Download presentation
Presentation is loading. Please wait.

1
Total Colonic Hirschsprung Disease
Tyler Bergstrom

2
Hirschsprung Disease Functional obstruction related to failure of a segment of bowel to relax secondary to abscense of parasympathetic myenteric and submucosal nerve cells in a segment of bowel 1:5,000 live births Total colonic aganglionosis (TCA) – extends from anus to >ileocecal valve up to 50 cm proximal TCA - ~1:50k; 5-7% HD cases M:F ratio = 4:1, 2:1 in long seg, and 1.1:1 in TCA TCA – overall mortality ~ 50% Danish pediatrician – first described in detail in 1888, aganglionic findings not evident until 1900s (dis 1st described in1800) Asians, males (4:1, 2:1 in long seg, and 1.1:1 in TCA), usually have failure of passage of meconium within 48 hrs -- classic explosive, foul-smelling stools assoc with fever and abd distension = HD entercolitis -pts need irrigation, Abx, and fluids -longer segments – need emergent ex lap with colostomy prox to aganglionic bowel
 – extends from anus to >ileocecal valve up to 50 cm proximal. TCA - ~1:50k; 5-7% HD cases. M:F ratio = 4:1, 2:1 in long seg, and 1.1:1 in TCA. TCA – overall mortality ~ 50% Danish pediatrician – first described in detail in 1888, aganglionic findings not evident until 1900s (dis 1st described in1800) Asians, males (4:1, 2:1 in long seg, and 1.1:1 in TCA), usually have failure of passage of meconium within 48 hrs. -- classic explosive, foul-smelling stools assoc with fever and abd distension = HD entercolitis. -pts need irrigation, Abx, and fluids. -longer segments – need emergent ex lap with colostomy prox to aganglionic bowel.")
3
Pathogenesis Aberrant colonization of ganglion cells in the myenteric and submucosal plexuses Decreased pool of neuroblasts, abnormal migration of neuroblasts, germline mutations, alteration in local tissue environment Results in lack of peristaltic wave propagation TCA separate disease from short segment HD or a longer form? -Neural crest cells migrate prox to distal -- possibly failure to migrate, failure to develop in successful migration -Other factors may contribute to TCA – malnorishment, errors in apoptosis, errors in cell differentiation – unclear if

4
Genetics >10 genes associated RET, EDNRG and END3 genes most common
RET variations in >70% TCA cases Endothelin system gene defects – EDNRB, decreased expression of EDN3 receptor Longer segments = higher familial association (15-20%) TCA – Trisomy 21 less common, few reliable associated abnormalities Associated genetic abnormalities (all variants): Trisomy 21 Cardiac septal defects Congenital central hypoventilation syndrome MEN type 2 Neurofibromatosis Waardenburg’s syndrome Anorectal malformations GU abnormalities RET thought to be most important in TCA Endothelin assoc in TCA – 37% vs 5% in HD MEN syn – higher assoc with longer segment HD
 TCA – Trisomy 21 less common, few reliable associated abnormalities. Associated genetic abnormalities (all variants): Trisomy 21. Cardiac septal defects. Congenital central hypoventilation syndrome. MEN type 2. Neurofibromatosis. Waardenburg’s syndrome. Anorectal malformations. GU abnormalities. RET thought to be most important in TCA. Endothelin assoc in TCA – 37% vs 5% in HD. MEN syn – higher assoc with longer segment HD.")
5
Histology Nerve immunostains significantly decreased in TCA compared to less severe forms TCA – lack of thick nerve trunks and near total loss of interstitial cells of Cajal Hypoganglionosis or extended transition zones in TCA animal models -Usually still see ICC in less severe forms -Extended transition zone not confirmed in humans

