Download presentation
Presentation is loading. Please wait.

1
Hunger When are we hungry? When do we eat? When there is no food in our stomach. When we are hungry. How do we know when our stomach is empty? Our stomach growls. These are also called hunger pangs.

2
407-420 Create a visual display that shows the interaction of our experiences and how they interact with biology to motivate us to eat....too much (weight gain) or too little. Areas of focus: –Physiological Focus Body chemistry & brain –Psychology of Hunger Taste Preference Situational After looking at the research, what has a bigger role, Biological, Psychological, Social-Cultural as it relates to the larger problem of either obesity or anorexia / bulimia. Groups (3) – take time with text and then collaborate. 45 minutes – 15 minutes to share out.
 – take time with text and then collaborate. 45 minutes – 15 minutes to share out..")
4
Summary

5
The Physiology of Hunger Stomach contractions (pangs) send signals to the brain making us aware of our hunger.
 send signals to the brain making us aware of our hunger.")
6
Stomachs Removed Tsang (1938) removed rat stomachs, connected the esophagus to the small intestines, and the rats still felt hungry (and ate food).
 removed rat stomachs, connected the esophagus to the small intestines, and the rats still felt hungry (and ate food).")
7
Motivation-Hunger Variations in body chemistry are important We feel hungry when glucose levels are low –Goes to the hypothalamus (regulates body’s weight as it influences our feelings of hunger and safety) To maintain its set point weight, the body also adjusts its basal metabolic rate of energy expenditure. Basal Metabolic Rate –body’s base rate of energy expenditure

8
Glucose: C 6 H 12 O 6 The glucose level in blood is maintained. Provides the major source of energy for body tissues. When its level is low, we feel hunger. Insulin decreases glucose in the blood, making us feel hungry. Glucose Molecule

9
Glucose & the Brain Levels of glucose in the blood are monitored by receptors (neurons) in the stomach, liver, and intestines. They send signals to the hypothalamus in the brain. Rat Hypothalamus

10
Hypothalamic Centers The lateral hypothalamus (LH) brings on hunger (stimulation). Destroy the LH, and the animal has no interest in eating. The reduction of blood glucose stimulates orexin in the LH, which leads rats to eat ravenously.

11
Hypothalamic Centers The ventromedial hypothalamus (VMH) depresses hunger (stimulation). Destroy the VMH, and the animal eats excessively. Richard Howard

12
Hypothalamus & Hormones The hypothalamus monitors a number of hormones that are related to hunger. HormoneTissueResponse Orexin increaseHypothalamusIncreases hunger Ghrelin increaseStomachIncreases hunger Insulin increasePancreasIncreases hunger Leptin increaseFat cellsDecreases hunger PPY increaseDigestive tractDecreases hunger

13
Set-Point Theory Suggest humans are genetically programed to carry a certain amount of body weight. Set Point – the weight the body normally maintains when one is trying neither to gain or lose weight. Influenced by the number of fat cells in the body and the metabolic rate. –Manipulating the lateral and the ventromedial hypothalamus alters the body’s “weight thermostat.” –If weight is lost, food intake increases (increase in hunger) and energy expenditure decreases (metabolic rate decreases). If weight is gained, the opposite takes place.
 and energy expenditure decreases (metabolic rate decreases). If weight is gained, the opposite takes place..")
14
The Psychology of Hunger Memory plays an important role in hunger. Due to difficulties with retention, amnesia patients eat frequently if given food (Rozin et al., 1998).
..")
15
Taste Preference: Biology or Culture? Body chemistry and environmental factors influence not only when we feel hunger but what we feel hungry for! Richard Olsenius/ Black Star Victor Englebert

16
Hot Cultures like Hot Spices Countries with hot climates use more bacteria- inhibiting spices in meat dishes.

17
Eating Disorders Anorexia Nervosa: A condition in which a normal-weight person (usually an adolescent woman) continuously loses weight but still feels overweight. Reprinted by permission of The New England Journal of Medicine, 207, (Oct 5, 1932), 613-617. Lisa O’Connor/ Zuma/ Corbis
, Lisa O’Connor/ Zuma/ Corbis.")
18
Eating Disorders Bulimia Nervosa: A disorder characterized by episodes of overeating, usually high-calorie foods, followed by vomiting, using laxatives, fasting, or excessive exercise.

