Download presentation
Presentation is loading. Please wait.

1
A TOOL KIT FOR POST ACUTE CARE TRANSITIONS Robert Young MD, MS Feinberg School of Medicine Northwestern University Project BOOST Heather Zinzella-Cox MD, CMD Director of Long Term Care and Rehab Division Practice Group Leader, IPC-Delaware

2
Speaker Disclosures: Dr. Robert Young has nothing to disclose. Dr. Heather Zinzella-Cox has nothing to disclose.

3
A toolkit, necessary but not sufficient… Collaboration, relationships, and communication between stakeholders Focus on doing quality improvement together Addresses local context and customization Passion aimed at remediating a highly disruptive transition for our patients in the current context of our health care system

4
Learning Objectives: By the end of the session, participants will be able to: Understand policies driving hospital readmission reduction efforts Gain familiarity with national hospital readmission reductions programs Review examples of hospital and SNF transitions of care interventions Review elements and give feedback on proposed multi- stake holder transitions toolkit (including SHM/AMDA )
")
5
1 in 5 Medicare beneficiaries were rehospitalized in 30 days Estimated cost to Medicare: $17.4 Billion (2004) Jencks et. al. NEJM, 2009

6
1 in 4 Medicare SNF residents were rehospitalized in 30 days Estimated cost to Medicare: $ 4.34 Billion (2006) Mor et. al. Health Affairs, 2010

7
Reform-It’s here! And it’s NOT going away!!

8
Affordable Care Act :Reducing Readmissions Community Based Care Transitions Started in FY 2011 §3026 AHRQ Center for Quality Improvement and Safety AHRQ funding for projects related to QI research and technical assistance. Topics identified include reducing readmissions. For Period FY 2011-2014 §3501 Quality Improvement Program for Hospitals with a High Severity Adjusted Readmissions March 2012 Program for eligible to work with Patient Safety Organizations §399KK Hospital Readmissions Reduction Program Beginning in FY 2013 Hospitals with higher than expected readmissions rates will experience decreased payments for Medicare discharges §3025 Hospital Based Value Purchasing Beginning in FY 2013 Hospitals with poor performance indicators will experience decreased payments for Medicare discharges §1886 Carrot Stick

9
Hospital Readmissions Reduction Program Financial penalties on hospitals for “excess” readmissions vs. “expected” All DRG payment* amounts in hospitals with excess readmissions are reduced by a factor determined by the level of “excess, preventable readmissions” *Excludes: DSH, IME, and Outlier payments

10
Hospital Readmissions Reduction Program 30 day readmissions For 3 diagnosis (Effective FY2013): Heart Failure Acute MI Pneumonia Excess = ratio of actual to expected (risk-adj) Reduction of up to 1%, 2%, 3% first 3 years
: Heart Failure Acute MI Pneumonia Excess = ratio of actual to expected (risk-adj) Reduction of up to 1%, 2%, 3% first 3 years")
11
Hospital Readmissions Reduction Program Estimated to save $280 million this year Aiming for $7.1 billion in savings over 10 years Look up your acute care hospital’s penalty for this year at: http://www.kaiserhealthnews.org/

12
Hospital Readmissions Reduction Program Based on a three year window Adapted from Amy Boutwell

13
Does this policy harm hospitals that care for the poor? other unintended consequences? Hospital Readmissions Reduction Program FY2015: to include COPD, CABG, PTCA and Other Vascular (per MedPac report) Likely progressing to all cause readmissions No Child Left Behind for Hospitals? http://www.qualitymeasures.ahrq.gov/expert/expert-commentary.aspx?id=37562
 Likely progressing to all cause readmissions No Child Left Behind for Hospitals. id=")
14
Hospital Value Based Purchasing FYI 13 FYI 14 $ 964 Million projected reduction in payments this year: See your hospital’s estimated bonus/penalties http://www.kaiserhealthnews.org/Stories/2012/December/21/value-based-purchasing- chart.aspxttp://www.kaiserhealthnews.org/Stories/2012/December/21/value-based-purchasing- chart.aspx Source: Centers for Medicare and Medicaid Services

