Download presentation
Presentation is loading. Please wait.

1
Integration Unit 2016 Malignant Pain Assessment & Management Dr. Khadija Bhimji kbhimji@ottawahospital.on.ca You may only access and use this PowerPoint presentation for educational purposes. You may not post this presentation online or distribute it without the permission of the author

2
Outline the WHO approach to the management of cancer pain Describe an approach to comprehensive pain assessment in palliative care Describe the specific pharmacokinetic and pharmacodynamic properties when choosing opioids for patients at the end of life Describe common side effects of opioids and an approach to their management that anticipates and prevents these Describe and deal with patient and family concerns or myths about opioid use at the end-of-life Explain the concepts of tolerance, physical dependence and addiction as they relate to the use of opioids in palliative care Discuss routes of administration of opioids Describe the use of adjuvant medications and other modalities in pain management Objectives [Integration Unit – Malignant Pain Assessment and Management – Dr. Khadija Bhimji]

3
58 yr old MBC x 2 years Treated with chemo, radiation Disease progression Pain Back pain primarily Shoots down spine, into legs Right posterior flank pain also Trouble ambulating Needs walker; W/C for distance, such as coming to clinic today Sue [Unit name – Lecture title – Prof name]
![ 58 yr old MBC x 2 years Treated with chemo, radiation Disease progression Pain Back pain primarily Shoots down spine, into legs Right posterior flank pain also Trouble ambulating Needs walker; W/C for distance, such as coming to clinic today Sue [Unit name – Lecture title – Prof name]](http://images.slideplayer.com/34/10183016/slides/slide_3.jpg " 58 yr old MBC x 2 years Treated with chemo, radiation Disease progression Pain Back pain primarily Shoots down spine, into legs Right posterior flank pain also Trouble ambulating Needs walker; W/C for distance, such as coming to clinic today Sue [Unit name – Lecture title – Prof name]")
4
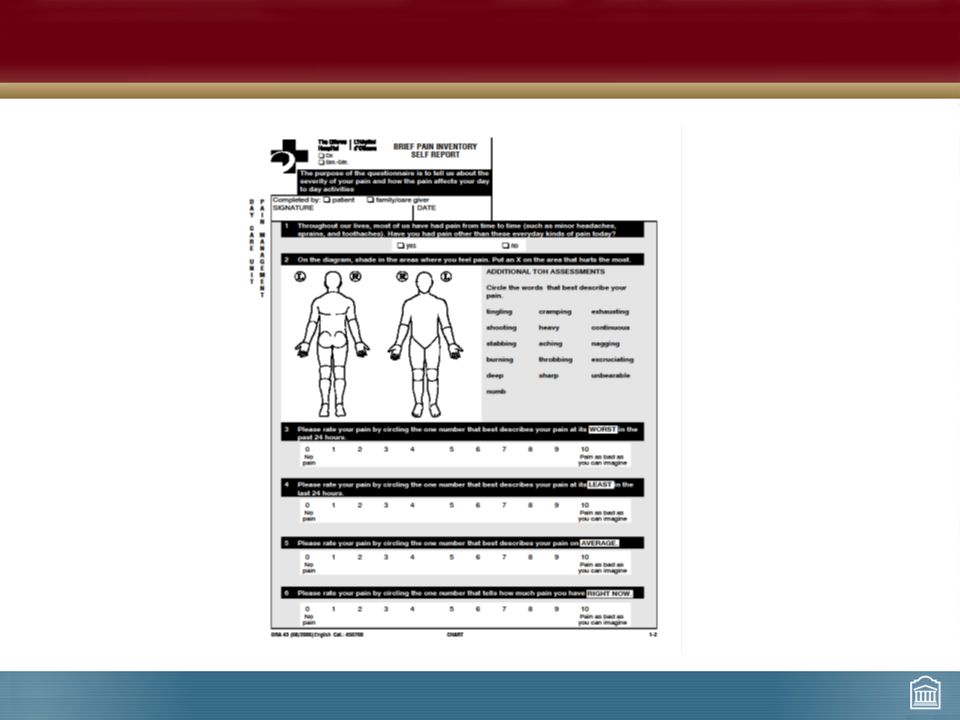
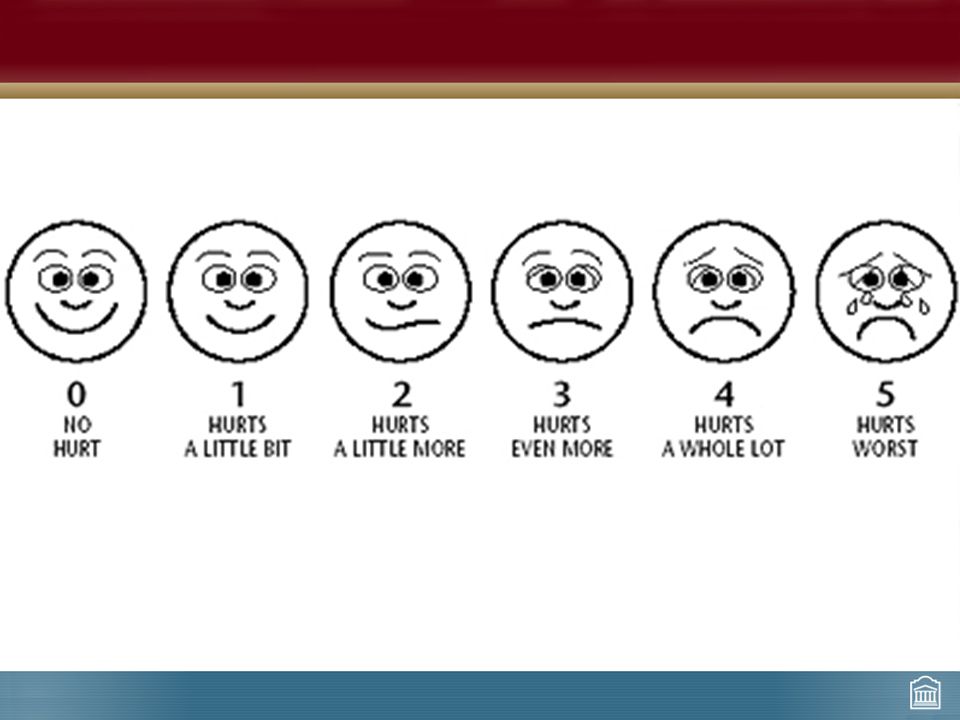
Pain Assessment Comprehensive pain history – Essential for analgesic strategy General description – PQRST – Location – Intensity (ESAS, BPI = NRS) Effect of meds Effect on ADLs, sleep
 Effect of meds Effect on ADLs, sleep")
7
http://www.youtube.com/watch?v=UM-HWkbnDfg Pain Assessment…