19
Statistics on Eating Disorders It is estimated that 8 million Americans have an eating disorder – seven million women and one million men One in 200 American women suffers from anorexia Two to three in 100 American women suffers from bulimia Nearly half of all Americans personally know someone with an eating disorder (Note: One in five Americans suffers from mental illnesses.) An estimated 10 – 15% of people with anorexia or bulimia are males
 An estimated 10 – 15% of people with anorexia or bulimia are males")
20
MORTALITY RATES Eating disorders have the highest mortality rate of any mental illness A study by the National Association of Anorexia Nervosa and Associated Disorders reported that 5 – 10% of anorexics die within 10 years after contracting the disease; 18-20% of anorexics will be dead after 20 years and only 30 – 40% ever fully recover The mortality rate associated with anorexia nervosa is 12 times higher than the death rate of ALL causes of death for females 15 – 24 years old. 20% of people suffering from anorexia will prematurely die from complications related to their eating disorder, including suicide and heart problems

21
Obesity http://www.cyberdiet.com A disorder characterized by being excessively overweight. Obesity increases the risk for health issues like cardiovascular diseases, diabetes, hypertension, arthritis, and back problems.

22
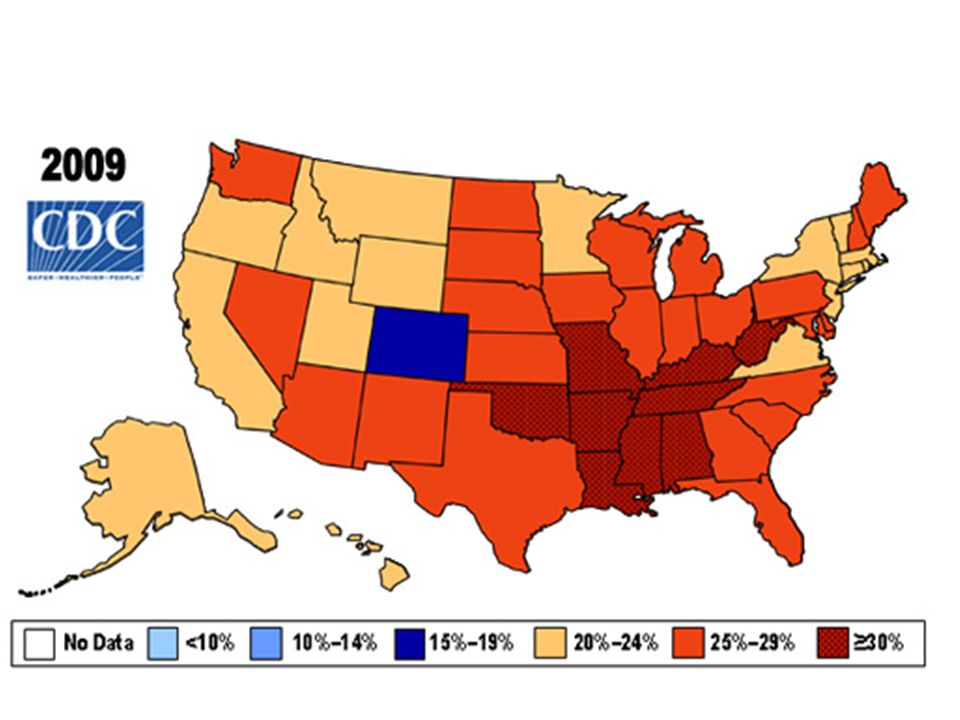
Latest Obesity Statistics USA Obesity Rates Reach Epidemic Proportions 58 Million Overweight; 40 Million Obese; 3 Million morbidly Obese Eight out of 10 over 25's Overweight 78% of American's not meeting basic activity level recommendations 25% completely Sedentary 76% increase in Type II diabetes in adults 30-40 yrs old since 1990

23
Obesity Related Diseases 80% of type II diabetes related to obesity 70% of Cardiovascular disease related to obesity 42% breast and colon cancer diagnosed among obese individuals 30% of gall bladder surgery related to obesity 26% of obese people having high blood pressure

24
Childhood Obesity Running Out of Control 4% overweight 1982 | 16% overweight 1994 25% of all white children overweight 2001 33% African American and Hispanic children overweight 2001 Hospital costs associated with childhood obesity rising from $35 Million (1979) to $127 Million (1999)
 to $127 Million (1999)")
25
Regulating Weight When a person’s weight drops or increases, the body responds by adjusting hunger and energy use to bring weight back to its initial stable amount. Most mammals, without consciously regulating, have a stable weight to which they keep returning. This is also known as their set point. A person’s set point might rise with age, or change with economic or cultural conditions. Therefore, this “set point” of stable weight is more of a current but temporary “settling point.”