15
Community Based Care Transitions 5 year project, 81 project currently Community based organization partnered with hospitals Improve transitions of beneficiaries from the inpatient setting or other care settings Fee for service Partnering with Northwestern to reduce readmissions using Eric Coleman’s Prg For example:

16
Traditional Care Transitions Modified from Reason, J. BMJ 2000;320 Hard work Good intentions Smart caregivers Invested patients Nonstandardized care System failures Poor communication Patient issues Adverse events Patients Courtesy of Jeff Greenwald, MD, SFHM

17
Improved Care Transitions Modified from Reason, J. BMJ 2000;320 Patients Adverse events Hard work Good intentions Smart caregivers Invested patients Standardized care System support Effective communication Patient-centered care Courtesy of Jeff Greenwald, MD, SFHM

18
National Acute Care Transitions Programs The Care Transitions Program (Coleman) Project Re-Engineered Discharge STate Action on Avoidable Rehospitalizations Transitional Care Model (Naylor) Better Outcomes by Optimizing Safe Transitions Much hybridization between these initiatives. And many others… Some examples of programs your hospital partners might be working on :

19
Uses a transition coach who spans care settings to improve patient and family self-management Focuses on Four Intervention “Pillars”: Medication Self-Management Use of a patient Personal Health Record Timely PCP and specialty follow up Knowledge of red flags and how to respond 4 Week Program

20
Nurse discharge advocate who work with patients during their hospital stay Help to arrange follow up appointments Confirm medication reconciliation Conduct patient education with individualized instruction booklet sent to PCP Electronic avatar example….

21
Multi-stake holder approach, across organizational boundaries, engages national and state level: Payers Providers Patients Families Currently in Massachusetts, Michigan, and Washington Source: Amy Boutwell: Interacting with your hospitals: forming a cross- continuum team

22
Transitional Care Nurse (APNs) who also spans care settings Regular home visits and telephone support Ensures provider collaboration Early screening for change in status Promotes self management Provide holistic patient and family support
 who also spans care settings Regular home visits and telephone support Ensures provider collaboration Early screening for change in status Promotes self management Provide holistic patient and family support")
23
Three key components of BOOST: Health Literacy- “Teach back” education, esp. self care information Identification of high risk patients on admission and targeting risk specific interventions Quality improvement through mentored implementation (physician QI experts) with hospital’s process improvement team For more info on interventions: (Hansen LO, Annals of Internal Med 2011)
 with hospital’s process improvement team For more info on interventions: (Hansen LO, Annals of Internal Med 2011).")
24
Observational study of 6,955,461 Medicare FFS hospitalizations for HF; 1993 and 2006, with 30-day f/u. Mean age = 80 52% Htn, 38% DM, 37% COPD LOS 8.8 days down to 6.3 Discharges to SNF increased from 13% to 20% Discharge to home decreased from 74% to 67% 30 day readmission increased from 17.2% to 20.1% Post-discharge mortality increased from 4.3% to 6.4% In-hospital mortality declined from 8.5% to 4.3% 30-day mortality declined from 12.8% to 10.7% Bueno et al. June, 2010

25
34 Studies; all but 3 subjective median proportion of readmissions deemed avoidable was 27.1% (range 5 - 79%) “The true proportion of hospital readmissions that are potentially avoidable remains unclear.”
 The true proportion of hospital readmissions that are potentially avoidable remains unclear.")
26
JAMA Systematic Review in 2011 of validated readmission risk prediction models Kansagara et al. JAMA 2011; 306:1688-98 “Most current readmission risk prediction models that were designed for either comparative or clinical purposes perform poorly.”– nearly all AUC’s ~60%

