Download presentation
Presentation is loading. Please wait.

1
Rickets The objectives of this lecture is to know the: Definition Causes and types Clinical presentation Radiological and lab.findings Treatment prognosis

2
General: Bone consists of a protein matrix called osteoid and a mineral phase, principally composed of calcium and phosphate, mostly in the form of hydroxyapatite. Osteomalacia is present when there is inadequate mineralization of bone osteoid; it occurs in children or adults. Rickets, a disease of growing bone, occurs in children only before fusion of the epiphyses, and is due to unmineralized matrix at the growth plates. Etiology: There are many causes of rickets including vitamin D disorders, calcium deficiency, phosphorous deficiency, and distal renal tubular acidosis.

3
Causes of Rickets VITAMIN D DISORDERS *Nutritional vitamin D deficiency *Congenital vitamin D deficiency *Secondary vitamin D deficiency: Malabsorption, Decreased liver 25-hydroxylase *Vitamin D–dependent rickets type 1 *Vitamin D–dependent rickets type 2 *Chronic renal failure CALCIUM DEFICIENCY *Low intake : Diet, Premature infants (rickets of prematurity) *Malabsorption : Primary disease, Dietary inhibitors of calcium absorption
 *Malabsorption : Primary disease, Dietary inhibitors of calcium absorption")
4
PHOSPHORUS DEFICIENCY *Inadequate intake * Premature infants (rickets of prematurity) * Aluminum-containing antacids * Renal loss X-linked hypophosphatemic rickets Autosomal dominant hypophosphatemic rickets Hereditary hypophosphatemic rickets with hypercalciuria Tumor-induced rickets McCune-Albright syndrome Neurofibromatosis Fanconi syndrome DISTAL RENAL TUBULAR ACIDOSIS.
 * Aluminum-containing antacids * Renal loss X-linked hypophosphatemic rickets Autosomal dominant hypophosphatemic rickets Hereditary hypophosphatemic rickets with hypercalciuria Tumor-induced rickets McCune-Albright syndrome Neurofibromatosis Fanconi syndrome DISTAL RENAL TUBULAR ACIDOSIS.")
5
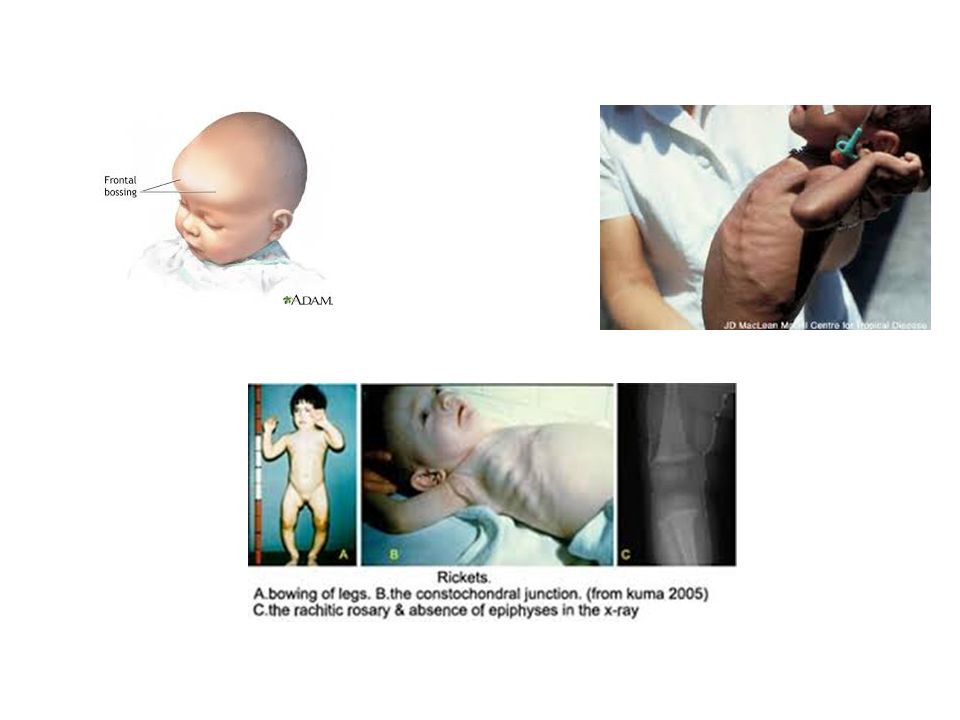
Clinical Features of Rickets GENERAL Failure to thrive, sweating,Protruding abdomen Muscle weakness (especially proximal), Fractures. HEAD Craniotabes,Frontal bossing,Delayed fontanels closure Delayed dentition; dental caries. CHEST Rachitic rosary,Harrison groove,Respiratory infections and atelectasis BACK Scoliosis,Kyphosis,Lordosis EXTREMITIES Enlargement of wrists and ankles,Valgus or varus deformities Anterior bowing of the tibia and femur, Leg pain. HYPOCALCEMIC SYMPTOMS Tetany,Seizures,Stridor due to laryngeal spasm