6
Diagnosis Failure to pass meconium in 1st 48 hrs, abd distension, bilious emesis TCA may present later and with milder symptoms Contrast enema Difficulty finding transition zone in 25% of TCA and false transition zones (more proximal in 10%) TCA – strongly associated with retention of barium > 24hrs Rectal and seromuscular biopsies total colonic HD can have elevated AchE activity in rectum and L colon but show near normal levels in proximal colon Anorectal manometry TCA – as much as 27% present after neonatal period; difficulties in Dx in ½ cases Contrast enema – would indicate transition zone and irregular colonic contractions in the distal segment, if entercolitis – mucosal ulcerations may be present; classic ? – only in 18% Bx – abscess of both myenteric and submucosal plexus with hypertrophic nerve fibers is dx; also increased AchE staining; enzymatic activity levels in rapid frozen section can help det proximal pt -- note – tot colonic HD can have elevated AchE act in rectum and L colon but show near normal levels in proximal colon Manometry – used in older children (distend rectum – should see reflexive relaxation of internal sphincter), can r/o HD
 TCA – strongly associated with retention of barium > 24hrs. Rectal and seromuscular biopsies. total colonic HD can have elevated AchE activity in rectum and L colon but show near normal levels in proximal colon. Anorectal manometry. TCA – as much as 27% present after neonatal period; difficulties in Dx in ½ cases. Contrast enema – would indicate transition zone and irregular colonic contractions in the distal segment, if entercolitis – mucosal ulcerations may be present; classic – only in 18% Bx – abscess of both myenteric and submucosal plexus with hypertrophic nerve fibers is dx; also increased AchE staining; enzymatic activity levels in rapid frozen section can help det proximal pt -- note – tot colonic HD can have elevated AchE act in rectum and L colon but show near normal levels in proximal colon. Manometry – used in older children (distend rectum – should see reflexive relaxation of internal sphincter), can r/o HD.")
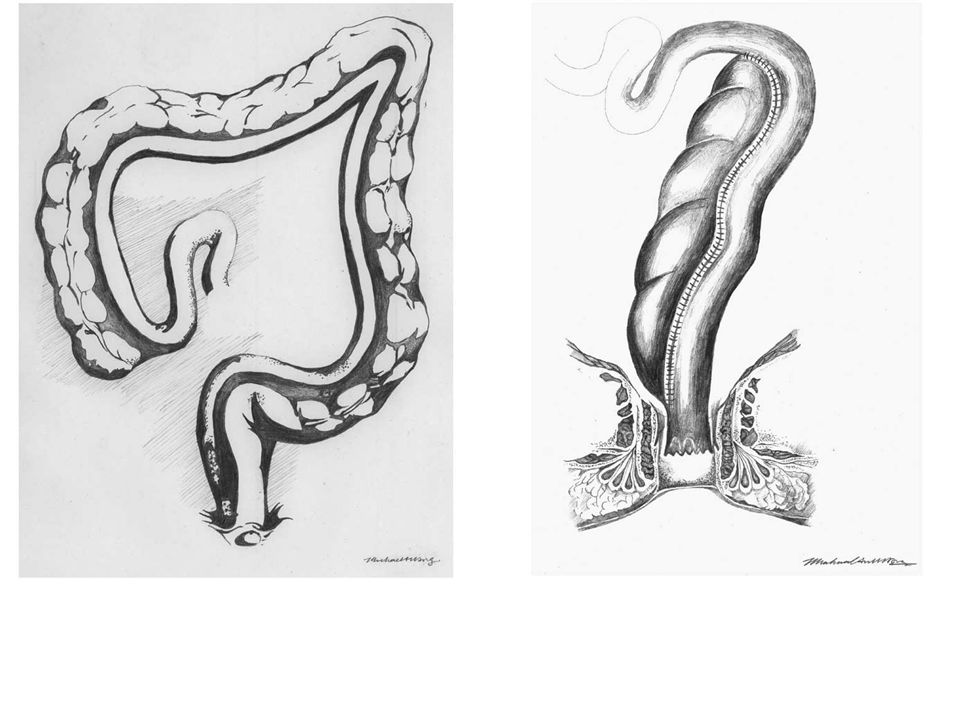
7
-classic “?” look of TCA

8
AXR – initial (1d old)
")
9
AXR 11/7 (HD 4)
")
10
Treatment Options Initial resuscitation, Abx, NGT
Initial leveling small bowel enterostomy with definitive surgical treatment 6-12 mo later No consensus on operation with best outcomes In staged – colostomy with Hartman pouch (unless transition zone is at or above splenic flexure) LATEP (lap assisst transanal endorectal pull-through) Pre-pull through mortality rate is 15%
 LATEP (lap assisst transanal endorectal pull-through) Pre-pull through mortality rate is 15%")
11
Surgical Management Swenson Soave Duhamel – Martin or mod std
Kimura colonic patch Swenson - removal of the entire aganglionic colon, with an end-to-end anastomosis above the anal sphincter Soave – attempt to avoid pelvic disection risks of Swenson; submucosal endorectal dissection and placing the pull-through bowel within a "cuff" consisting of aganglionic muscle Duhamel - the normal colon down through the bloodless plane between the rectum and the sacrum and joining the two walls to create a new lumen, which was aganglionic anteriorly and normally innervated posteriorly Martin modification – long side-to side anst of ganglionic ileum to aganglionic colon; not often performed due to increased morbidity rate (64%) Kimura patch - placing a right colon patch segment placed proximal to enterostomy (stoma site) with vascular pedicle intact then on 2nd procedure take the ostomy down and anast to anus as pull through (patch will act to absorb water and slow transit) *right colon has better H2O abs capacity Duhamel operation favored in a 2011 study from England among surgeons
 Kimura patch - placing a right colon patch segment placed proximal to enterostomy (stoma site) with vascular pedicle intact then on 2nd procedure take the ostomy down and anast to anus as pull through (patch will act to absorb water and slow transit) *right colon has better H2O abs capacity. Duhamel operation favored in a 2011 study from England among surgeons.")
13
Surgical Management Restorative proctocolectomy with J-pouch ileoanal anastomosis 5 - 7 cm-long stapled J-pouch and its apex sewn to the anal canal 1–2 cm above the dentate line BM frequency is 3 /day at 24 mo (5-6 in PO for typical TCA) -Used for UC and FAP patients -Protective ileostomy then f/u with ileostomy closure 3 mo after initial operation
 -Used for UC and FAP patients. -Protective ileostomy then f/u with ileostomy closure 3 mo after initial operation.")
14
Functional Outcomes Good bowel control in 60% (lack of incontinence, soiling, etc) 1/3 incontinent, 10% in diapers at night Daily BM rate of 5-6 in childhood and 3-4 in adolescence Minor developmental delay associated with longer aganglionic segment TCA pts – >50% below 2nd percentile for weight, 25% underweight at age 5 Other factors such as major devel delay, differences in wt were not statistically significant difference

