, CCRN 3 < 70 <85% Heart Rate Systolic Blood pressure Respiration rate SpO2 Temperature Level of consciousness 2 < <8 <90% <35 Confused Alert Voice Pain 3 >130 >200 >30 Uncons.")
27
Case Study Conclusion RRT activated at 0705 on hospital day 6 –team arrived at 0710 Code Blue called at 0719 while RRT team present. Time of death- 0734 d/t pt unresponsive to ACLS. Data from Joanna Emmons, MSN, RN, ACNS-BC, CCNS, CCRN

28
July, 2013 Failure to Recognize results in a Failure to Respond that Results in a Failure to Rescue No method to recognize subtle deterioration Results in delay in intervention No clear defined action list Improve Outcomes Confidential

29
Deterioration Detection 85% 90% 92% 94% 98% SpO2 Safety Limit (Alarm) 3 2 1 MEWS thresholds SpO2 Deterioration Detection range Fire Alarm Smoke Detector
 MEWS thresholds SpO2 Deterioration Detection range Fire Alarm Smoke Detector")
30
30 Up to 40% of unexpected deaths in hospitals occur on the general floor (IHI-TCATB) Retrospective vital signs data shows: o Measurements sometimes incomplete (RR missing 15.4% of time) o No specific escalation criteria for abnormal vitals o Nurse visits vary in frequency and duration o Judgment varies according to training, experience, hierarchy, culture The Challenge Failure to Recognize the Signs = Failure to Rescue
 Retrospective vital signs data shows: o Measurements sometimes incomplete (RR missing 15.4% of time) o No specific escalation criteria for abnormal vitals o Nurse visits vary in frequency and duration o Judgment varies according to training, experience, hierarchy, culture The Challenge Failure to Recognize the Signs = Failure to Rescue")
32
Documented Resp Rates Resp Rate obtained by Resp Pod 32

33
Small, lightweight and compact body-worn solution Attached with a patch, preferred on the left costal arch of the patient’s chest Derives respiration rate, patient posture and pulse rate at defined time intervals by using 3D accelerometer technology Respiratory Monitor

34
Change Focus to Prevention Record - Recognize - Report - Respond Dr. Chris Subbe

35
Key Findings Mean time required to complete and record a set of vital signs reduced by ~50% Survival rate following RRT call increased by 6.3% among patients who had an RTT call LOS in US hospitals reduced by 3 percent for all patients admitted to the study wards Vitals I Clinical Study: Critical Care Medicine 2012 Vol. 40, No 8, 2349-2361, Aug 2012 10 hospitals ww (5 US, 4 EU, 1Aus) 12 Wards 349 beds Cohort of 18.305 patients (pre: 9.617, post 8.688) Timeframe : June 2009 – August 2010 Main Hypothesis : positive outcome when using MP5SC for vital signs collection in conjunction with EWS (Early Warning Scoring) Software Early Warning Scoring Advantages of embedding EWS in vital signs monitors
 12 Wards 349 beds Cohort of patients (pre: 9.617, post 8.688) Timeframe : June 2009 – August 2010 Main Hypothesis : positive outcome when using MP5SC for vital signs collection in conjunction with EWS (Early Warning Scoring) Software Early Warning Scoring Advantages of embedding EWS in vital signs monitors.")
36
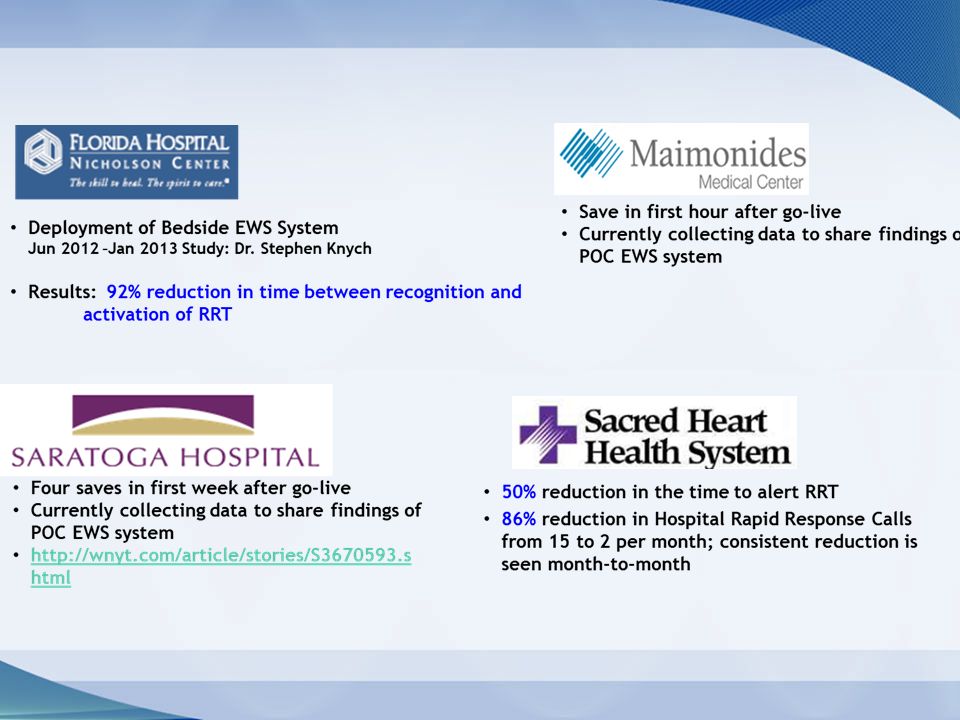
Transformation Success Earlier intervention: 76% reduction in the time to alert the Rapid Response Team 70% reduction in Hospital Code Blue from Q1 – Q4 2013 12% reduction in Length of Stay (From 3.3 – 2.9 days) Code blue cost savings = $800,000 savings (Note: This is customer reported data that is non-peer reviewed) Results delivered during AACN 2013 Boston, MA NO CODE BLUES ON PILOT FLOOR FOR OVER 825 days
 Code blue cost savings = $800,000 savings (Note: This is customer reported data that is non-peer reviewed) Results delivered during AACN 2013 Boston, MA NO CODE BLUES ON PILOT FLOOR FOR OVER 825 days")
Similar presentations




 in Wales Chris Subbe, Wrecsam>")


 Module 3: Responding to clinical deterioration – managing common acute conditions Communicating clinical concerns—using ISBAR.>")






 introduced.>")



. The relationship between emergency department.>")



