Download presentation
Presentation is loading. Please wait.

1
1000 lives + Mini Collaborative: Community Bundle Marie Lewis Donna Owen Powys Local Health Board

2
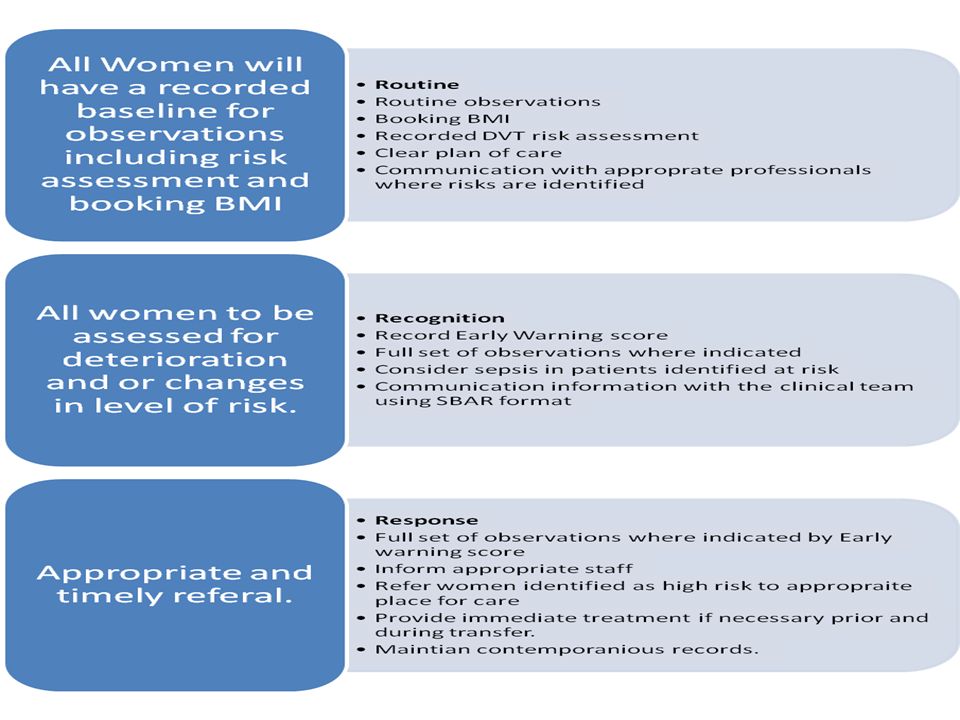
Transforming Maternity Services Mini collaborative: Community Model The community bundle is made up of three aspects similar to the four care bundles within Transforming Maternity Services. Pre-Admissions: All women have adequate history taken and recorded in their hand held records including BMI, Medical conditions, Obstetric History and VTE risk assessment. Plan for frequency of observations. Recognition: Routine maternal observations carried out as per local guidelines. Risk assessments repeated as appropriate and any changes recorded within the hand held records. Early warning score used as trigger for full set of observations and referral if necessary. Response: Communication with all members of the team using the SBAR format. Referral to appropriate place for further care and investigation. Immediate care if necessary prior to and during transfer. Mechanism for recording findings, actions and follow up.

3
When implementing the community bundle organisations need to consider local processes for referral from community to acute settings, the acceptable timeframe and communication process feeding back to community from the acute setting.

5
Community Risk assessment tool for venous thrombosis [VTE] Obstetrician Review SUMMARY: Reviewed by: Date: This assessment needs to form part of any further risk assessment following identification of risk factors (and referral) or during any AN hospital admission. Deep Vein Thrombosis Risk Assessment Booking Indications for consideration of antenatal thromboprophylaxis All women to be assessed by midwife at first/booking appointment. YE S NOYESNO Previous DVT/PEAntithrombin deficiency Systemic lupus erythematosisSickle cell disease Antiphospholipid syndromeMyeloproliferative disorder BMI ≥45kg/m 2 Consider referral to anaesthetist as per local guidance Assessed by Date / Signature If one or more Indications (above) present, woman to be referred for obstetric led care and consideration of antenatal thromboprophylaxis. Referred to (if appropriate): Date: Please refer to local guidance re referral timeframes and follow-up.
![Community Risk assessment tool for venous thrombosis [VTE] Obstetrician Review SUMMARY: Reviewed by: Date: This assessment needs to form part of any further risk assessment following identification of risk factors (and referral) or during any AN hospital admission.](http://images.slideplayer.com/34/10235295/slides/slide_5.jpg "Deep Vein Thrombosis Risk Assessment Booking Indications for consideration of antenatal thromboprophylaxis All women to be assessed by midwife at first/booking appointment. YE S NOYESNO Previous DVT/PEAntithrombin deficiency Systemic lupus erythematosisSickle cell disease Antiphospholipid syndromeMyeloproliferative disorder BMI ≥45kg/m 2 Consider referral to anaesthetist as per local guidance Assessed by Date / Signature If one or more Indications (above) present, woman to be referred for obstetric led care and consideration of antenatal thromboprophylaxis. Referred to (if appropriate): Date: Please refer to local guidance re referral timeframes and follow-up..")
6
Routine: All Women are risk assessed at booking. Documented in hand held records Referred to consultant where VTE risk has been identified. This assessment is to identify risk factors for referral and should be used in conjunction with local guidelines for referral to consultant care. Clinical judgement remains a priority. The community midwife is not responsible for deciding whether thromboprophylaxis is required. But is responsible for following up the outcome of her referral.

