Download presentation
Presentation is loading. Please wait.

1
Brain waves or brain drain Interactive case discussion Dr Jenny Vaughan and Dr Richard Perry Charing Cross Hospital Hammersmith Hospital Imperial College

2
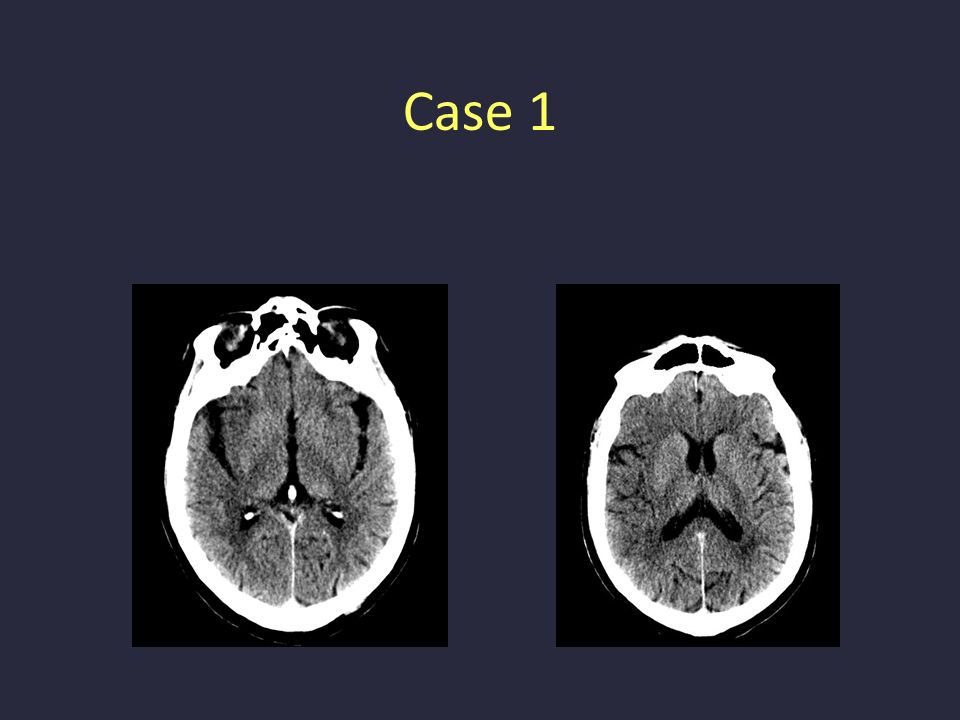
Case 1 68yr old lady Well on going to bed at 11pm Woke up at 5am with right sided arm and leg weakness and aphasia A&E 7 am NIHSS 12, BP 165/105 Out of CT scanning 7.30

3
Case 1 - CT brain What do we do now?

4
Case 1 Patient thrombolysed at 07.40 am Speech improved by 10 minutes after initiation of thrombolysis Arm and leg weakness improved at 1hr 2hr NIHSS score 3

5
Note time of onset of stroke Published evidence suggests that outcomes good if thrombolysed inside guidelines Technically thrombolysed outside of current guidelines Case 1

6
Thrombolysing outside guidelines > 3 hrs – – ECASS III (3-4.5 hrs) and IST III (3-6 hrs) –May benefit from ‘penumbral imaging’ > 80 years –No increased risk of haemorrhage but 3 X higher 3 month mortality Posterior circulation stroke –Not in ECASS trials, often don’t score enough on NIHSS –Note benefit for basilar artery thrombosis Improving symptoms –Most TIAs less than 30 minutes –1/3 of those who improve, then have severe deterioration Cervical artery dissection –> 50 pts reported – seems safe Hyperglycaemia –Increased ICH rate over 8.4 mmol/L, 25% > 11.1 mmol/L
 and IST III (3-6 hrs) –May benefit from ‘penumbral imaging’ > 80 years –No increased risk of haemorrhage but 3 X higher 3 month mortality Posterior circulation stroke –Not in ECASS trials, often don’t score enough on NIHSS –Note benefit for basilar artery thrombosis Improving symptoms –Most TIAs less than 30 minutes –1/3 of those who improve, then have severe deterioration Cervical artery dissection –> 50 pts reported – seems safe Hyperglycaemia –Increased ICH rate over 8.4 mmol/L, 25% > 11.1 mmol/L")
7
Case 1 By 15.00 speech slightly worse Re-scanned Now what do we do?

8
Heparinised Improved again Case 1

9
Heparin in acute stroke The evidence: –Lack of large formal trial of standard dose IV heparin –Small studies of IV heparin, sc heparin, sc tinzaparin, IV danaparoid failed to show overall advantage ( haemorrhage) –Cochrane review (2000) suggested no benefit –ESPRIT trial 2007 - warfarin vs aspirin in non- cardioembolic stroke w/o leukoaraiosis - no benefit
 –Cochrane review (2000) suggested no benefit –ESPRIT trial warfarin vs aspirin in non- cardioembolic stroke w/o leukoaraiosis - no benefit")
10
So what do I do? Heparin in acute stroke In acute stroke secondary to AF, in tight carotid stenosis, multiple TIA within 24 hrs, or ‘stroke in evolution’ consider getting help with decision from on-call neurologist or senior stroke physician If in doubt and no help is available, omission better than comission. You are supported by the guidelines

11
Then at day 1, 21.00hrs, further weakness and speech deterioration Eyes deviated to left Dense hemiparesis Now what do we do? Case 1

13
Intracerebral haemorrhage Recurrent infarction Seizure Hypotension Anaphylaxis Sepsis Hypoglycaemia Cerebral oedema Case 1 Post thrombolysis complications

14
Case 1 Day 2, GCS 10/15, increasingly drowsy Anything further we can do?

15
Case 1 Management of symptomatic cerebral haemorrhage post thrombolysis Consider 6-8 units of cryoprecipitate w. factor VIII and 6-8 units platelets Discuss w. neurosurgery (correct clotting first) Note duration of alteplase action –Rapidly cleared from plasma bt –Fribrinogen depletion 4 hr < 40% 24 hr >80% Bleeding after 36 hrs rarely secondary to thrombolytic treatment Any other ideas?
 Note duration of alteplase action –Rapidly cleared from plasma bt –Fribrinogen depletion 4 hr < 40% 24 hr >80% Bleeding after 36 hrs rarely secondary to thrombolytic treatment Any other ideas .")
16
Case 1 Decompressive craniectomy

17
Malignant infarction of MCA has 80% mortality rate Usually 2 nd to 5 th day Pooled data from DECIMAL, DESTINY, HAMLET Decompressive hemi-craniectomy within 48 hrs of stroke reduces mortality NNT to prevent death, severe disability, or moderate disability are 2,2, and 4 Now need to define optimal patient characteristics – probably younger Note neurosurgery in cerebellar CVA can be helpful When would a neurosurgeon help?

18
Outcome –Hemiparesis. Transfers with one –Speech improving Case 1

Similar presentations






 Thrombolytic canalization of occluded arteries may reduce the degree.>")












