Download presentation
Presentation is loading. Please wait.

1
1 May 2013 Dr Samantha Russell

2
1. Autoimmune Disorders 2.Cardiovascular Disease 3. Endocrine Disorders 4. Hematologic and Coagulation Disorders 5. Human immunodeficiency virus 6. Hypertensive Disorders 7. Liver Disease 8. Malignant Hyperthermia 9. Musculoskeletal Disorders 10. Neurologic and Neuromuscular Disease 11. Obesity 12. Renal Disease 13. Respiratory Disease 14. Substance Abuse 15. Trauma The parturient with systemic disease

3
Failure of self-tolerance Systemic lupus erythematosus Antiphospholipid syndrome Systemic sclerosis (scleroderma) Polymyositis and dermatomyositis Autoimmune disorders
 Polymyositis and dermatomyositis Autoimmune disorders")
4
Production of autoantibodies causing an immune complex disorder 1/700 women with peak incidence at around age 30

5
Presence of 4 or more of criteria:- Malar rash Discoid rash Photosensitivity Oral ulceration Arthritis Serositis Renal disorder Neurologic disorder Hematologic disorder Immunologic disorder Antinuclear antibody Diagnosis of SLE (1997)
")
6
often patients have increased disease activity, most often during the 2 nd, 3 rd trimesters & puerperium Maternal effects - mortality prevalence about 0.05% Fetal effects Loss -> obstetric history is a strong predictor of outcome in subsequent pregnancies Pregnancy loss is increased with renal involvement and hypertension Increased risk of preterm delivery Neonatal lupus erythematosus (NLE) – reversible and irreversible manifestations
 – reversible and irreversible manifestations")
7
Medical Ideally delay pregnancy until disease has been quiet for at least 6 months Hydroxychloroquine & azathioprine should be continued Mycophenolate mofetil should be discontinued Low dose prednisone (<20mg daily) appears to be safe watch for gestational diabetes Manage complications of SLE Preeclampsia is more common (reviews quote 20-30% incidence) Obstetric Should be considered high-risk Measure Cr Cl, 24-hour urine protein level and anti-Ro/anti-La antiboides Thromboprophylaxis if antiphospholipid syndrome Monitor for preeclampsia Platelet count to be repeated monthly Management
 appears to be safe watch for gestational diabetes Manage complications of SLE Preeclampsia is more common (reviews quote 20-30% incidence) Obstetric Should be considered high-risk Measure Cr Cl, 24-hour urine protein level and anti-Ro/anti-La antiboides Thromboprophylaxis if antiphospholipid syndrome Monitor for preeclampsia Platelet count to be repeated monthly Management")
8
is a prothrombotic disorder that results in both arterial and venous thrombosis and is characterised by the presence of two autoantibodies, lupus anticoagulant and anticardiolipin antibody Lupus anticoagulant has no true anticoagulant activity in vivo but appears to block in vitro assembly of prothrombinase ( a phospholipid complex) thus preventing the conversion of prothrombin to thrombin The current model for thrombotic tendency involves antiphospholipid antibodies binding to glycoproteins on platelets, monocytes and endothelial cells. These complexes cause platelet adhesion, expression of prothrombotic molecules and local complement activation Antiphospholipid syndrome

9
Modified Sapporo classification criteria or Sydney criteria (2006) – by the presence of 2 major components, one clinical and the other a laboratory finding.
 – by the presence of 2 major components, one clinical and the other a laboratory finding.")
10
Maternal Thromboembolic disease Thrombocytopenia Antiphospholipid syndrome Fetal placental infarction may increase risk for death in utero Effects

11
ACOG 2005: women with antiphospholipid syndrome and no thrombotic history should receive prophylactic doses of heparin and low-dose aspirin during pregnancy and 6-8 weeks postpartum if thrombotic history should receive full anticoagulation throughout pregnancy and postpartum period. Treatment