27
An Issue of Incentives

28
A Few Comments on Transition Interventions Very little, if any, rigorous process/outcomes data Types of interventions are reaching saturation Most are multi-component interventions (similar to inpatient strategies) The keystone to these efforts are collaborative teams (including ED representatives) from both settings
 The keystone to these efforts are collaborative teams (including ED representatives) from both settings")
29
Taxonomy of Hospital and SNF Transitions of Care Interventions Acute CareSkilled Nursing Facility Bridging Interventions Discharge paperwork Disease specific order sets Post discharge follow up Nursing warm handoffs NP and PAs to follow patients @ SNF Acute care transfer paperwork Contact information from sending SNF provider Inventory of SNF services INTERACT, eSNF Collaborative Teams: Root Cause Analysis Aggregate data analysis (Community Level) Coordinate joint quality improvement efforts ED engagement- protocols regarding the return of patient to SNF Medication reconciliation Goals of care Physician warm handoffs (Bi-directional) Health Information Exchanges/RHIOs
 Coordinate joint quality improvement efforts ED engagement- protocols regarding the return of patient to SNF Medication reconciliation Goals of care Physician warm handoffs (Bi-directional) Health Information Exchanges/RHIOs")
30
Developed a partnership with area SNF’s to work on heart failure and pneumonia care transitions Joint monthly meetings (sometimes further apart depending on volume and results) to analyze readmissions Worked with SNF medical directors to develop and implement HF and PNA protocols Developed disease specific discharge orders and protocols Follow up phone calls post discharge to SNF to ensure transfer information and protocols were received and implemented An Example from BOOST: Nursing Home Collaboration
 to analyze readmissions Worked with SNF medical directors to develop and implement HF and PNA protocols Developed disease specific discharge orders and protocols Follow up phone calls post discharge to SNF to ensure transfer information and protocols were received and implemented An Example from BOOST: Nursing Home Collaboration")
31
Caution on disease specific interventions Ouslander et al JAMDA ‘11

32
Nursing Workflow: Key Points Sheet

33
Discharge to Nursing Home Standard Orders

34
In Response…the SNFs Worked to cohort short term patients on to specialized units Implement heart failure clinics within the SNF Some SNFs are now sending case manager to follow the patient in the hospital Started to implement INTERACT (watching adherence closely) Educating SNF staff on HF and PNA with hospital providing CEUs ------------------------------------------------------------------------------- Silver Cross now starting to have Transitions Case Manager follow HF and PNA patients in house and 30 days after discharge into the SNF
 Educating SNF staff on HF and PNA with hospital providing CEUs Silver Cross now starting to have Transitions Case Manager follow HF and PNA patients in house and 30 days after discharge into the SNF")
36
An Example From IPC Great example hospitalist and SNF/LTC provider collaboration Motivated by benefits for both providers: Improve patient safety/decrease readmissions Increased market share, referrals to SNF, leverage with hospitals (for hospitalists) Prepare for future: ACO, bundled payments ECF Medical Director/Hospital Based Medical Director ensured close coordination of efforts on the SNF/LTC side and in the acute care setting-> Cross setting interprofessional team
 Prepare for future: ACO, bundled payments ECF Medical Director/Hospital Based Medical Director ensured close coordination of efforts on the SNF/LTC side and in the acute care setting-> Cross setting interprofessional team")
37
SNF/LTC side Went through a rigorous process looking at causes of readmissions: RCA, analyzing facility readmission rates, LOS of index hospitalization, admitting and d/c dx, timing of readmission (day of the week), nurse to pt ratio/staff on duty, doctor on call. Found: Vast majority occurred within 7 days of NF admission Readmitted over the weekend and Monday morning Occurred on evening shift RCA revealed- 1 st week: due to poor handoff from hospital 2 nd week: poor facility communication 2 nd -4 th week: facility communcition/unavoidable

38
Hospital Side Went through flow mapping of discharge process to SNF (failure modes effects analysis), RCA with fishbone diagram of hospital specific causes, surveyed NH regarding completeness and timeliness of communication
, RCA with fishbone diagram of hospital specific causes, surveyed NH regarding completeness and timeliness of communication")
39
Hospital Side cont. Collaborated with ECF Team, Physician, Nurse, Social Work and Care Management identifying gaps in transition: Timeliness of Discharge Poor hand-off communication Lack of pertinent documentation Collaborative follow-up

40
Interventions SNF/LTC Physician 5 days a week 8 hrs a day. New admits on weekends if possible SBAR/Interact II inservices to nurses and ECF physician CHF/COPD/PNA/UTI and high risk patients talked about daily in AM report High Risk patients with frequent follow up by MD/NP Acute Care Side Social Services ids receiving doc. Interagencies and Med. Rec completed/ RX on chart and faxed Chart copied timely fashion Warm physician & RN handoff D/C Summary faxed to ECF PCF/Staff RN prepare a “Discharge Communication Packet” Communication Tool, Interagencies, Med. Rec., D/C Summary, RX Post D/C Call to review patient status