8
*There is some variation in the clinical presentation of rickets based on the etiology. Changes in the lower extremities tend to be the dominant feature in X-linked hypophosphatemic rickets. Symptoms secondary to hypocalcemia occur only in those forms of rickets associated with decreased serum calcium. *The chief complaint in a child with rickets is quite variable. Many children present because of skeletal deformities, whereas others may have difficulty walking due to a combination of deformity and weakness. Other common presenting complaints include failure to thrive

9
Radiology: Rachitic changes are most easily visualized on posteroanterior radiographs of the wrist, although characteristic rachitic changes can be seen at other growth plates. The edge of the metaphysis loses its sharp border, which is described as fraying. In addition, the edge of the metaphysis changes from a convex or flat surface to a more concave surface This is termed cupping, and is most easily seen at the distal ends of the radius, ulna, and fibula. There is widening of the distal end of the metaphysis, corresponding to the clinical observation of thickened wrists and ankles, as well as the rachitic rosary. Other radiologic features include coarse trabeculation of the diaphysis and generalized rarefaction.

11
Diagnosis: Most cases of rickets are diagnosed based on the presence of classic radiographic abnormalities. The diagnosis is supported by physical examination findings and a history and laboratory test results that are consistent with a specific etiology. Clinical Evaluation: *Because the majority of children with rickets have a nutritional deficiency, the initial evaluation should focus on a dietary history, emphasizing intake of vitamin D and calcium. *Cutaneous synthesis mediated by sunlight exposure is an important source of vitamin D. It is important to ask about time spent outside, and clothing. winter sunlight is ineffective at stimulating cutaneous synthesis of vitamin D. Children with increased skin pigmentation are at increased risk for vitamin D deficiency because of decreased cutaneous synthesis.

12
*The presence of maternal risk factors for nutritional vitamin D deficiency, including diet and sun exposure, is an important consideration when a neonate or young infant has rachitic findings, especially if the infant is breast-fed (congenital rickets) *The child's medication use is relevant because certain medications, such as the anticonvulsants phenobarbital and phenytoin, increase degradation of vitamin D, and aluminum-containing antacids interfere with the absorption of phosphate. *Malabsorption of vitamin D is suggested by a history of liver or intestinal disease. There may be signs or symptoms suggestive of deficiencies of other fat-soluble vitamins (A, E, and K). *A history of renal disease (proteinuria, hematuria, urinary tract infections) is an additional significant consideration, given the importance of chronic renal failure as a cause of rickets. *The family history is important, as there is large number of genetic causes of rickets, although most are rare.
. *A history of renal disease (proteinuria, hematuria, urinary tract infections) is an additional significant consideration, given the importance of chronic renal failure as a cause of rickets. *The family history is important, as there is large number of genetic causes of rickets, although most are rare..")
13
The physical examination focuses on detecting manifestations of rickets. *It is important to observe the child's gait, auscultate the lungs to detect atelectasis or pneumonia, and plot the patient's growth. Alopecia suggests vitamin D–dependent rickets type 2. The initial laboratory tests serum calcium; phosphorus; alkaline phosphatase; parathyroid hormone (PTH); 25-hydroxyvitamin D; 1, 25-dihydroxyvitamin D 3 ; creatinine; and electrolytes. Other investigations done according to the suspected etiology of rickets, for example; Urinalysis is useful for detecting the glycosuria and aminoaciduria seen with Fanconi syndrome.
; 25-hydroxyvitamin D; 1, 25-dihydroxyvitamin D 3 ; creatinine; and electrolytes. Other investigations done according to the suspected etiology of rickets, for example; Urinalysis is useful for detecting the glycosuria and aminoaciduria seen with Fanconi syndrome..")
14
NUTRITIONAL VITAMIN D DEFICIENCY : the most common cause of rickets Etiology: *Vitamin D deficiency most commonly occurs in infancy due to a combination of poor intake and inadequate cutaneous synthesis. *Transplacental transport of vitamin D, typically provides enough vitamin D for the 1st 2 mo of life unless there is severe maternal vitamin D deficiency. Breast-fed infants, because of the low vitamin D content of breast milk, rely on cutaneous synthesis or vitamin supplements. *Cutaneous synthesis can be limited due to the ineffectiveness of the winter sun in stimulating vitamin D synthesis; avoidance of sunlight due to cultural practices; and decreased cutaneous synthesis because of increased skin pigmentation. *Infants who receive formula receive adequate vitamin D, even without cutaneous synthesis.