12
Antiphospholipid antibodies can cause coagulation factor deficiencies. In such patients neuraxial anaesthesia (NA) is relatively contra-indicated. In the absence of an underlying coagulation deficit or anticoagulation therapy, the prolonged aPTT does NOT suggest bleeding tendency, and NA may be administered Anaesthetic management
 is relatively contra-indicated. In the absence of an underlying coagulation deficit or anticoagulation therapy, the prolonged aPTT does NOT suggest bleeding tendency, and NA may be administered Anaesthetic management.")
13
Chronic progressive autoimmune disease of unknown aetiology characterised by deposition of fibrous connective tissue in the skin and other tissues. A heterogeneous disorder that is separated into limited cutaneous scleroderma ( also termed CREST syndrome) and diffuse cutaneous scleroderma. Multidisciplinary approach required Systemic sclerosis (scleroderma) Lidar M, Langevitz P. Pregnancy issues in scleroderma. Autoimmunity reviews 2012 (11) A515-519
 and diffuse cutaneous scleroderma. Multidisciplinary approach required Systemic sclerosis (scleroderma) Lidar M, Langevitz P. Pregnancy issues in scleroderma. Autoimmunity reviews 2012 (11) A")
14
Triad of Raynaud’s phenomenon, non-pitting oedema, and hidebound skin. Diagnosis

15
Maternal Difficult airway Thrombocytopenia Scleroderma renal crisis Fetal Miscarriages and prematurity small full-term infants Complications

16
Cardiovascular System

17
ParameterChange Cardiac output+50% Stroke volume+25% Heart rate+25% Left ventricular end-diastolic volumeIncreased Left ventricular end-systolic volumeNo change Ejection fractionIncreased Left ventricular stroke work indexNo change Pulmonary capillary wedge pressureNo change Pulmonary artery diastolic pressureNo change Central venous pressureNo change Systemic vascular resistance-20% Central Hemodynamics at term gestation

18
Congenital Heart Disease Primary pulmonary hypertension Cardiomyopathy Hypertrophic obstructive cardiomyopathy Peripartum cardiomyopathy Ischemic heart disease Valvular disorders Transplanted heart Arrhythmias Diseases of the Aorta Infective endocarditis Cardiovascular Disease

19
Estimated prevalence of clinically significant cardiac disease in pregnancy is <1%, yet is the most important cause of nonobstetric maternal morbidity and mortality in the United States Significant morbidity in pulmonary HTN, Eisenmenger’s syndrome, and severe cases of Marfan’s syndrome Maternal outcomes correlate with NYHA functional classification

20
If complete repair and normal cardiovascular function require no special treatment If shunts: avoid air bubbles in IV lines, use LOR to saline in epidural rather than air, early administration of labour analgesia, maintain balance of PVR and SVR Congenital heart disease

21
Among women with valvular heart disease, those with mitral stenosis carry the greatest potential for problems during pregnancy. Asymptomatic women with aortic stenosis and only mild or moderate LV outflow obstruction generally tolerate pregnancy well, as do those with regurgitant lesions In Marfan ‘s syndrome, pregnancy should not be undertaken if the aortic root dimension exceeds 4 cm. Even if the aortic root is normal, a small increased risk of dissection is present Women with well-functioning bioprosthetic valves and normal hemodynamics may safely undertake a pregnancy. Bioprostheses deteriorate rapidly in young people, and therefore preconception counseling should be kept under frequent review. Valvular heart disease and pregnancy Trail TA. Cardiol Clin 30 (2012) 369-381
")
23
Preload: avoid aortocaval compression, maintain intravascular volume and venous return Afterload: maintain adequate SVR Contractility: Avoid myocardial depression during GA Heart rate: maintain normal HR Rhythm: maintain sinus rhythm Right side of heart Goals of anaesthetic management in patients with aortic stenosis

24
Maintain normal to slightly elevated HR Prevent an increase in SVR Avoid myocardial depression during GA ~ Aortic regurgitation

25
Aggressively treat acute AF Maintain venous return Maintain adequate SVR Right side of heart: prevent pain, hypoxemia, hypercarbia, and acidosis, which may increase PVR ~ Mitral stenosis

26
Prevent an increase in SVR Maintain a normal to slightly elevated HR (ephedrine) Aggressively treat AF (cardioversion/anticoagulate) Maintain venous return Prevent an increase in central vascular volume Avoid myocardial depression during GA Right side of heart: Prevent increase in PVR ~ Mitral regurgitation
 Aggressively treat AF (cardioversion/anticoagulate) Maintain venous return Prevent an increase in central vascular volume Avoid myocardial depression during GA Right side of heart: Prevent increase in PVR ~ Mitral regurgitation")
27
Most common cardiac condition 12-17% of women of childbearing age Primary/idiopathic MVP or secondary and associated with ASD, endocarditis or MS Prognosis depends on coexisting CVS disease Beta-adrenergic receptor antagonists may be necessary to treat arrhythmias, chest pain and palpitations Progressive MR occurs in approximately 15% of patients with MVP Mitral valve prolapse

