Download presentation
Presentation is loading. Please wait.

1
Chapter 26: The Urinary System
3 Lectures: Gross Anatomy of Kidneys How filtrate is formed and how the rate of filtration (GFR) is controlled Tubular reabsorption and secretion
 is controlled. Tubular reabsorption and secretion.")
2
Kidneys (2), ureters (2), urinary bladder (1) & urethra (1)
Kidneys filter blood plasma and returns water and solutes back to blood What remains is urine Urine flows from each kidney, down its ureter to the bladder and to the outside via the urethra

3
Overview of Kidney Functions
Regulation of blood ionic composition Na+, K+, Ca+2, Cl- and phosphate ions Regulation of blood pH H+ and HCO3 Regulation of blood volume conserving or eliminating water Regulation of blood pressure Excretion of wastes Production of hormones (erythropoietin & calcitriol) Help maintain Homeostasis
 Help maintain Homeostasis.")
4
External Anatomy of the Kidneys
Paired kidneys - kidney-bean-shaped Located just above the waist between the peritoneum & posterior wall of abdomen retroperitoneal along with adrenal glands & ureters Protected by 11th & 12th ribs Right kidney lower because of liver Renal hilus – where ureters and blood vessels enter/exit

5
External Layers of the Kidney
Renal Capsule – Deepest smooth transparent sheet of dense irregular connective tissue–helps maintain the shape of the kidney Adipose Capsule – Intermediate protects the kidney from trauma Renal Fascia – Superficial anchors kidney to the surrounding structures and to the abdominal wall

6
POSTERIOR

7
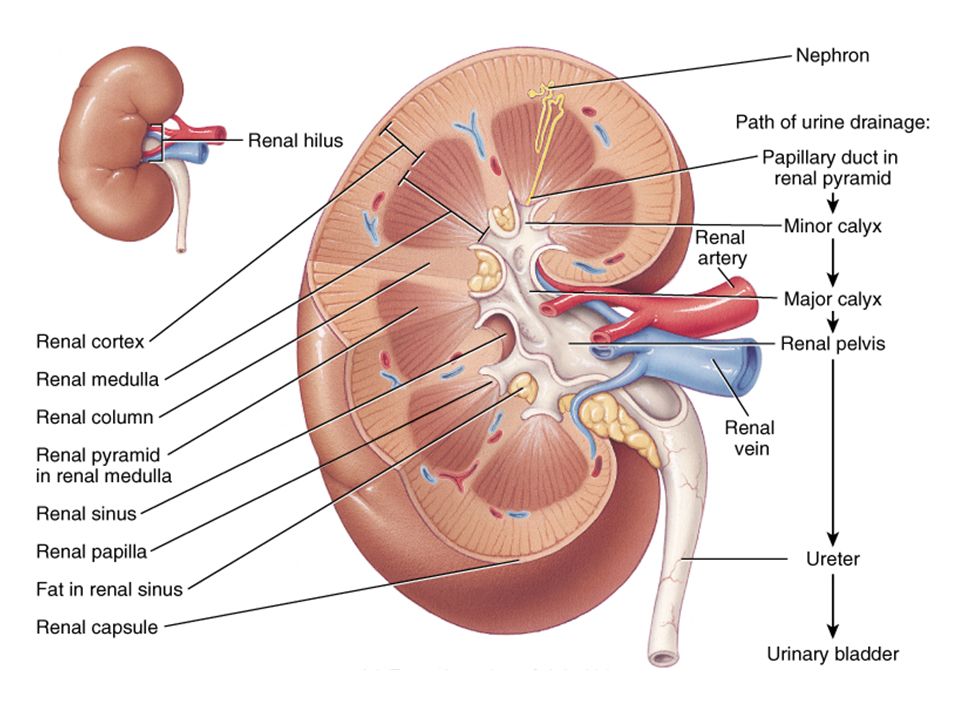
Internal Anatomy of the Kidneys
Two Distinct Regions: Renal Cortex: Superficial light red region Renal Medulla Deep, dark reddish-brown region consists of 8-18 cone-shaped renal pyramids separated by renal columns renal papilla point toward the Renal hilum Together the Renal Cortex and the Renal Medulla constitute the parenchyma – functional portion of kidney

