Download presentation
Presentation is loading. Please wait.

1
Assessing & Managing Pain in Older Adults Arden L Aylor, MD Geriatrics

2
Objectives Prevalence and characteristics of pain in the elderly Factors that influence pain perception in older adults Challenges in assessing pain EBM practice guidelines for managing pain in older adults

3
What is Old?

4
Prevalence of Pain in Older Adults Effecting ADLs 25-50% of community-dwelling older adults 45-80% of nursing home residents >50% of elderly patients with multiple co-morbidity >60% of hospitalized patients in last 3 days of life 31% of women and 19% of men >75 yrs report pain in 3 or more areas of the body Urwin et al, 2006

5
Prevalence of Acute Pain 75% of hospitalized adults reported experiencing moderate - severe pain at some point during their hospitalization 21% of older persons admitted to the hospital reported under-treated moderate - severe pain during their hospitalization IASP, 2006

6
The Picture of Pain in Older Adults Chronic pain is often multi-focal and multi- factorial Common types: ◦ Musculoskeletal ◦ Internal organ ◦ Neuropathic ◦ Cancer-related

7
The Picture of Pain in Older Adults Many hospitalized older adults will have both chronic and acute pain In hospitalized Pts, pain is often under assessed and/or under-treated

8
Pain Treatment in Hospitalized Older Adults Cognitively intact older Pts with hip fracture: ◦ 44% rated pre-op pain as very severe (>8/10) ◦ 42% rated post-op pain as very severe (>8/10) ◦ 83% of Pts had no standing order for analgesic during entire hospital stay What about our cognitively impaired patients? Pain Sympt Manage, 2005

9
Unrelieved Pain in NH Residents 45-80% have substantially under-treated pain 29% with cancer have unrelieved daily pain ◦ 26% received no scheduled analgesics 25% have unrelieved daily non-cancer pain ◦ 31% received no analgesics 32% of bereaved family members reported NH patients did not receive adequate help with pain during the last days Pain Sympt Manage, 2005

10
Consequences of Persistent Pain Unnecessary suffering Depression and anxiety Impaired ambulation & gait disturbance Sleep disturbances Impaired cognition Impaired appetite & weight loss Decreased socialization Increased healthcare utilization ( cost) Increased agitation and resistance to further care AGS Guideline for Persistent Pain, 2007
 Increased agitation and resistance to further care AGS Guideline for Persistent Pain, 2007")
11
Consequences of Untreated Acute Pain Impaired ambulation Slower functional recovery Functional disability Higher rate of post-op complications Conversation to chronic pain Increased risk for delirium Increased mortality AGS Guideline for Persistent Pain, 2007

12
Acute Pain and Delirium Risk factors for delirium among older adults hospitalized with hip fracture: ◦ Cognitive Impairment - RR: 65% ◦ Receiving opiods - RR: 95% In cognitively intact patients: o Severe pain was associated with 9x the risk of delirium AGS Guideline for Persistent Pain, 2007

13
The Experience of Pain in Older Adults – is it Different?

14
Effects of Aging on Pain Processing Pain threshold decreases with age ◦ EEG responses to acute noxious stimuli decreased in speed & amplitude Tolerance to pain increases with age ◦ Degenerative changes in 5HT and NE levels contribute to impaired neurotransmission and inappropriate pain perception ◦ Decreased efficacy of endogenous opioid analgesic systems Gagliese & Farrell, 2005

15
Pain Coping Strategies in Older Adults Older adults with chronic pain have a greater risk of catastrophic outcomes compared to those with similar diagnoses Older adults often have poor problem solving & coping strategies Older adults tend to focus more on prayer and hope rather than medical intervention Gibson, 2006

16
Challenges in Assessing and Treating Pain in Older Adults Illness-related & physiological barriers Patient and caregiver attitudes A-typical presentation Lack of appropriate assessment tools specific to older adults

17
Illness-Related and Physiological Barriers Sensory deficits Cognitive impairment Increased sensitivity to: ◦ Medication side effects ◦ Polypharmacy Co-morbidity Depression

18
Attitudes that Hinder Pain Reporting Stoic: They do not wanting to be perceived as a “complainer” Concerns about addiction, side effects and tolerance Pain in old age is inevitable Nothing can be done to relieve pain Older adults cannot tolerate strong analgesics Older adults are less sensitive to pain

19
A-typical Presentations “I don’t have any pain, but I sure am sore!” “I feel fine - as long as I’m not moving!” Pain is what the patient says it is - but what if they can’t tell us?