28
Organic heart diseaseNormal CVS status Rule out other causes Treat underlying cause, drug therapy only if arrhythmias are symptomatic or threatening to mother or fetus Treat underlying disease Drug therapy only if arrhythmia persists and use smallest dosage required Use drugs known as safe to fetus Re-evaluate periodically Cardiac arrhythmia

29
In women of reproductive age the commonest arrhythmia is paroxysmal SVT Defined as any tachyarrhythmia with a HR >120bpm, requiring atrial or atrioventricular junctional tissue for its initiation and maintenance. Paroxysmal describes an arrhythmia that begins and ends abruptly. Atrioventricular nodal re-entry and Wolf-Parkinson White syndrome account for the majority of SVT Robins K, Lyons G. Supraventricular tachycardia in pregancy. 2004. BJA 92 (1): 140-3 Paroxysmal supraventricular tachycardia (SVT)
: Paroxysmal supraventricular tachycardia (SVT).")
30
Pregnancy is a risk factor for paroxysmal SVT. Result of hemodynamic, hormonal, autonomic, and emotional changes. An expanded circulating volume may increase myocardial irritability and a faster sinus heart rate may alter tissue excitability, initiating a re-entry circuit. Peripartum oxytocin, tocolytic and anaesthetic drugs have also been suggested as triggers for inducing SVT

31
Differential diagnosis includes acute myocardial infarction (AMI) aortic dissection and aortic syndromes pulmonary embolism amniotic fluid embolism Sahni G, Chest Pain Syndromes in Pregnancy. Cardiol Clin 30 (2012) 343-367 Chest pain syndromes in pregnancy
 Chest pain syndromes in pregnancy.")
32
ParameterEffect of pregnancy Supply Diastolic timeDecreased CPPDecreased Arterial oxygen content Arterial oxygen tensionIncreased Haemoglobin concentrationDecreased Coronary vessel diameterUnchanged Demand Basal oxygen requirementIncreased Heart rateIncreased Wall tension Preload (ventricular radius)Increased AfterloadDecreased Contractilityincreased Balance between myocardial oxygen supply and demand during pregnancy
Increased AfterloadDecreased Contractilityincreased Balance between myocardial oxygen supply and demand during pregnancy")
33
Sahni G, Chest Pain Syndromes in Pregnancy. Cardiol Clin 30 (2012) 343-367
")
34
Endocrine System

35
Diabetes Mellitus Thyroid disorders Pheochromocytoma Biggar MA, Lennard TWJ. Systemic review of phaeochromocytoma in pregnancy. British Journal of Surgery 2013; 100:182-190 Endocrine Disorders

36
Major complications of diabetes mellitus Acute DKA Hyperglycemic nonketotic state hypoglycemia Chronic Macrovascular Coronary Cerebrovascular Peripheral vascular Microvascular Retinopathy nephropathy Neuropathy Autononic somatic Diabetes Mellitus

37
Hyperthyroidism (0.2-1.9%) Abnormal thyroid stimulator Graves Disease (70-90%) Intrinsic thyroid autonomy Toxic adenoma Inflammatory disease Subacute thyroiditis Extrinsic hormone source Ectopic thyroid tissue Thyroid hormone ingestion Thyroid disorders
 Abnormal thyroid stimulator Graves Disease (70-90%) Intrinsic thyroid autonomy Toxic adenoma Inflammatory disease Subacute thyroiditis Extrinsic hormone source Ectopic thyroid tissue Thyroid hormone ingestion Thyroid disorders")
38
Labwork Hyperthyroid symptom scale developed on the basis of the following clinical factors: Nervousness Sweating Heat intolerance Hyperactivity Tremor Weakness Hyperdynamic precordium Diarrhoea Appetite Level of incapacitation Diagnosis