8
The Pain Experience Complex! Meaning of the pain – Is she worried about etiology? – What it means about her illness? Influenced by emotional, sociocultural and spiritual context of individual Important to be sensitive to this in assessment and treatment

9
Total Pain

10
Physical Exam Focussed – Identify source of pain Investigations as appropriate – Will they help identify source of pain? – Will management change?

11
Classify Pain Nociceptive Neuropathic Visceral Somatic

12
Sue Tylenol #3 constipating, makes her feel “mixed up” – Can’t concentrate on her reading, or needlepoint No relief with advil any longer “Not ready for Morphine” – Saw what it did to her grandmother

13
Addiction, Dependence, & Tolerance Ask Normalize Explain Emphasize the difference between physical dependence, addiction (psychological dependence), and tolerance
, and tolerance")
14
Physical Dependence Normal physiological response to the pharmacological effects of chronic opioid use Body adapts to presence of opioid such that withdrawal symptoms seen if opioid suddenly stopped/naloxone given – Sweating, tremors, agitation, muscle cramps, abdominal cramps, tachycardia, fever, dilated pupils

15
Tolerance Normal physiological phenomenon Increasing doses of opioid required over time to produce same analgesic effect Mechanism? COMPLEX! – Thought to be related to changes in opioid receptors or drug metabolism Degree and rate to which tolerance develops varies greatly between different opioids and individuals