7
Recognition: Community midwives are key players in recognising when deterioration or deviation from norm occurs. The early warning score does not replace clinical judgement but is designed to aid community midwives in decision making, consistency and documentation. All women at every opportunity should be asked about their wellbeing. And the EWS recorded.

8
Full set of observations: At each contact, the healthcare professional should ask the woman about her health and wellbeing. Where a woman reports feeling well, routine care should be given, no additional observations are necessary. However any symptoms reported by the woman or identified through clinical observations should be assessed. [NICE CG 37] If a women reports feeling unwell or has a EWS of 1 a full set of observations should be carried out. Full set of observations should include: Heart rate Respiratory rate Systolic blood pressure Maternal wellbeing Temperature Observations should be scored using the Early Warning score as a trigger for referral. Health Professionals always remain responsible for the decisions they make and regardless of the early warning score should refer to the obstetric unit any concerns that they have.

9
Community Early Warning Score Aide memoir: Score0123 Looks/feels wellYesNo Respirations9-20 /min21-24/ min25-29/ min 30/ min Pulse61-100/min101-110/min41-60 or 111-129/min 130/min Systolic BP100-140mmhg141-160mmhg91-99mmhg 161mmhg Diastolic BPUp to 90mmhg91-99mmhg100-109mmhg>110 or <40mmhg Temperature36-37.935.1-35.938-39 40

10
EWS Score 0 Score 3 or above Score 1-2 Continue routine care Refer to consultant care Complete full set Obs if not previously done and commence Mews chart Score 1-2 Repeat full set Obs in 30 mins 1-2 discuss with Appropriate professional for plan of care. Health care professionals should use their clinical judgement at all times when making decisions the EWS is not conclusive.

11
Recognition: Where indicated women should be referred to an appropriate setting and a full plan of care recorded. To aid communication and documentation the SBAR format is recommended.

12
Addressograph Date: Time Left: Time Arrived: Transfer from: Transfer to: Arranged with (Name) Maternal Transfer Document Situation: Reason Background: Gravida: Para: EDD: Gestation: Relevant medical/obstetric history Assesment: - Clinical Impression/Actions/observations Recommendation: including your requests and expected time frame Midwife: Date: Time:
 Maternal Transfer Document Situation: Reason Background: Gravida: Para: EDD: Gestation: Relevant medical/obstetric history Assesment: - Clinical Impression/Actions/observations Recommendation: including your requests and expected time frame Midwife: Date: Time:")
13
Work so far: We have piloted the community model with one midwife. Her response: the model was clear to understand and easy to use. The documentation needs to be incorporated into clinical paperwork and not additional. It is all stuff we do already why do we need something new? Mews chart is un-necessary and wasteful when most women will only have one set of obs. The community model is now being piloted amongst the wider team.

14
What next: Wider pilot needed in other community settings. Consider using National Early warning score? Data collection system needed: suggested as part of retrospective record keeping audit? Implementation plan to include awareness raising in MW’s, GP’s and DGH’s. Education and training needs analysis: importance of measuring resps and referral to appropriate professionals.

15
Coos card We were also asked to look at separately piloting a client satisfaction card. The aim of the card is to get customer feedback and a scoring system to monitor client satisfaction with the service. We used a satisfaction card that had been developed for use within Powys and added the recommended score system.

16
What next: Wider pilot needed in other community settings. Data collection system needed: monitor results. Implementation plan.

17
What the women think: We have piloted the cards in one area of Powys: Women said: they were easy to understand. They were a good way of feeding back. The boxes were too small for comments.

18
Thank you Marie Lewis: marie.lewis2@wales.nhs.uk Donna Owen: donna.owen2@wales.nhs.uk

Similar presentations



![Presented by [Insert name of presenter] [Insert title] [Insert LHD/SHN name] Month 2014 PD2014_030 Using Resuscitation Plans in End of Life Decisions.](/12/3498778/big_thumb.jpg "Presented by [Insert name of presenter] [Insert title] [Insert LHD/SHN name] Month 2014 PD2014_030 Using Resuscitation Plans in End of Life Decisions.>")


 Scottish Government Health Directorates.>")









![Template for study specific training for Intrapartum Research Studies [ Please see guide before using this]](/23/6849745/big_thumb.jpg "Template for study specific training for Intrapartum Research Studies [ Please see guide before using this]>")