9
Number of Nephrons Remains constant from birth – one million
any increase in size of kidney results in an increase in size of individual nephrons If injured, no replacement occurs Dysfunction is not evident until function declines by 25% of normal (other nephrons handle the extra work) Removal of one kidney causes enlargement of the remaining until it can filter at 80% of normal rate of 2 kidneys
 Removal of one kidney causes enlargement of the remaining until it can filter at 80% of normal rate of 2 kidneys.")
10
The Nephron – functional unit of kidney
Renal Corpuscle: filtration Gomerulus Glomerular capsule (Bowman’s capsule) Renal Tubules: reabsorption & secretion Proximal convoluted tubule (PCT) Nephron loop (loop of Henle) Distal convoluted tubule (DCT) DCTs of several nephrons empty into a single Collecting Duct
 Renal Tubules: reabsorption & secretion. Proximal convoluted tubule (PCT) Nephron loop (loop of Henle) Distal convoluted tubule (DCT) DCTs of several nephrons empty into a single Collecting Duct.")
11
Juxtamedullary Nephrons – 15%
Two Types of Nephrons Cortical Nephrons – 85% Juxtamedullary Nephrons – 15%

12
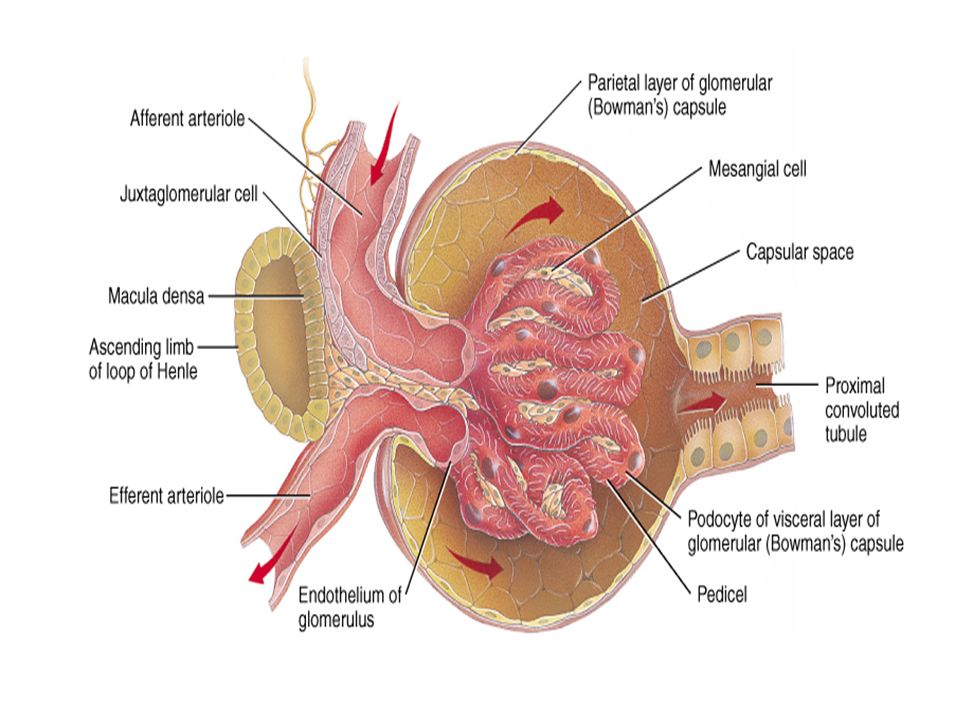
Glomerular (Bowman’s) Capsule
Bowman’s capsule surrounds glomerulus forming capsular space Two layers of capsule: Visceral layer – Podocytes – “foot cells” modified simple squamous Parietal layer – Simple squamous epithelium Think of it as a fist punched into an inflated bag

