Download presentation
Presentation is loading. Please wait.

1
Thromboprophylaxis in pregnancy: Cardiff and Vale’s approach and the reasons why Rachel Rayment, Consultant Haematologist, UHW Rachel.Rayment@wales.nhs.uk

2
My remit: Share your DVT risk assessment tool highlighting the change in BMI upper threshhold Explain the knowledge behind and the justification for changes in BMI Implementation of the tool/measures of compliance Clinical feedback to the tool………

3
…………….In 20 minutes, allowing time for questions………..

4
The risk assessment tool

5
Tick if present Previous DVT/PE Refer to haematology clinic Antithrombin deficiency Refer to haematology clinic Systemic lupus erythematosis Refer to haematology clinic Sickle cell disease Refer to haematology clinic Antiphospholipid syndrome Refer to haematology clinic Myeloproliferative disorder Refer to haematology clinic BMI ≥45kg/m 2 Refer to anaesthetic clinic @ 32/40 if booking BMI ≥ 45 Assessed by Date / Signature Indications to consider antenatal thromboprophylaxis (continue during hospital admission) THROMBOPROPHYLAXIS RISK ASSESSMENT FOR PREGNANT WOMEN Medical staff to assess ALL women at their first hospital antenatal clinic visit
 THROMBOPROPHYLAXIS RISK ASSESSMENT FOR PREGNANT WOMEN Medical staff to assess ALL women at their first hospital antenatal clinic visit")
6
Indications for thromboprophylaxis (TEDS & Clexane) whilst antenatal inpatient (Medical staff to assess at each antenatal admission) Indication One tick = Thromboprophylaxis required Tick if present Hyperemesis Booking BMI ≥35kg/m 2 Dehydration with dry tongue / poor urine output Sepsis Immobility – >3 days bed rest Significant medical co-morbidity (such as heart disease, metabolic, endocrine or respiratory pathologies, acute infectious diseases or inflammatory conditions) Varicose veins with phlebitis Active cancer / cancer treatment Ongoing antenatal thromboprophylaxis Thromboprophylaxis required (Yes/No) Date Signature
 whilst antenatal inpatient (Medical staff to assess at each antenatal admission) Indication One tick = Thromboprophylaxis required Tick if present Hyperemesis Booking BMI ≥35kg/m 2 Dehydration with dry tongue / poor urine output Sepsis Immobility – >3 days bed rest Significant medical co-morbidity (such as heart disease, metabolic, endocrine or respiratory pathologies, acute infectious diseases or inflammatory conditions) Varicose veins with phlebitis Active cancer / cancer treatment Ongoing antenatal thromboprophylaxis Thromboprophylaxis required (Yes/No) Date Signature")
7
Prescription of Thromboprophylaxis: Booking Weight (kg) Enoxaparin dose (mg) frequency <5020od 50-10040od 101-12040bd >12060bd
 Enoxaparin dose (mg) frequency <5020od od bd >12060bd")
8
Contraindications to Enoxaparin (CLEXANE) 1. Birth or spinal or epidural analgesia / anaesthesia anticipated within next 12 hours 5. DIC 2. Wait 6 hours following performing spinal or epidural analgesia / anaesthesia or epidural catheter removal 6. Past history of heparin-induced thrombocytopenia (discuss with haematologist) 3. Do not remove epidural catheter within 12 hours of Clexane administration. (If on > 40mg discuss with anaesthetist) 7. Patient is already receiving other anticoagulants (e.g. warfarin/heparin) 3. Active bleeding8. Severe liver disease 4. Platelet count < 75 x 10 9 /l 9. Severe renal impairment: If eGFR < 30ml/min or evidence of acute renal failure use subcutaneous unfractionated heparin 5000u bd Consider below knee antiembolism stockings alone if enoxaparin is contraindicated and thromboprophylaxis needed. Avoid stocking if pedal pulses are impalpable, peripheral vascular disease, severe dermatitis, peripheral neuropathy, recent skin graft
 3. Do not remove epidural catheter within 12 hours of Clexane administration. (If on > 40mg discuss with anaesthetist) 7. Patient is already receiving other anticoagulants (e.g. warfarin/heparin) 3. Active bleeding8. Severe liver disease 4. Platelet count < 75 x 10 9 /l 9. Severe renal impairment: If eGFR < 30ml/min or evidence of acute renal failure use subcutaneous unfractionated heparin 5000u bd Consider below knee antiembolism stockings alone if enoxaparin is contraindicated and thromboprophylaxis needed. Avoid stocking if pedal pulses are impalpable, peripheral vascular disease, severe dermatitis, peripheral neuropathy, recent skin graft.")
9
Postnatal Ensure thromboprophylaxis (TEDS & Clexane for 5 days) has been prescribed following birth if one or more factor present Tick if present Women receiving thromboprophylaxis throughout pregnancy should continue treatment for 6 weeks postpartum PPH >1500ml Red blood cell transfusion or transfusion of coagulation factors Caesarean section (elective or emergency) Still-birth BMI >40kg/m 2 Sepsis Complex vaginal delivery (Thromboprophylaxis should be considered) Signature / Date Prescription of Thromboprophylaxis: Booking Weight (kg) Enoxaparin dose (mg) frequencyConsider below knee antiembolism stockings alone if enoxaparin is contraindicated. Avoid stocking if pedal pulses are impalpable, peripheral vascular disease, severe dermatitis, peripheral neuropathy, recent skin graft <5020od 50-10040od 101-12040bd >12060bd