15
Clinical Manifestations: The clinical features are typical of rickets mentioned earlier with a significant minority presenting with symptoms of hypocalcemia; In addition, these children have an increased risk of pneumonia and muscle weakness, leading to a delay in motor development. Laboratory Findings: Hypocalcemia is a variable finding due to the actions of the elevated PTH to increase the serum calcium concentration. The hypophosphatemia is due to PTH-induced renal losses of phosphate, combined with a decrease in intestinal absorption. The wide variation in 1,25-D levels (low, normal, or high) is secondary to the upregulation of renal 1α-hydroxylase due to concomitant hypophosphatemia and hyperparathyroidism. The level of 1,25-D is only low when there is severe vitamin D deficiency. S. Alkaline phosphatase is high. PTH level is high.
 is secondary to the upregulation of renal 1α-hydroxylase due to concomitant hypophosphatemia and hyperparathyroidism. The level of 1,25-D is only low when there is severe vitamin D deficiency. S. Alkaline phosphatase is high. PTH level is high..")
16
Diagnosis The diagnosis of nutritional vitamin D deficiency is based on the combination of a history of poor vitamin D intake and risk factors for decreased cutaneous synthesis, radiographic changes consistent with rickets, and typical laboratory findings. Treatment: Children with nutritional vitamin D deficiency should receive vitamin D and adequate nutritional intake of calcium and phosphorus. 1) There are 2 strategies for administration of vitamin D: 300,000–600,000 IU of vitamin D is administered orally or intramuscularly as 2–4 divided doses over 1 day. Because the doses are observed, this is ideal in situations where adherence to therapy is questionable. The alternative is daily, high-dose vitamin D, with doses ranging from 2,000– 5,000 IU/day over 4–6 wk. Either strategy should be followed by daily vitamin D intake of 400 IU/day, typically given as a multivitamin
 There are 2 strategies for administration of vitamin D: 300,000–600,000 IU of vitamin D is administered orally or intramuscularly as 2–4 divided doses over 1 day. Because the doses are observed, this is ideal in situations where adherence to therapy is questionable. The alternative is daily, high-dose vitamin D, with doses ranging from 2,000– 5,000 IU/day over 4–6 wk. Either strategy should be followed by daily vitamin D intake of 400 IU/day, typically given as a multivitamin.")
17
. 2) It is important to ensure that children receive adequate dietary calcium and phosphorus; this is usually provided by milk formula, and other dairy products. *Children who have symptomatic hypocalcemia may need intravenous calcium acutely, followed by oral calcium supplements, which typically can be tapered over 2–6 wk in children who receive adequate dietary calcium. Prognosis: Most children have an excellent response to treatment, with radiologic healing occurring within a few months. Laboratory test results should also normalize rapidly. Many of the bone malformations improve dramatically, but children with severe disease may have permanent deformities. Prevention: Most cases of nutritional rickets can be prevented by universal administration of a daily multivitamin containing 400 IU of vitamin D to children who are breast-fed. For other children, the diet should be reviewed to ensure that there is a source of vitamin D.

18
CONGENITAL VITAMIN D DEFICIENCY: Congenital rickets, occurs when there is severe maternal vitamin D deficiency during pregnancy. Maternal risk factors include poor dietary intake of vitamin D, lack of adequate sun exposure, and closely spaced pregnancies. These newborns may have symptomatic hypocalcemia, intrauterine growth retardation, and decreased bone ossification, along with classic rachitic changes, and predispose infants to neonatal hypocalcemic tetany. Treatment of congenital rickets includes vitamin D supplementation and adequate intake of calcium and phosphorus.

19
Thank you

Similar presentations

















 Vitamin D 2 : Ergosterol (pro D 2 ) Ergocalciferol (D 2 ) added to milk and dairy. (Human) Vitamin D 3 : Pro (7-dehydrocholesterol)>")



 Defective Bone Formation Inadequate mineralization of osteoid (RICKETS) Defective osteoid.>")