13
Histology of Renal Tubule & Collecting Duct
Proximal convoluted tubule (PCT) simple cuboidal with brush border of microvilli - increase surface area for absorption Descending limb of loop of Henle simple squamous Ascending limb of loop of Henle simple cuboidal forms juxtaglomerular apparatus (JGA) where makes contact with afferent arteriole Distal convoluted & collecting ducts simple cuboidal composed of principal & intercalated cells which have microvilli
 simple cuboidal with brush border of microvilli - increase surface area for absorption. Descending limb of loop of Henle. simple squamous. Ascending limb of loop of Henle. simple cuboidal. forms juxtaglomerular apparatus (JGA) where makes contact with afferent arteriole. Distal convoluted & collecting ducts. simple cuboidal composed of principal & intercalated cells which have microvilli.")
14
Macula densa is thickened part of ascending limb of Loop of Henle
Juxtaglomerular (JG) cells are modified muscle cells in afferent arteriole Together form Juxtaglomerular apparatus (JGA) – helps regulate blood pressure Mesangial cells – specialized smooth muscle Relaxed – increases surface area – increases filtration Contracted – decreases surface area – decreases filtration
 cells are modified muscle cells in afferent arteriole. Together form Juxtaglomerular apparatus (JGA) – helps regulate blood pressure. Mesangial cells – specialized smooth muscle. Relaxed – increases surface area – increases filtration. Contracted – decreases surface area – decreases filtration.")
15
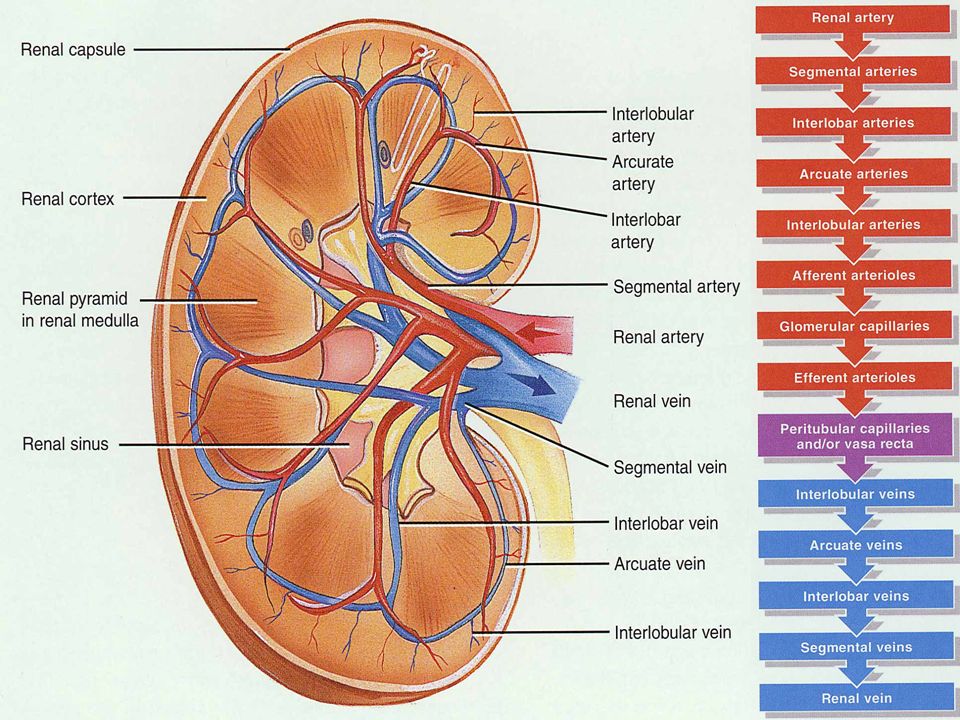
Blood Supply of Kidney Abundantly supplied with blood vessels
receive 25% of resting cardiac output via renal arteries Blood enters kidney via Renal Artery Radiate outward into renal cortex - branch off into Afferent arterioles (one per nephron) Enters nephron and becomes a ball-shaped capillary network called Glomerulus (filtration) Leaves nephron as Efferent arteriole Efferent arteriole divides to either Peritubular capillaries (Cortical nephron) or Vasa recta (Juxtamedullary nephron) Blood leaves kidney via Renal Vein
 Enters nephron and becomes a ball-shaped capillary network called Glomerulus (filtration) Leaves nephron as Efferent arteriole. Efferent arteriole divides to either Peritubular capillaries (Cortical nephron) or Vasa recta (Juxtamedullary nephron) Blood leaves kidney via Renal Vein.")
17
From Renal Artery Renal Vein