16
Addiction Pathologic psychological condition Compulsion to take drug(s) to experience its psychic effects (euphoria, being “high” or “spaced out”) Studies show cancer patients receiving opioids for cancer pain DO NOT become psychologically dependent (addicted)
 to experience its psychic effects (euphoria, being high or spaced out ) Studies show cancer patients receiving opioids for cancer pain DO NOT become psychologically dependent (addicted)")
17
WHO Pain Ladder

18
WHO Analgesic Ladder Step 1: Mild Pain – Use a non-opioid analgesic – ASA, Acetaminophen, NSAID Step 2: Moderate Pain – Use a “weak” opioid – Tramadol (maybe), low doses opioid Step 3: Severe Pain – Use a “strong” opioid – Morphine, Hydromorphone, Oxycodone, Fentanyl – Codeine (prodrug – metabolized to morphine) AVOID DEMEROL!!!
, low doses opioid Step 3: Severe Pain – Use a strong opioid – Morphine, Hydromorphone, Oxycodone, Fentanyl – Codeine (prodrug – metabolized to morphine) AVOID DEMEROL!!!")
19
Tramadol Minimal opioid effect – Poor Mu receptor affinity – SNRI effect Caution if administered with other SSRIs, SNRIs, MAO inhibitors – Serotonin syndrome Starting dose usually 50 (to 100) mg q6h Long acting formulations available
 mg q6h Long acting formulations available")
20
Opioids in Cancer Pain Morphine – Principal opioid used for moderate or severe pain – Gold standard against which all others are measured Morphine, hydromorphone, codeine – Available po, parenteral (iv/sc) Tramadol, tapentadol, oxycodone – PO only All have active metabolites which accumlate in RF – dose, interval in RF Fentanyl – iv/sc or transdermal only – No active metabolites
 Tramadol, tapentadol, oxycodone – PO only All have active metabolites which accumlate in RF – dose, interval in RF Fentanyl – iv/sc or transdermal only – No active metabolites")
21
Dosing of Opioids Half-life po/sc = 4hrs (immediate release) Time to peak effect – Oral dose peaks in approx. 90 minutes – SC dose peaks in approx. 45 minutes Only fentanyl SHORT half life < 1hr – Must be given as continuous dosing (IV/SC/TD) Time to peak effect = 5-10 mins (iv) or 20 mins (sc) Consider long acting formulation ONLY when pain is well controlled
 Time to peak effect = 5-10 mins (iv) or 20 mins (sc) Consider long acting formulation ONLY when pain is well controlled.")
22
Drug ORAL DOSE (mg)PARENTERAL DOSE (mg) Morphine2010 Codeine200100 Oxycodone10- Meperidine200-30075 Hydromorphone42 Fentanyl-DRUG Equianalgesic Table Fentanyl dose is calculated by first converting the opioid to the equianalgesic dose of oral morphine. Fentanyl patch at 25 ucg/hr = Hydromorphone 20 mg; Oxycodone 50 mg; Morphine 100 mg; Tramadol 500 mg (oral equivalent in 24 hours)
.")
23
Commencing Opioids 1.Discuss opioid fears and misapprehension with patient: “Morphine Myths” 2.Prescribe a “rescue” dose of IR opioid for ‘breakthrough’ or ‘episodic’ pain (10% of total daily dose) 3.See ‘Opioid Equivalency’ table on One45
 3.See ‘Opioid Equivalency’ table on One45")
24
What Route? ORAL route is first choice Alternate routes if unable to take oral meds – Rectal Morphine, hydromorphone, methadone Safe, inexpensive, effective Not popular with all patients! Not suitable if anorectal lesions, thrombocytopenia, neutropenia – Transdermal Non-invasive, convenient Cannot take po Suitable if pain well controlled on stable dose opioids

25
What Route? Parenteral – More invasive IV – rarely, although absorbed faster than sc SC – preferred to iv as just as effective, easier to maintain, more comfortable, less expensive IM – NEVER! Uncomfortable, erratic absorption, no advantage over sc Spinal

26
Indications for SC Route Intestinal obstruction Severe pain requiring urgent intervention Dysphagia Intractable N/V Diminished GI absorption Terminal care

27
COMMONUNCOMMON NauseaPruritis VomitingUrinary Retention ConstipationMyoclonus SedationRespiratory Depression ConfusionSeizures Dry MouthSweating Postural Hypotension Side Effects of Opioids