39
General supportive measures Cooling blanket and ice Chlorpromazine (25-50mg IV) or meperidine (25-50mg IV) to diminish shivering Intravenous hydration Glucose and electrolyte replacement Oxygen Glucocorticoids: dexamethasone (2-4mg IV 8hr) or hydrocortisone (100mg IV q8hr) B complex vitamins Reduction of synthesis and secretion of thyroid hormone Antithyroid med: PTU 200-400mg po 6-8hrly, methimazole 20-25mg po q 6hrly Iodine: sodium iodide (1g IV) or lugol’s solution 4-8drops orally 6-8hr) after PTU glucocorticoids Reduction of peripheral conversion of T4 to T3 Antithyroid medication Glucocorticoids Radiographic contrast agents propanolol Decrease in metabolic effects of thyroid hormones: B-blockers Other therapeutic manoeuvres: plasma exchange, dantrolene Dx and rx of the underlying illness that precipitated the thyroid storm Treatment of thyroid storm
 or meperidine (25-50mg IV) to diminish shivering Intravenous hydration Glucose and electrolyte replacement Oxygen Glucocorticoids: dexamethasone (2-4mg IV 8hr) or hydrocortisone (100mg IV q8hr) B complex vitamins Reduction of synthesis and secretion of thyroid hormone Antithyroid med: PTU mg po 6-8hrly, methimazole 20-25mg po q 6hrly Iodine: sodium iodide (1g IV) or lugol’s solution 4-8drops orally 6-8hr) after PTU glucocorticoids Reduction of peripheral conversion of T4 to T3 Antithyroid medication Glucocorticoids Radiographic contrast agents propanolol Decrease in metabolic effects of thyroid hormones: B-blockers Other therapeutic manoeuvres: plasma exchange, dantrolene Dx and rx of the underlying illness that precipitated the thyroid storm Treatment of thyroid storm")
40
Hematologic and coagulation systems

41
Anemia Coagulation Thrombocytopenic coagulopathies Congenital coagulopathies Acquired coagulopathies Hypercoagulable states Hematologic and coagulation disorders

42
Dilutional anemia of pregnancy Thalassemia Sickle cell disease Autoimmune hemolytic anaemia Anemia

43
Autoimmune thrombocytopenic purpura Thrombotic thrombocytopenic purpura Drug-induced platelet disorders Gestational thrombocytopenia Thrombocytopenic coagulopathies

44
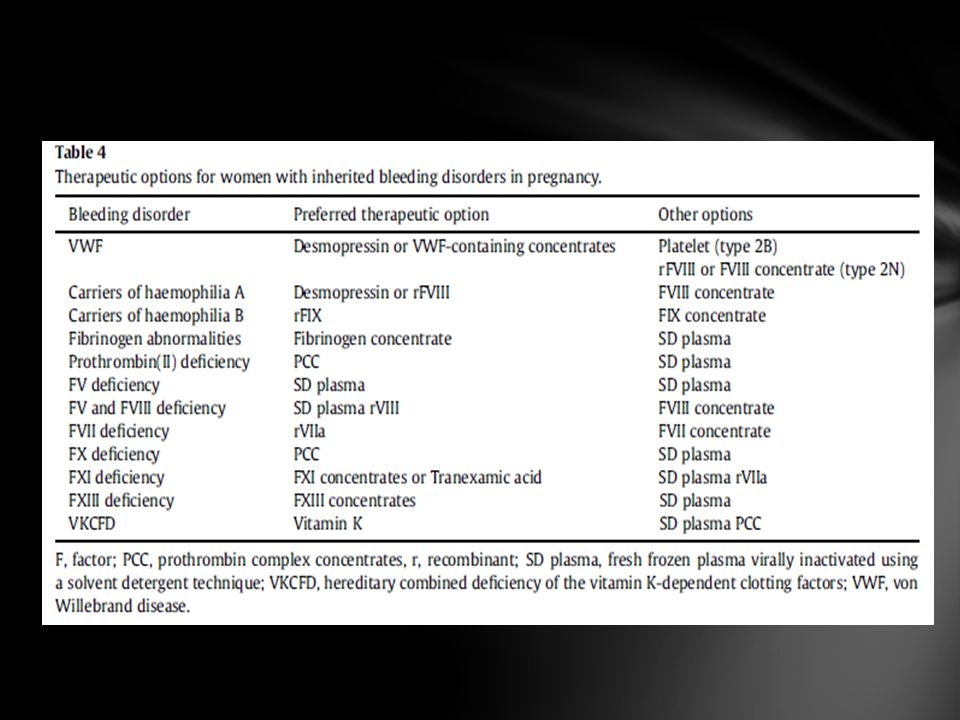
Prenatal diagnosis only considered in severe bleeding disorders such as hemophilia Besides fibrinogen and Factor XIII deficiencies unclear whether there is increased pregnancy loss and APH But all are increased risk of PPH Von Willebrand’s disease and carriers of hemophilia account for the majority of inherited bleeding disorders in women Congenital coagulopathies: bleeding disorders