18
Summary of Renal Anatomy
2 kidneys (retroperitoneal), 2 ureters, 1 bladder, 1 urethra 3 layers – Renal capsule (deepest), Adipose capsule (intermediate), Renal Fascia (superficial) Parenchyma = Cortex + Medulla Functional portion of kidney Nephrons = functional units (cortical + juxtamedullary) Nephron: Renal (Bowman’s) capsule – parietal layer + visceral layer PCT – Simple cuboidal with microvilli Loop of Henle – Thin descending + Thick ascending DCT Collecting Duct – Principal + Intercalated cells Drainage system collects fluid from nephrons Minor calyx – Major calyx – Renal pelvis – Ureter – Bladder – Urethra Blood Supply: Renal Artery Afferent Arteriole Glomerulus Efferent Arteriole – Peritubular capillaries + Vasa recta Renal Vein
, 2 ureters, 1 bladder, 1 urethra. 3 layers – Renal capsule (deepest), Adipose capsule (intermediate), Renal Fascia (superficial) Parenchyma = Cortex + Medulla. Functional portion of kidney. Nephrons = functional units (cortical + juxtamedullary) Nephron: Renal (Bowman’s) capsule – parietal layer + visceral layer. PCT – Simple cuboidal with microvilli. Loop of Henle – Thin descending + Thick ascending. DCT. Collecting Duct – Principal + Intercalated cells. Drainage system collects fluid from nephrons. Minor calyx – Major calyx – Renal pelvis – Ureter – Bladder – Urethra. Blood Supply: Renal Artery. Afferent Arteriole. Glomerulus. Efferent Arteriole – Peritubular capillaries + Vasa recta. Renal Vein.")
19
Nephrons and collecting ducts perform 3 basic processes:
1. Glomerular filtration – water and most solutes 2. Tubular reabsorption – 99% of water and many useful solutes back into blood 3. Tubular secretion – waste, drugs, excess ions from blood to tubules

20
Glomerular Filtration
Blood pressure produces glomerular filtrate 180 litres/day filtrate produced 99% reabsorbed to blood 1-2 L/day urine Substances filtered out must cross 3 filtration barriers of the endothelial-capsular membrane: Glomerular endothelial cell fenestrations Basal lamina Pedicels of podocytes – filtration slits

21
Filtration Membrane #1 Endothelial fenestrations - Stops all cells and platelets #2 Basal Lamina - Stops large plasma proteins #3 Podocytes - Pedicels (filtration slits) - Stops medium-sized proteins
 - Stops medium-sized proteins.")
23
Endothelial-Capsular Membrane

24
3 Reasons why the volume of fluid filtered by the renal corpuscle is much larger than in other blood capillaries: Large surface area regulated by Mesangial cells. When cells are relaxed, surface area is maximal and filtration rates are high. Filtration membrane is thin and porous – 50x leakier than other blood capillaries Glomerular capillary blood pressure is high – efferent arteriole diameter is smaller than afferent arteriole.