28
Teaching Point Anticipate side effects Educate patient to expect possible side effects, what to expect, how to manage

29
Managing Opioid Side Effects Constipation – Prevention! Tolerance to constipation never develops Always prescribe regular laxatives – Increase dose laxatives when opioid doses substantially increased

30
Managing Opioid Side Effects Expect N/V to resolve within few days – Metoclopramide 5-10 mg po/sc/iv q4h prn Dry Mouth – Other drugs may contribute! – Rx: sugar free candies Urinary retention – Usually transient – +/- Foley catheter

31
Managing Opioid Side Effects Neurotoxic side effects primarily due to accumulation of active opioid metabolites – Sedation – Myoclonus – Delirium / hallucinations – Hyperalgesia

32
Managing Opioid Side Effects Rx: – Hydration – R/O underlying aggravating metabolic factors – Rx symptoms – Opioid rotation or dose reduction BEWARE: Sepsis can enhance toxicity!

33
Managing Opioid Side Effects Respiratory depression – RARE! Tolerance to respiratory depression develops within 24 hours Patients on opioids over long periods develop tolerance to respiratory depressant effects – Large doses opioids have little effect on respiration Naloxone if indicated

34
Medication Type Mechanism of Action Indication Steroids Inhibits inflammatory response to tissue damage Peritumor edema Spontaneous discharge injured nerve SCC ICP Neuropathic pain AEDs (Gabapentin, pregabalin) Spontaneous nerve discharge Block voltage dependent Na + channels ?effect on Ca 2+ channels GABA agonism (selective AEDs) ?NMDA antagonism (selective) Neuropathic pain TCAs, SNRIs (Nortriptyline, duloxetine, venlafaxine) MAO activity in descending pain-modulating pathways Neuropathic pain Adjuvant Medications
 Spontaneous nerve discharge Block voltage dependent Na + channels effect on Ca 2+ channels GABA agonism (selective AEDs) NMDA antagonism (selective) Neuropathic pain TCAs, SNRIs (Nortriptyline, duloxetine, venlafaxine) MAO activity in descending pain-modulating pathways Neuropathic pain Adjuvant Medications")
35
Medication Type Mechanism of Action Indication Bisphosphonates Inhibits osteoclast activityBone pain NMDA Receptor Antagonists Inhibits action of glutamate in dorsal horn by inhibiting NMDA receptor (responsible for functional alterations in central transmission of pain, resulting in opioid tolerance, neurotoxicity, and neuropathic pain): Ketamine, methadone Neuropathic pain Opioid-induced neurotoxicity ?High opioid tolerance Other SNRIs (duloxetine, venlafaxine) Cannabinioids Interrupts pain transmission Neuropathic pain Adjuvant Medications
: Ketamine, methadone Neuropathic pain Opioid-induced neurotoxicity High opioid tolerance Other SNRIs (duloxetine, venlafaxine) Cannabinioids Interrupts pain transmission Neuropathic pain Adjuvant Medications")
36
Palliative radiation Interventional analgesia Other Modalities in Pain Management

37
= Subarachnoid Ligamentum flavum Dura & arachnoid Layers (thecal sac) CSF
 CSF")
38
Port-a-cath (Intrathecal) PORT INTRATHECAL CATHETER RUBBER SEPTUM INTERNAL CONNECTOR CADD PUMP SC IT CATHETER GRIPPER PORT
 PORT INTRATHECAL CATHETER RUBBER SEPTUM INTERNAL CONNECTOR CADD PUMP SC IT CATHETER GRIPPER PORT")
39
In Summary… Select the appropriate analgesic drug Prescribe appropriate dose of drug Administer drug by appropriate route Schedule appropriate dosing interval Prevent persistent pain Relieve breakthrough pain Titrate dose of drug aggressively Prevent, anticipate, and manage side effects Use appropriate adjuvant drugs

Similar presentations








. For CHRONIC pain, use a scheduled medication regimen. ( ex:>")



 Jason.>")

 Medical University of Sofia, Faculty of Medicine Department of Pharmacology and Toxicology.>")