45
1% of population Von Willebrand’s disease

46
X-linked recessive disease Women mainly carriers and expected to have 50% of normal clotting factor level Wide variation of levels have been reported though due to lyonisation and some women may have low levels of factor Factor 8 levels increase progressively in Haemophilia A carriers during pregnancy reaching peak in 3 rd trimester. Most carriers of haemophilia A have normal (>50IU/dL) F8 levels at term. In contrast, F9 levels do not increase significantly during pregnancy.. Haemophilia A & B
 F8 levels at term. In contrast, F9 levels do not increase significantly during pregnancy.. Haemophilia A & B.")
47
Gender can be determined from 11 weeks gestation to avoid invasive diagnostic tests if requested by parents Multidisciplinary approach with early recognition

49
Bleeding disorder is not an indication for abdominal delivery Neuraxial anaesthesia not a contra-indication if normal coagulation and factor levels. Very little evidence with risk and safety Avoid prolonged labour, mid-forceps delivery, fetal scalp monitoring or blood sampling, vacuum extraction and intramuscular injections Active management of 3 stage

50
Human immunodeficiency virus (HIV)
")
51
“window period” Comorbid disease and substance abuse Transmission of the disease in nonbreast-fed infants occurs 30% of the time in utero and 70% during labour and delivery Impaired cell-mediated (humoral) immunity, causes infected person to be more susceptible to viral, bacterial, mycobacterial and malignant disease *Peripheral neuropathy is the most frequent neurological complication in HIV patients. Affects approximately 35% of patients with AIDS and manifests clinically as polyneuropathy and myopathy. Autonomic dysfunction in the HIV-infected person may appear with or without CNS abnormalities. AIDS patients may present with uncommon autonomic disturbances, such as orthostatic syncope, hypotension and diarrhea. Coagulation abnormalities include ITP Review article: Human Immunodeficiency Virus: Anesthetic and obstetric considerations. Evron S et al. Anesth Analg 2004;98:503-11 HIV

52
Surgical interventions do not increase the postoperative risk for complications or death. CNS HIV infection has occurred in asymptomatic patients therefore not a contra-indication for NA. Regional anesthesia is often technique of choice Take into consideration the presence of neuropathies, local infection, or blood clotting abnormalities Patients with AIDS are more sensitive to opioids and benzodiazepines* Adverse reactions of HAART No evidence that pregnancy accelerates clinical deterioration or that viral RNA load changes significantly PEP prophylaxis Management

53
JOGC Volume 30, number 3, march 2008 Diagnosis, evaluation and management of the hypertensive disorders of pregnancy Hypertension