10
CMACE 2006-2008 - saving mother’s lives Deaths18 BMI >3011 Learning difficulties / mental health disorder 5 Minority ethnic group6 (2 spoke no English) Hyperemesis3 Prolonged immobility2
 Hyperemesis3 Prolonged immobility2")
11
CEMACE 2003-5 Risk factors – all deaths n=33 BMInumber% >251676 >301248 >35838 >45629 >6025 Weight recorded 25 BMI calculated in 21

12
Welsh Health Survey 2008 57% of adults in Wales are overweight or obese 19% of adults in Wales are overweight or obese

13
Pregnancy associated DVT: Cardiff and Vale 2010 Antenatal: 3 –1@ 37 weeks in a 21 year old with no risk factors –1@29 weeks in a 23 year old with no risk factors –1@7-8 weeks in a 33 year old with an unplanned pregnancy and a prior history of DVT in pregnancy, not on thromboprophylaxis Up to 6 weeks post-natal: 2 –1@ 5 days post c/s. 28 year old. Ventilated on ITU, adenocarcinoma in pleural aspirate. Patient died. –1@ 28 year old 4 days following SVD of 2nd baby. No complications. No risk factors. >6 weeks <1 year post-natal –1@ 24 yr old 8 weeks post partum. Fractured ankle, immobilised with POP, raised BMI –1@ 28 year old 5 months post partum. No risk factors

14
Cardiff and Vale: Pregnancy related PE’s 2010 Antenatal:1 –33 years old. G6P5. BMI <25. –8 weeks gestation, massive PE requiring thrombolysis Post natal:1 –19 year old. No risk factors (BMI <25). –9 weeks post delivery (1 st symptoms 6-7 weeks)
. –9 weeks post delivery (1 st symptoms 6-7 weeks).")
15
Cardiff and Vale Pregnancy related deaths due to VTE 2010 1

16
Thrombosis in pregnancy – the risk factors

17
Incidence and risk factors for PE in the postpartum period Morris Journal of thrombosis and haemostasis 2010 All deliveries in New South Wales 2001- 2006 510 889 deliveries to 380 459 women 375 episodes of PE Incidence of PE 0.73/1000 deliveries 7 deaths due to PE Mortality 0.013/1000 (CEMACH 0.015/1000)
")
18
Pregnancy/delivery factorAdjuste d OR 95% CI SLE8.833.47-22.5 Transfusion of coagulation factors 8.243.92 – 17.3 Stillbirth in current pregnancy5.973.09-11.6 VTE in a prior birth4.180.49-36.0* Red Cell transfusion3.932.25-6.86 *1 case in 260 PE’s had a history of VTE in previous birth

19
Pregnancy/delivery factorAdjusted OR 95% CI Caesarean section during labour 3.72.67- 5.15 Caesarean section without labour 3.11*2.22- 4.30 Preterm live-birth (<37 weeks)2.181.54- 3.09 Pregnancy hypertension2.061.49- 2.85 *No significant difference between c/s during labour and without labour
 Pregnancy hypertension *No significant difference between c/s during labour and without labour")
20
Pregnancy/delivery factorAdjusted OR 95% CI Parity >31.491.02-2.20 LGA (10 th percentile)1.400.96-2.04 SGA (<10 th percentile)1.230.84-1.81 Smoker1.170.83 -1.65
 SGA (<10 th percentile) Smoker")
21
What is the evidence in favour of thromboprophylaxis in pregnancy?