26
Which foods to eat? Taste Preferences Some taste preferences are universal. Carbohydrates temporarily raise levels of serotonin, reducing stress and depression. Other tastes are acquired and become favorites through exposure, culture, and conditioning. Different cultures encourage different tastes. Some cultures find these foods to be delicious: reindeer fat and berries, or roasted guinea pig.

27
Biology, Evolution, and Taste Preferences Differences in taste preferences are not arbitrary. Personal and cultural experience, influenced by biology, play a role. We can acquire a food aversion after just one incident of getting sick after tasting a food. It is adaptive in warm climates to develop a taste for salt and spice, which preserve food. Disliking new tastes may have helped to protect our ancestors.

28
How much do we eat? Eating depends in part on situational influences. Social facilitation: the presence of others accentuates our typical eating habits Unit bias: we may eat only one serving/unit (scoop, plateful, bun-full) of food, but will eat more if the serving size is larger Buffet effect: we eat more if more options are available
 of food, but will eat more if the serving size is larger Buffet effect: we eat more if more options are available.")
29
Influences on Eating Behavior

30
Variations from the Norm of Body Weight In some cases, the set point of a person’s body weight drifts from a healthy weight. Psychological disorders of eating can override this set point, ignore biological signals, and lead to extreme weight loss. In other cases, the set point seems to drift upward. Biological tendencies can lead to increased weight that is hard to lose, leading to obesity.

31
Obesity is linked to diabetes, heart problems, arthritis, and some cancers. Obesity refers to an amount of body fat that increases the risk of health problems to the point that weight loss is a health priority.

32
Is Fat Bad? Having some body fat is normal and healthy; fat stores energy effectively for later use. Body fat has been seen as a sign of affluence, and thus has been considered attractive. Standards vary in different cultures, sometimes creating an unhealthy norm of being overweight or underweight. Being mildly overweight is not considered a problem if the person is in good physical condition or exercising.

33
Obesity and Life Expectancy

34
How does obesity develop, and why is it hard to change? It was adaptive for our ancestors to crave energy-rich food when available. Problem: energy-rich ‘junk’ food is now easily available, and cheaper than healthy food It is adaptive to slow down our burning of fat when food is scarce. Problem: in poverty or in crash diets, our body can slow down weight loss Obesity and Weight Control Physiology of Obesity Once a person is obese, losing weight is not so easy as “just eating less.” Fat has a lower metabolic rate then other tissue, so a person might gain weight when eating “normally.” Eating less to lose weight slows metabolism. This prevents weight loss, and ensures weight gain when returning to a normal diet. Even if weight loss succeeds, a formerly obese person will have to eat less than an average person just to prevent weight gain.

35
Genetics and Obesity Adopted siblings eating the same meals end up with a BMI/weight resembling biological parents, not people in the same household. Identical twins have similar weights, even when raised apart with different food. There seem to be many genes with effects on weight. Lifestyle Factors and Obesity People who are restless and fidgeting burn off more calories and gain less weight than others. Inadequate sleep causes weight gain, despite increased active time, because of appetite hormones. Having an obese friend correlates with becoming obese. Sedentary lifestyles and fast food may be leading to increased body fat worldwide. Social Psychology of Obesity Discrimination based on weight has been found to be stronger than race and gender discrimination. In one study, actors were seen as less employable when made to look heavier. Even children are prejudiced against the overweight. Perhaps as a result, people who are obese are more likely to be depressed or isolated.

36
Losing Weight: The Challenge If you decide to move your body’s set point to a lower body weight: Because of the physiological factors and perhaps due to lifestyle and peer issues: once obese, weight loss is difficult, and permanent weight loss is even harder. obsessive weight loss attempts can add to shame, anxiety, depression, and disordered eating habits. Begin with an understanding of the metabolic challenges you face, so that you blame slow progress on physiology, not poor willpower. Begin with self-acceptance and a decision to change, rather than feeling shame. Make gradual and consistent, not drastic and varying, lifestyle changes. Increase exercise and healthy food choices. Get support. Losing Weight: The Plan

37
Reasons for Eating Disorders 1.Sexual Abuse: Childhood sexual abuse does not cause eating disorders. 2.Family: Younger generations develop eating disorders when raised in families in which weight is an excessive concern. 3.Genetics: Twin studies show that eating disorders are more likely to occur in identical twins rather than fraternal twins.

38
Body Image (Women) Western culture tends to place more emphasis on a thin body image in comparison to other cultures.
 Western culture tends to place more emphasis on a thin body image in comparison to other cultures.")
39
Summary

Similar presentations







 was an American scientist who studied the influence of diet on health. He conducted.>")


 David Myers PowerPoint Slides Worth Publishers, © 2007.>")