25
Glomerular Filtration depends on 3 main pressures:
One pressure promotes filtration Two pressures oppose filtration Glomerular blood hydrostatic pressure (GBHP) – 55 mmHg Promotes filtration by forcing water and solutes through filtration membrane 2. Capsular hydrostatic pressure (CHP) – 15 mmHg Opposes filtration by exerting back pressure against filtration membrane 3. Blood colloid osmotic pressure (BCOP) – 30 mmHg Opposes filtration by the presence of proteins in blood plasma which slows down osmosis
 – 55 mmHg. Promotes filtration by forcing water and solutes through filtration membrane. 2. Capsular hydrostatic pressure. (CHP) – 15 mmHg. Opposes filtration by exerting back pressure against filtration membrane. 3. Blood colloid osmotic pressure. (BCOP) – 30 mmHg. Opposes filtration by the presence of proteins in blood plasma which slows down osmosis.")
26
Net Filtration Pressure (NFP)
GBHP = 55 mmHg - Promotes CHP = 15 mmHg - Opposes BCOP = 30 mmHg - Opposes Net Filtration Pressure (NFP) = GBHP – CHP – BCOP = 55 – = 10 mmHg Therefore, a pressure of only 10 mmHg causes a normal amount of blood plasma to filter from the glomerulus into the capsular (Bowman’s) space. Changes to either of these three pressures will affect the Glomerular Filtration Rate (GFR)
 = GBHP – CHP – BCOP. = 55 – = 10 mmHg. Therefore, a pressure of only 10 mmHg causes a normal amount of blood plasma to filter from the glomerulus into the capsular (Bowman’s) space. Changes to either of these three pressures will affect the Glomerular Filtration Rate (GFR)")
27
Glomerular Filtration Rate (GFR)
Amount of filtrate formed in all renal corpuscles of both kidneys - average adult male rate is 125 mL/min Homeostasis requires GFR to be constant too high & useful substances are lost due to the speed of fluid passing through nephron too low and sufficient waste products may not be removed from the body Three mechanisms control GFR by either (a) adjusting blood flow in/out of glomerulus (JGA) or (b) altering capillary surface area for filtrations (mesangial cells). (Table 26.2 pg. 996) Renal autoregulation Neural regulation Hormonal regulation
 adjusting blood flow in/out of glomerulus (JGA) or (b) altering capillary surface area for filtrations (mesangial cells). (Table 26.2 pg. 996) Renal autoregulation. Neural regulation. Hormonal regulation.")
28
1. Renal Autoregulation of GFR
Kidneys themselves help maintain a constant GFR despite normal, everyday changes in blood pressure (BP) Myogenic mechanism systemic increases in BP also increase GFR Increases to BP stretch the afferent arteriole smooth muscle fibers contract, reducing the diameter of the arteriole – decreasing blood flow and GFR Tubuloglomerular feedback elevated systemic BP raises the GFR - fluid flows too rapidly through the renal tubules & Na+, Cl- and water are not reabsorbed quickly enough macula densa detects that difference & inhibit release of NO (vasodilator) from the Juxtaglomerular cells afferent arterioles constrict & reduce GFR
 Myogenic mechanism. systemic increases in BP also increase GFR. Increases to BP stretch the afferent arteriole. smooth muscle fibers contract, reducing the diameter of the arteriole – decreasing blood flow and GFR. Tubuloglomerular feedback. elevated systemic BP raises the GFR - fluid flows too rapidly through the renal tubules & Na+, Cl- and water are not reabsorbed quickly enough. macula densa detects that difference & inhibit release of NO (vasodilator) from the Juxtaglomerular cells. afferent arterioles constrict & reduce GFR.")
29
Tubuloglomerular feedback:
Myogenic mechanism: Increase in BP stretches walls of Afferent arteriole Smooth muscles in vessel walls contract Blood flow decreases which lowers GFR Tubuloglomerular feedback: Macula densa detect changes to filtrate Inhibit release of NO (potent vasodilator) by Juxtaglomerular cells Afferent arteriole contracts
 by Juxtaglomerular cells. Afferent arteriole contracts.")
30
3. Hormonal Regulation of GFR
Two hormones contribute to regulation of GFR: Atrial natriuretic peptide (ANP) – increases Angiotensin II – decreases Atrial Natriuretic Peptide (ANP): stretching of the atria that occurs with an increase in blood volume causes cells of atria to release ANP relaxes glomerular Mesangial cells, therefore increasing capillary surface area and increasing GFR Angiotensin II: Release stimulated by decrease in blood volume/pressure Enzyme Renin secreted by juxtaglomerular cells potent vasoconstrictor that narrows both afferent & efferent arterioles decreasing GFR
 – increases. Angiotensin II – decreases. Atrial Natriuretic Peptide (ANP): stretching of the atria that occurs with an increase in blood volume causes cells of atria to release ANP. relaxes glomerular Mesangial cells, therefore increasing capillary surface area and increasing GFR. Angiotensin II: Release stimulated by decrease in blood volume/pressure. Enzyme Renin secreted by juxtaglomerular cells. potent vasoconstrictor that narrows both afferent & efferent arterioles decreasing GFR.")
31
Summary of Filtration Occurs in Renal Corpuscle
Substances filtered across 3 filtration barriers (endothelial-capsular membrane): Glomerular endothelial cell – fenestrations make it very porous (leaky) Basal lamina Pedicels of podocytes – filtration slits Filtration is dependent on 3 pressures: Glomerular blood hydrostatic pressure (GBHP) - promotes Capsular hydrostatic pressure (CHP) - opposes Blood colloid osmotic pressure (BCOP) – opposes Net Filtration Pressure = GBHP – CHP – BCOP Determines Glomerular Filtration Rate (GFR) Must remain constant GFR regulated by 3 mechanisms Renal Autoregulation : Myogenic mechanism Tubulogomerular feedback Neural Regulation – ANS – “Fight or Flight” Hormonal Regulation Angiotensin II – Decreases GFR Atrial natriuretic peptide (ANP) – Increases GFR
: Glomerular endothelial cell – fenestrations make it very porous (leaky) Basal lamina. Pedicels of podocytes – filtration slits. Filtration is dependent on 3 pressures: Glomerular blood hydrostatic pressure (GBHP) - promotes. Capsular hydrostatic pressure (CHP) - opposes. Blood colloid osmotic pressure (BCOP) – opposes. Net Filtration Pressure = GBHP – CHP – BCOP. Determines Glomerular Filtration Rate (GFR) Must remain constant. GFR regulated by 3 mechanisms. Renal Autoregulation : Myogenic mechanism. Tubulogomerular feedback. Neural Regulation – ANS – Fight or Flight Hormonal Regulation. Angiotensin II – Decreases GFR. Atrial natriuretic peptide (ANP) – Increases GFR.")
32
1. Glomerular filtration – water and most solutes
2. Tubular reabsorption – 99% of water and many useful solutes back into blood 3. Tubular secretion – waste, drugs, excess ions from blood to tubules