54
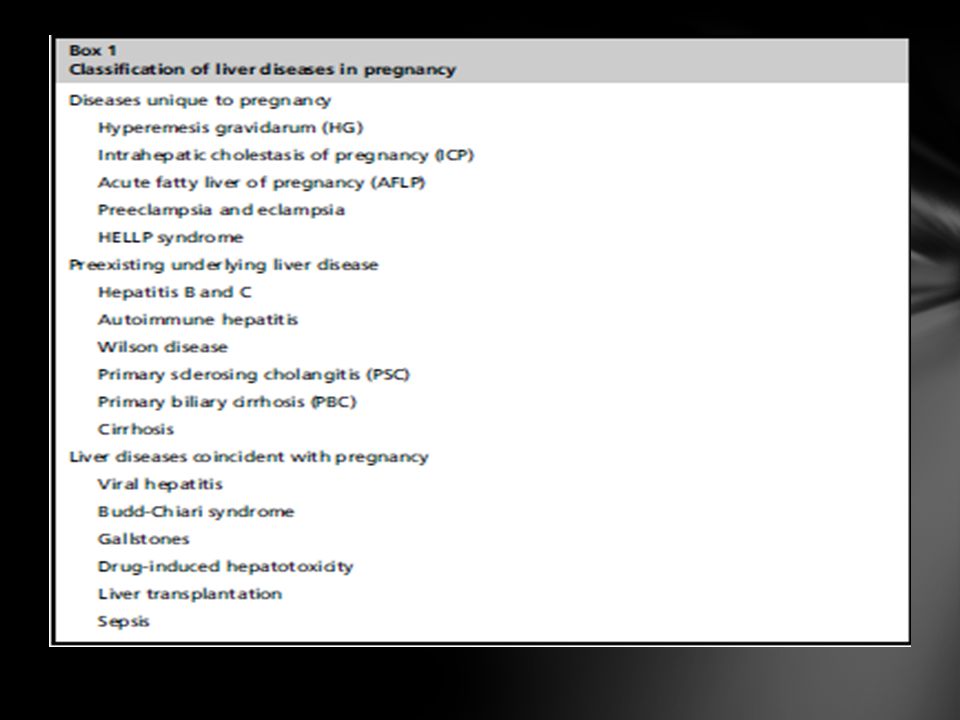
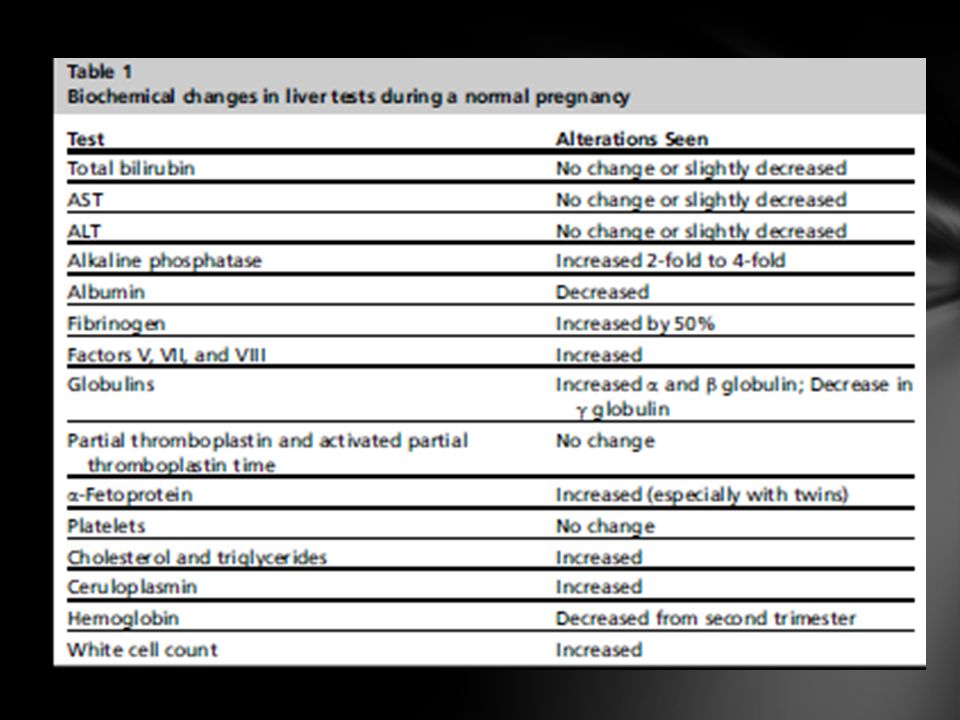
Viral hepatitis Intrahepatic cholestasis of pregnancy Acute fatty liver of pregnancy Spontaneous hepatic rupture of pregnancy Portal hypertension Liver transplantation Anesthetic management of the parturient with liver disease Liver Disease

55
Mufti AR, Reau N. Clin Liver Dis 16(2012) 247-269 Liver disease in pregnancy
 Liver disease in pregnancy")
58
Scoliosis Rheumatoid arthritis Ankylosing spondylitis Spina bifida Achondroplasia Osteogenesis imperfecta spondylolisthesis Musculoskeletal disorders