41
Results: Process Metrics Post DC Call to ECF providers provided valuable feedback regarding the process changes implemented and what was of best value regarding transition process

42
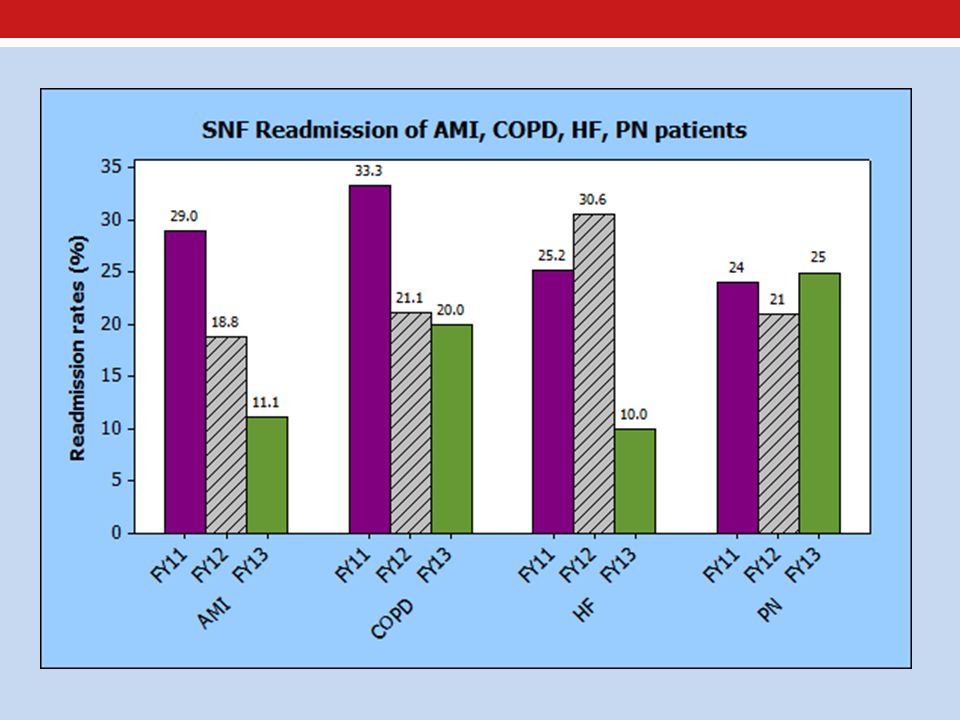
Results: Readmission Outcomes Decreasing readmission rate in both target population for project and all 5C patients

43
Results: Hospital Staff Perceptions of Care ECF feedback regarding process improvement changes implemented consistently favorable and supportive

44
INTERACT Transition Tools Multiple Transitions Tools for Acute Care and SNF Engaging Hospitals in Your Program Hospital to Post-Acute Care Transfer Form Acute Care Transfer Document Checklist Nursing Home Capabilities List Nursing Home to Hospital Transfer Form

45
Engaging Hospitals in Your Program Great tips: Making sure hospital receives and uses transfer information-> Need to review transfer package with ED, Acute care. Be ready to accept the patient back to the facility if appropriate Identify the readmissions champion at the hospital (talk to CMO, CNO…)
.")
46
Hospital to Post Acute Care Transfer Form Demographics Goals of care, advanced directives Acute care physician’s contact information Clinical info, procedures High risk conditions/treatments Nursing care, nutrition, therapies, skin care, infection control Precautions Pending tests and f/u

47
Acute Care Transfer Document Checklist Check list to make sure that transfer document package is complete. Even has a message to make sure that the inpatient unit gets the documentation

48
Nursing Home Capabilities List A list of available services: Clinician and consult services Diagnostic tests Therapies Social and Psych svcs Nursing svcs Interventions Pharmacy svs

49
Nursing Home to Hospital Transfer Form Demographics Contact information Code status Clinical Info Mental status Functional status Devices and rx Isolation precautions Risk alerts Conditions for accepting resident back