33
Tubular reabsorption Paracellular reabsorption
Epithelial cells all along the renal tubules and collecting duct carry out reabsorption Proximal convoluted tubules (PCT) make largest contribution More distal tubule cells fine-tune reabsorption to maintain homeostasis Paracellular reabsorption 50% of reabsorbed material moves between cells by diffusion in some parts of tubule Transcellular reabsorption material moves through both the apical and basolateral membranes of the tubule cell
 make largest contribution. More distal tubule cells fine-tune reabsorption to maintain homeostasis. Paracellular reabsorption. 50% of reabsorbed material moves between cells by diffusion in some parts of tubule. Transcellular reabsorption. material moves through both the apical and basolateral membranes of the tubule cell.")
34
Reabsorption in the PCT
Largest amount of solute and water reabsorption occurs in PCT 65% of filtered water, Na+ and K+ 100% of glucose and amino acids 80-90% of HCO3 Most solute reabsorption in PCT involves Na+ Water is only reabsorbed by osmosis: obligatory water reabsorption occurs when water is “obliged” to follow the solutes being reabsorbed facultative water reabsorption occurs in collecting duct under the control of antidiuretic hormone (ADH)
")
35
Reabsorption of Glucose in PCT
Intracellular sodium levels are kept low due to Na+/K+ ATPase pump on basolateral membrane Low intracellular Na+ creates concentration gradient high in filtrate – low in cell Na+ symporters on apical membrane use energy from gradient to bring in glucose Secondary active transport 2 Na+ and 1 glucose attach to symporter and enter cell together Glucose then diffuses out of cell and into peritubular capillaries