15
36 papers analyzed from 1980 to 2011
Of 396 pts in long term f/u - 60% had satisfactory or normal bowel control 25% of the patients were soiling at long-term follow-up. 17.5% need for major operation Overall long-term poor outcome in this study was 33% Permanent stomas and the need for rectal dilatations and washouts were considered, with 6.5% of the patients requiring a permanent stoma Major operation including redo PT, stoma formation, or other laparotomy

16
Post-operative complications
Entercolitis – more common in TCA postoperatively (42% in pull through operations vs 10.6% in rectosigmoid HD) Related to amount retained aganglionic segment Obstructive symptoms ~ 10% Mortality after operation was 1.9% in retro study Entercolitis – often assoc with outflow obstruction; fever, abdominal distention, diarrhea, elevated white blood cell count, and evidence of intestinal edema on abdominal radiograph -Tx: nasogastric drainage, intravenous fluids, broad-spectrum antibiotics, and decompression of the rectum and colon using rectal stimulation or irrigations
 Related to amount retained aganglionic segment. Obstructive symptoms ~ 10% Mortality after operation was 1.9% in retro study. Entercolitis – often assoc with outflow obstruction; fever, abdominal distention, diarrhea, elevated white blood cell count, and evidence of intestinal edema on abdominal radiograph. -Tx: nasogastric drainage, intravenous fluids, broad-spectrum antibiotics, and decompression of the rectum and colon using rectal stimulation or irrigations.")
17
References Moore S. Total colonic aganglionosis in Hirschsprung disease. Seminars in Pediatric Surgery (2012) 21, McLaughlin D, Friedmacher F, Puri P. Total colonic aganglionosis: a systematic review and meta-analysis of long-term clinical outcome. Pediatr Surg Int (2012) 28:773–779 Hukkinen, M , Koivusalo A, Rintala RJ, Pakarinen MP. Restorative proctocolectomy with J-pouch ileoanal anastomosis for total colonic aganglionosis among neonates and infants. Journal of Pediatric Surgery 49 (2014) 570–574. Marquez T, Acton R, Hess Donavon, Duval S, Saltzman D. Comprehensive review of the procedures of total colonic aganglionosis. Journal of Pediatric Surgery (2009) 44, 257–265. Escobar m, GrosfeldJ, West K, et al. Long-term outcomes in total colonic aganglionosis: a 32-year experience. Journal of Pediatric Surgery (2005) 40, 955–961. More K, Rao S, McMichael J, et al.Growth and Developmental Outcomes of Infants with Hirschsprung Disease Presenting in the Neonatal Period: A Retrospective Study. Journal of Pediatric Surgery. Blackburn et al.. Total Colonic Aganglionosis. European Journal of Pediatric Surgery. July 2013.
 28:773–779. Hukkinen, M , Koivusalo A, Rintala RJ, Pakarinen MP. Restorative proctocolectomy with J-pouch ileoanal anastomosis for total colonic aganglionosis among neonates and infants. Journal of Pediatric Surgery 49 (2014) 570–574. Marquez T, Acton R, Hess Donavon, Duval S, Saltzman D. Comprehensive review of the procedures of total colonic aganglionosis. Journal of Pediatric Surgery (2009) 44, 257–265. Escobar m, GrosfeldJ, West K, et al. Long-term outcomes in total colonic aganglionosis: a 32-year experience. Journal of Pediatric Surgery (2005) 40, 955–961. More K, Rao S, McMichael J, et al.Growth and Developmental Outcomes of Infants with Hirschsprung Disease Presenting in the Neonatal Period: A Retrospective Study. Journal of Pediatric Surgery. Blackburn et al.. Total Colonic Aganglionosis. European Journal of Pediatric Surgery. July")
Similar presentations






 Clase 10: Fisiología del colon Dr. Michel Baró A.>")

 Arch Debranching vs. Elephant Trunk for Hybrid Repair of the Proximal Thoracic Aorta Arch Debranching versus Elephant Trunk Procedures for Hybrid Repair.>")







 is characterised by massive colonic dilation with symptoms and signs of colonic obstruction.>")