50
Nursing Home to Hospital Transfer Form 2 nd page that could be forwarded later Family and other social issues Behavioral Issues Primary Goals of Care at transfer Diet, Skin, Immunizations, Physical Therapy, ADLS, Impairments, Continence

51
The SHM Post Acute Care Task Force Transition Toolkit

52
PAC project advisory board Karl Steinberg, MD, CMD Keith Krein, MD, CMD Heather Zinzella-Cox, MD, CMD Amy Boutwell, MD, MPP Donald Quinn, MD, MBA Kerry Weiner, MD Sean Muldoon, MD, MPH Sabitha Rajan MD, MSc Rob Young, MD, MS Tina Budnitz, MPH Mark Williams, MD

53
SHM Post Acute Care Task Force Toolkit Project Goal is to create an acute care to SNF transitions toolkit Have gone through expert panel process to identify issues complicating acute care hospital transfers to SNF and back Once finalized- aim to pilot with BOOST and other hospital-snf groups

54
Post Acute Care Project cont. Implementation Guide For Acute Care Providers partnered with SNF Providers Discuss issues that we may not be able to change (policies, structural issues) but should be aware of Integrate toolkit into a QI process Educational recommendations for housestaff, hospitalists, and other acute care providers Online Toolkit Repository of recommended instruments for participants to use Allow various organizations to submit their instrument for review and dissemination through the toolkit Develop needed instruments to fill in gaps Additional Work on Engaging Emergency Medicine Even with communication tools, what process needs to be in place to give EM providers the confidence to return the patient to SNF, if appropriate Can hospitalist help? Perhaps consult on EM patients and reach out to SNF providers to facilitate return process
 but should be aware of Integrate toolkit into a QI process Educational recommendations for housestaff, hospitalists, and other acute care providers Online Toolkit Repository of recommended instruments for participants to use Allow various organizations to submit their instrument for review and dissemination through the toolkit Develop needed instruments to fill in gaps Additional Work on Engaging Emergency Medicine Even with communication tools, what process needs to be in place to give EM providers the confidence to return the patient to SNF, if appropriate Can hospitalist help. Perhaps consult on EM patients and reach out to SNF providers to facilitate return process.")
55
Implementation Guide: Examples of Issues to Address Environment, Governmental Regulation Federal and state level regulations Variations in SNF at local level State Health Information Exchanges Facility Level Issues Medication issues (antibiotic selection, narcotics) Timing of discharges (e.g. Friday afternoons) Staffing issues / availability of services Nursing to nursing warm handoffs EMR access (read only)
 Staffing issues / availability of services Nursing to nursing warm handoffs EMR access (read only).")
56
Implementation Guide: Examples of Issues Physician Level Factor Lack of person in charge of transfer (social work vs. physician vs. nurse?) Housestaff education in academic settings Acute care physician education regarding SNF and available services Clarification of specialty care plan and contact information Variations in discharge process depending on discharging service (ortho vs gen surgery vs medicine discharges) Availability of discharge summaries/discharge summary content Patient and Family Concerns Addressing patient and family expectations (fact sheet?) Goals of care discussions Issues with dementia and other behavioral problems
 Housestaff education in academic settings Acute care physician education regarding SNF and available services Clarification of specialty care plan and contact information Variations in discharge process depending on discharging service (ortho vs gen surgery vs medicine discharges) Availability of discharge summaries/discharge summary content Patient and Family Concerns Addressing patient and family expectations (fact sheet ) Goals of care discussions Issues with dementia and other behavioral problems.")
57
Online Toolkit (Prior example)
")
58
Engaging Emergency Medicine Need to determine what elements are necessary for EM to feel confident about discharging patients back to SNF when appropriate Determine if other information is needed upon transfer to the ED May need to do some qualitative work to determine EM concerns What can hospitalist do to help?

59
Thanks for your attention! Contact Information Further questions or comments? Feel free to contact us at: Heather: hzinzella@ipc-hub.comhzinzella@ipc-hub.com Rob: r-young@northwestern.orgr-young@northwestern.org

Similar presentations





 A Community Collaboration.>")

 MassPro February, 2013 2:30p-3:30p.>")










 Supporting Patients and Practitioners in Optimizing Health.>")