36
Reabsorption of Bicarbonate & H+ ion secretion in PCT
CO2 + H2O H2CO HCO3- + H+

37
Reabsorption within Loop of Henle
Osmolarity of interstitial fluid progressively increases deeper into the medulla Descending loop is highly permeable to water. Water moves by osmosis out of the tubule (15% of total reabsorption) increasing filtrate concentration Thick ascending loop has many Na+, K+ and Cl- transporters. Ions pass out of filtrate and into intersitital fluid (20-30% total reabsorption) These cells are also impermeable to water, so water does not follow osmotically. Therefore decreasing concentration/osmolarity of filtrate This osmotic gradient is how the kidneys are able to produce concentrated or dilute urine.
 increasing filtrate concentration. Thick ascending loop has many Na+, K+ and Cl- transporters. Ions pass out of filtrate and into intersitital fluid (20-30% total reabsorption) These cells are also impermeable to water, so water does not follow osmotically. Therefore decreasing concentration/osmolarity of filtrate. This osmotic gradient is how the kidneys are able to produce concentrated or dilute urine.")
38
Reabsorption in Early DCT Reabsorption in late DCT & Collecting Ducts
Absorb 10-15% of water and 5% of Na+ and Cl- Also where parathyroid hormone (PTH) stimulates reabsorption of Ca2+ depending on body’s needs. Reabsorption in late DCT & Collecting Ducts By end of DCT, 95% of solutes & water have been reabsorbed and returned to the bloodstream Cells in the collecting duct make the final fine tuning adjustments: principal cells reabsorb Na+ and secrete K+; facultative reabsorption of H2O (ADH) intercalated cells reabsorb K+ & bicarbonate ions (HCO3) and secrete H+ (regulate pH) Hormonally controlled by Angiotensin II, Aldosterone, Atrial natriuretic peptide (ANP) , Antidiuretic hormone (ADH) and Parathyroid hormone
 stimulates reabsorption of Ca2+ depending on body’s needs. Reabsorption in late DCT & Collecting Ducts. By end of DCT, 95% of solutes & water have been reabsorbed and returned to the bloodstream. Cells in the collecting duct make the final fine tuning adjustments: principal cells reabsorb Na+ and secrete K+; facultative reabsorption of H2O (ADH) intercalated cells reabsorb K+ & bicarbonate ions (HCO3) and secrete H+ (regulate pH) Hormonally controlled by Angiotensin II, Aldosterone, Atrial natriuretic peptide (ANP) , Antidiuretic hormone (ADH) and Parathyroid hormone.")
39
Angiotensin II and Aldosterone
When blood volume/pressure drop – JG cells secrete renin Renin helps convert angiotensin I – angiotensin II (active) decreases GFR by vasoconstricting afferent arteriole enhances absorption of Na+, Cl- and water in PCT promotes aldosterone production (adrenal gland) which causes principal cells to reabsorb more Na +,Cl-, and water increases blood volume/pressure by increasing water reabsorption Atrial Natriuretic Peptide (ANP) Stimulated by large increase in blood volume inhibits reabsorption of Na + and water in PCT & suppresses secretion of aldosterone & ADH increase excretion of Na + into tubules (obligated water) which increases urine output and decreases blood volume
 decreases GFR by vasoconstricting afferent arteriole. enhances absorption of Na+, Cl- and water in PCT. promotes aldosterone production (adrenal gland) which causes principal cells to reabsorb more Na +,Cl-, and water. increases blood volume/pressure by increasing water reabsorption. Atrial Natriuretic Peptide (ANP) Stimulated by large increase in blood volume. inhibits reabsorption of Na + and water in PCT & suppresses secretion of aldosterone & ADH. increase excretion of Na + into tubules (obligated water) which increases urine output and decreases blood volume.")
40
Antidiuretic Hormone (ADH)
Released by posterior pituitary Stimulated by an increased plasma osmolarity or a decrease in blood volume (hemorrhage) Stimulates the insertion of aquaporin-2 channels into the apical membrane of principal cells of late DCT and collecting duct– greatly increases permeability of cells and reabsorption of water from filtrate (concentrated urine) In absence of ADH, principal cells of DCT and collecting ducts are impermeable to water – no water is reabsorbed therefore increasing urine output (dilute urine) Diabetes insipidus – lack of ADH or insensitive to it excrete 20L urine/day
 Stimulates the insertion of aquaporin-2 channels into the apical membrane of principal cells of late DCT and collecting duct– greatly increases permeability of cells and reabsorption of water from filtrate (concentrated urine) In absence of ADH, principal cells of DCT and collecting ducts are impermeable to water – no water is reabsorbed therefore increasing urine output (dilute urine) Diabetes insipidus – lack of ADH or insensitive to it. excrete 20L urine/day.")
41
Breaking The Seal Alcohol inhibits release of ADH
Without ADH, DCT and collecting ducts are impermeable to water Kidneys can’t reabsorb needed water – instead produce copious amounts of dilute urine Effects of alcohol linger long after you stop drinking – leaving you feeling dehydrated

42
Summary – Absorption & Secretion

Similar presentations
















. Other excretory.>")