59
Spina bifida occulta is defined as failed fusion of the neural arch without herniation of the meninges or neural elements Spina bifida cystica is defined as failed closure of the neural arch with herniation of the meninges (or together with neural elements) !tethered cord syndrome (TCS) Occult spinal dysraphism where the bony defect is associated with > 1 anomalies of the spinal cord Spina Bifida
 !tethered cord syndrome (TCS) Occult spinal dysraphism where the bony defect is associated with > 1 anomalies of the spinal cord Spina Bifida")
60
Should avoid both the squatting position and prolonged lithotomy position Epidural: higher incidence of dural puncture If occult spinal dysraphism – neurological history, MRI What type of neuraxial technique? Management of women with known TCS

61
Multiple sclerosis Headache Spinal cord injury Myasthenia gravis Epilepsy Myotonia and myotonic dystrophy Muscular dystrophy Neurocutaneous syndromes Landry-Guillain-Barre syndrome Polio Brain neoplasms Idiopathic intracranial hypertension Maternal hydrocephalus with shunt Intracerebral hemorrhage Cerebral vein thrombosis Motor neuron disorders Isolated mononeuropathies during pregnancy Neurologic and neuromuscular disease

62
Epilepsy is one of the most common neurological disorders in childbearing age with a prevalence of 0.3-0.7% in pregnant women Risk of seizures in pregnancy was reduced by 50-70% once there had been 1 year’s freedom from seizures before pregnancy. Polytherapy gave the highest incidence of congenitial malformations. Valproate treatment was associated with the highest incidence of malformed infants. Lamotrigine has the lowest rate Pregnancy complications in patients with epilepsy Borthen I, Gikhus NE. Curr opin obstet gynecol 2012 24:78-83

63
Planned pregnancy by optimizing antiepileptic drugs versus the seizure and obstetric complication risks. Unclear if there is an increased risk of pregnancy complications some studies report increased risks of preeclampsia, gestational hypertension and preterm birth in patients with epilepsy Management

64
?surgical repair HD stability NA techniques No definite advantage of certain delivery. If vaginal reduce 2 nd stage and attenuate blood pressure fluctuations Management of aneurysms and AVMS

66
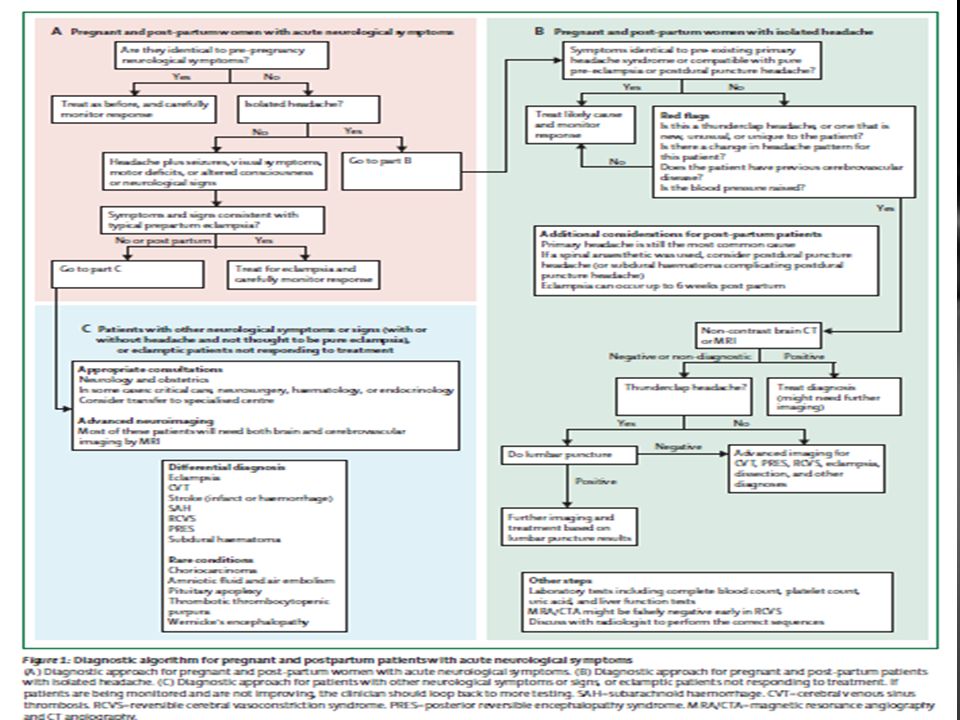
40% of post-partum women have headaches often within the first week after delivery