20
Nonverbal Patients Coma Advanced dementia Status post stroke End-of-Life Developmentally disabled Delirium

21
Cognitive Impairment & Pain Management Study: Advanced dementia patients hospitalized with hip fracture received 1/3 the amount of opioid analgesics that cognitively intact older patients received Cognitively impaired (MMSE < 23) hip surgery Pts received significantly less opioids than intact older patients despite reporting similar pain intensity J Ortho, 2004
 hip surgery Pts received significantly less opioids than intact older patients despite reporting similar pain intensity J Ortho, 2004")
22
What is Different about the Pain Experience of People with Advanced Dementia? Tolerance to acute pain possibly increases, but pain threshold appear to decrease Dementia may blunt response to acute pain Cognitive impairment may decrease the perceived analgesic effectiveness Pain can negatively affect cognitive function

23
ASPMN: Position Statement Ethical principles Establish a pain assessment procedure protocol “Assume Pain is Present” Use empirical trials Re-assess and document Pain Management Nursing, 2006

24
ASPMN: Pain Assessment Patient’s may self-report pain Behaviors (facial expressions, crying) Follow-up reported pain from a family members or caregivers Follow-up on Pts response to empirical therapy
 Follow-up reported pain from a family members or caregivers Follow-up on Pts response to empirical therapy")
25
Can Patients with Cognitive Impairment Reliably Report Pain? Cognitive Impaired NH Pts under report pain, yet their reports are still valid 83% - cognitive impaired NH residents could reliably complete at least one pain scale 73% - post-op patients with moderate cognitive impaired were able to complete a 4-point verbal descriptor scale Pain Management, 2006

26
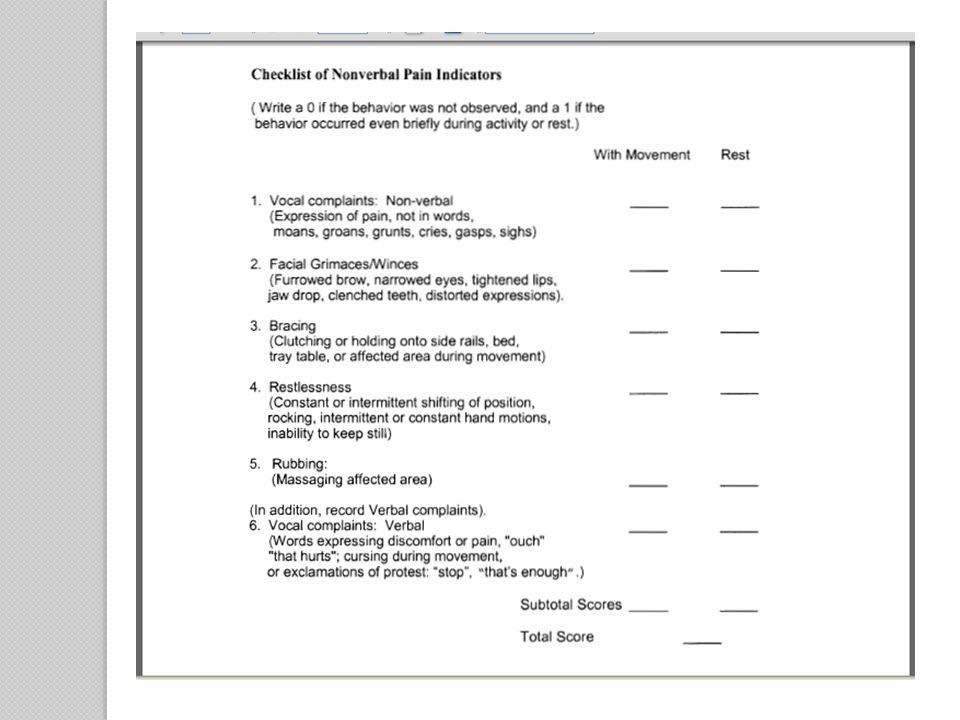
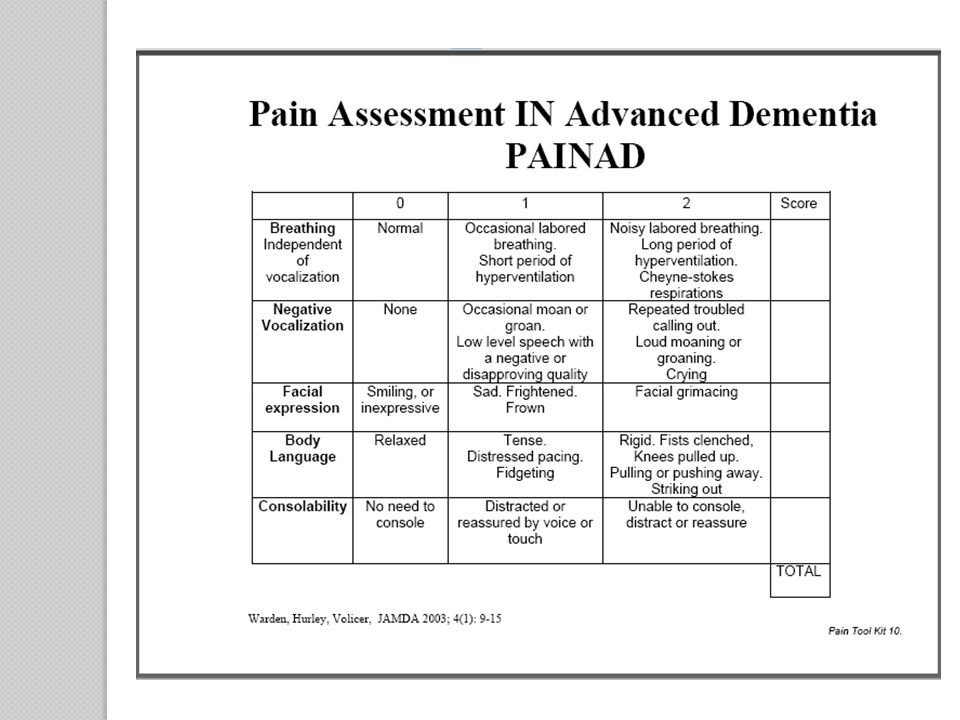
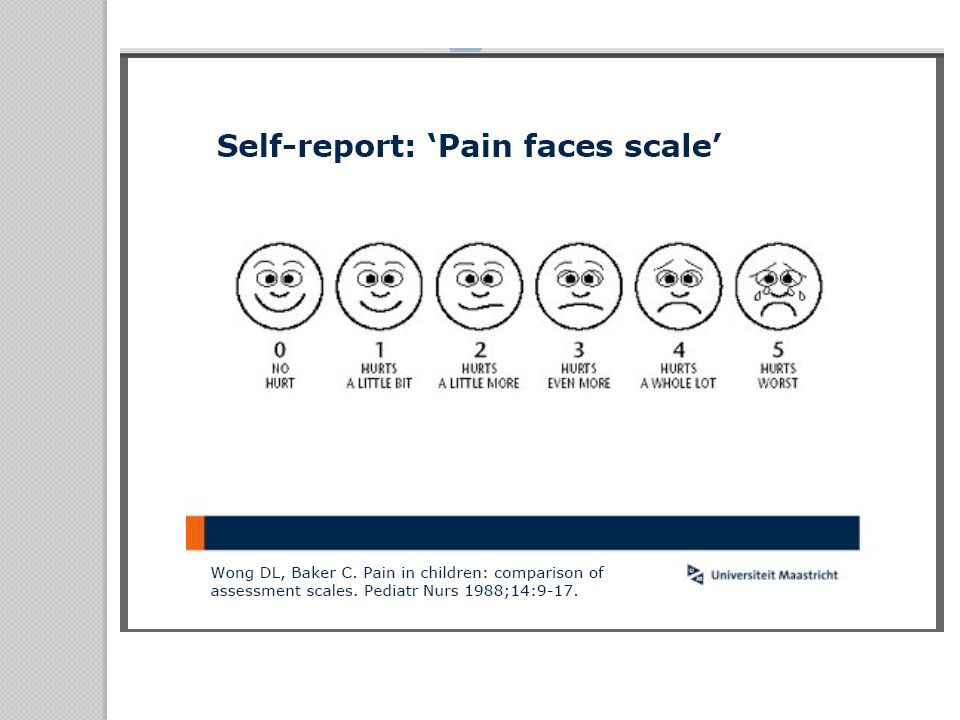
Pain Behavior Assessment Tools Checklist for Nonverbal Pain Indicators PAIN-AD Pain Faces Scale Pain Assessment Scale for Seniors with Severe Dementia (PACSLAC)
")
30
PACSLAC Four subscales with a total of 60 items: Facial expressions (13 items) Activity/body movements (20 items) Social/personality/mood (12 items) Physiological indicators/Eating and sleeping changes/Vocal behaviors (15 items) The number of checks on each are added together and recorded and then these sums are added together for a total score.
 Activity/body movements (20 items) Social/personality/mood (12 items) Physiological indicators/Eating and sleeping changes/Vocal behaviors (15 items) The number of checks on each are added together and recorded and then these sums are added together for a total score.")
31
Evidence for Attempting Empirical Analgesic Trial 650 mg TID APAP: 63% decrease in negative behaviors ◦ Allowed 75% of psychotropic medications to be discontinued Standardized assessment and treatment protocol significantly decreased discomfort among demented NH residents Regular analgesic therapy increased social engagement in NH residents Gibson, 2006