22
Cochrane review: Prophylaxis for venous thromboembolic disease in pregnancy and the early postnatal period Tooher, Cochrane Database 2010 issue 5

23
13 trials 1774 women 4 trials: antenatal thromboprophylaxis –UFH vs LMWH ( 2 studies) –heparin vs no treatment (2 studies) 8 trials: thromboprophylaxis post c/s –HES v UFH (1 study) –Heparin vs placebo (4 studies) –UFH vs LMWH (3 studies) 1 trial post-natal thromboprophylaxis
 –heparin vs no treatment (2 studies) 8 trials: thromboprophylaxis post c/s –HES v UFH (1 study) –Heparin vs placebo (4 studies) –UFH vs LMWH (3 studies) 1 trial post-natal thromboprophylaxis")
24
Cochrane review conclusion “There is insufficient evidence from RCTs to guide clinical decision making” “Practionners must rely on consensus derived clinical practice guidelines”

25
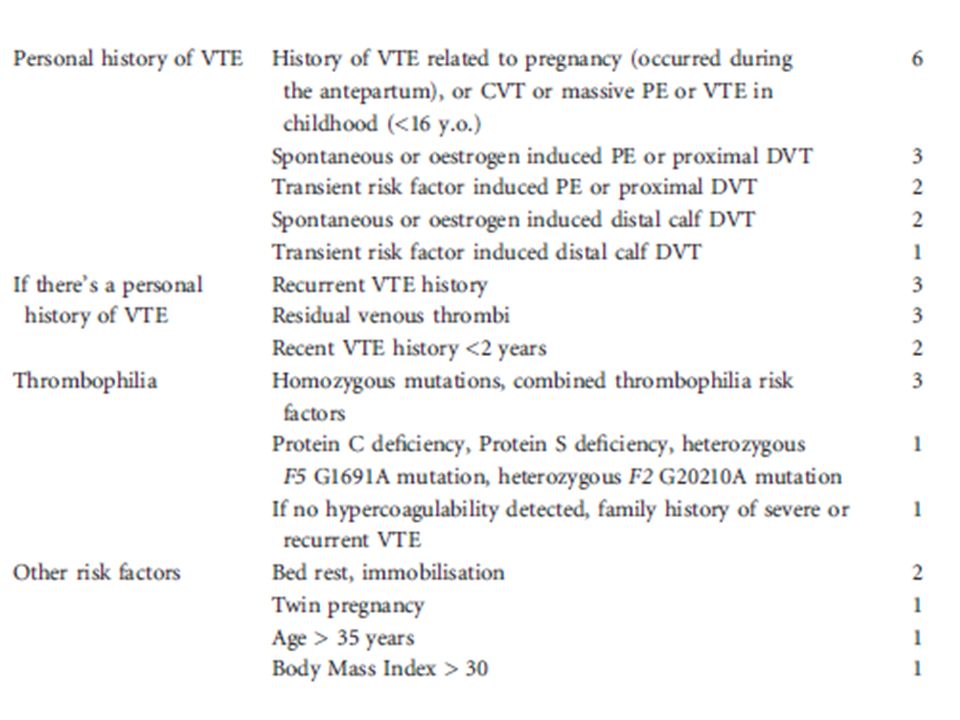
Risk scoring in pregnancy Dargaud BJHaem 2009 Prospective multicentre clinical trial 2005-2007 286 women Personal h/o VTE or Known thrombophilia