69
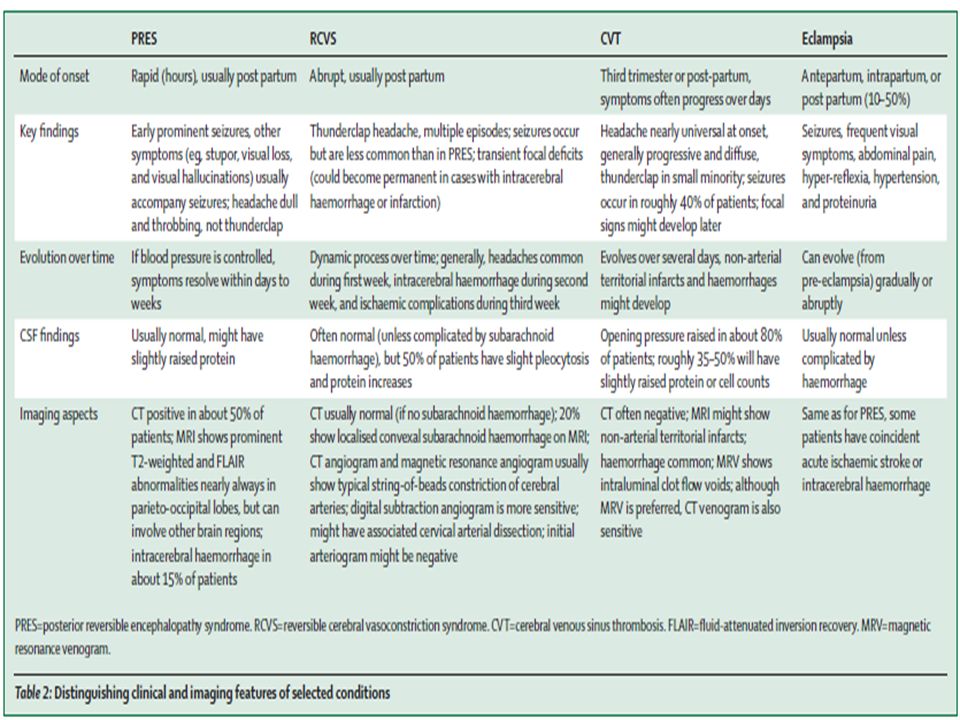
Difference between pituitary apoplexy and Sheehan’s syndrome?

70
Renal parenchymal disease Acute renal failure Renal transplant urolithiasis Renal Disease

71
Respiratory System

72
ParameterChange relative to non-pregnant state Diaphragm excursionIncreased Chest wall excursionDecreased Pulmonary resistanceDecreased 50% FEV 1 No change FEV 1 /FVCNo change Flow-volume loopNo change Closing capacityNo change Effects of pregnancy on respiratory mechanics and physiology

73
ParameterChange relative to non-pregnant state Lung volumes: Inspiratory reserve volume+5% Tidal volume+45% Expiratory reserve volume-25% Residual volume-15% Lung capacities: Inspiratory capacity+15% Functional residual capacity-20% Vital capacityNo change Total lung capacity-5% Dead space+45% Respiratory rateNo change Ventilation: Minute ventilation+45% Alveolar ventilation+45%

74
Asthma Cigarette smoking Cystic fibrosis Respiratory failure Respiratory disease

75
Most common medical conditions, 4-8% of pregnancies 1/3 of women will experience a worsening of asthma control, 1/3 will improve and the remaining 1/3 will remain unchanged during pregnancy Asthma McCallister JW. Asthma in pregnancy: management strategies. Curr Opin Pulm Med. 2003; 19:13-17

76
Younger age Unmarried Lower socioeconomic status Obesity Smokers Women with asthma have been shown to be more likely to have URTIs and UTIs during pregnancy Risk factors for exacerbations

77
Perception of teratogenic risks of asthma medications may influence a patients decision to continue therapy with better compliance if the obstetrician says it will be safe to continue meds. Spirometry and peak expiratory flow rates are useful objective tools for monitoring PFTs as they are unaffected by gestation, and routine measurement is recommended. Fraction of exhaled nitric oxide has been evaluated as a tool for assessing eosinophilic airway inflammation in asthma. Management

78
The End

Similar presentations









 LECTURE Dr. Essam H. Jiffri.>")








 F.R.C.P. (E) F.R.C.P. (LONDON) F.A.C.C Designed At A.V. Dept. F.J.M.C. By.>")