32
EBM: Guidelines for Persistent Pain American Geriatrics Society: Management of persistent pain in older persons www.americangeriatrics.org American Medical Directors Association: Pain management in the long term care setting www.amda.com ASPM: Persistent pain management Iowa City (IA): University of Iowa Gerontological Nursing Interventions Research Cen ter
: University of Iowa Gerontological Nursing Interventions Research Cen ter")
33
Pearls from the Guidelines Minimize reliance on physical signs of pain Include cognitive status in your initial pain assessment Establish the terms the patient uses to describe their pain and document Establish the pain intensity tool that works for the individual and use it consistently Teach caregivers how to assess for barriers

34
Pearls from the Guidelines Avoid use of antipsychotic therapy for behavior issues Always combine analgesic therapy with non-drug therapy Maximize APAP dose (4 gm/day) Use empirical analgesic trials for nonverbal patients Avoid use of codeine and propoxyphene (Darvocet) Patient goals for therapy - include functional goals
 Use empirical analgesic trials for nonverbal patients Avoid use of codeine and propoxyphene (Darvocet) Patient goals for therapy - include functional goals")
35
Thank You

Similar presentations




 Vancouver Coastal Health.>")














, ARNP Ann L. Horgas, RN, PhD, FAAN University of Florida College of Nursing.>")