27
ScoreAntenatal TPPostnatal TP <3NoYes 3-53 rd trimesterYes >6>6 Clinical management according to risk score

28
Clinical outcomes according to risk score

29
Consider offering LMWH if pregnant woman is admitted and: Expected to be immobile for >3 days Known thrombophilia >35 yearsPersonal history VTE Critical care admission!st degree relative with VTE DehydrationHyperemesis gravidarum Excess blood loss or blood transfusion BMI >30kg/m 2 OHSSPre-Eclampsia Multiple pregnancyVaricose veins with phlebitis NICE guidance- 92, 2010

30
Additional Risk Factors for VTE Thromboprophylaxis following caesarean section? ACCP (grade)NICERCOG (grade) NoneNo (1B)Emergency c/s: 7 days LMWH Emergency c/s: 7 days LMWH (C) > 1 LMWH OR Mechanical Method for duration of hospital stay (2 C) Elective c/s: 7 days LMWH ALL: 7 days LMWH if BMI >40kg/m 2 Elective c/s: 7 days LMWH (C) ALL: 7 days LMWH if BMI >40kg/m 2 (C) Multiple – at very high risk LMWH AND Mechanical Method for duration of hospital stay (2C) Selected patients with persisting risk Extended thromboprophylaxis following discharge (up to 6 weeks) (2C)
NICERCOG (grade) NoneNo (1B)Emergency c/s: 7 days LMWH Emergency c/s: 7 days LMWH (C) > 1 LMWH OR Mechanical Method for duration of hospital stay (2 C) Elective c/s: 7 days LMWH ALL: 7 days LMWH if BMI >40kg/m 2 Elective c/s: 7 days LMWH (C) ALL: 7 days LMWH if BMI >40kg/m 2 (C) Multiple – at very high risk LMWH AND Mechanical Method for duration of hospital stay (2C) Selected patients with persisting risk Extended thromboprophylaxis following discharge (up to 6 weeks) (2C).")
31
Post natal thromboprophylaxis RCOGSIGN >2 persisting risk factorsLMWH for 7 days (C) >3persisting risk factorsAES + LMWH for 7 days (C) BMI >40kg/mLMWH for 7 days (consensus) YES (C) Emergency section (category 1,2 or 3) LMWH for 7 days (C)YES (C) Elective caesarean section + 1 risk factor LMWH for 7 days (C)YES (C) asymptomatic heritable or acquired thrombophilia LMWH at 7 days – 6 weeks (C) YES (C) Women with previous VTELMWH until 6 weeks (C)YES (C) Women receiving LMWH antenatallyLMWH until 6 weeks (C)YES (C) In women who have additional persistent risk factors thromboprophylaxis LMWH up to 6 weeks (consensus)
 >3persisting risk factorsAES + LMWH for 7 days (C) BMI >40kg/mLMWH for 7 days (consensus) YES (C) Emergency section (category 1,2 or 3) LMWH for 7 days (C)YES (C) Elective caesarean section + 1 risk factor LMWH for 7 days (C)YES (C) asymptomatic heritable or acquired thrombophilia LMWH at 7 days – 6 weeks (C) YES (C) Women with previous VTELMWH until 6 weeks (C)YES (C) Women receiving LMWH antenatallyLMWH until 6 weeks (C)YES (C) In women who have additional persistent risk factors thromboprophylaxis LMWH up to 6 weeks (consensus)")
32
RCOG guidance: Green top guideline 37 (2009) Antenatal management: The major change
 Antenatal management: The major change")
33
Antenatal Thromboprophylaxis with LMWH should be considered if: ≥ 3 risk factors and managed as an outpatient ≥ 2 risk factors and managed as an inpatient a Score 1 for BMI > 30 kg/m2; 2 for BMI > 40 kg/m2 (BMI based on booking weight)
")
34
Risk scoring at time of delivery – added to pre-existing factors. ≥ 2 risk factors give LMWH for 7 days

35
Pregnancy/delivery factorAdjusted OR95% CI Previous VTE (all)24.817.6-36.0 SLE8.75.8-13 Obstetric haemorrhage9.01.1-71 Transfusion (all)7.66.2-9.4 Stillbirth in current pregnancyNot recorded Caesarean section during labour2.71.8-4.1 Caesarean section without labour2.01.5-2.7 Preterm live-birth (<37 weeks)2.41.6-3.5 Pregnancy hypertension2.92.1-3.9 Parity >32.41.8-3.1 Weight >120kg4.321.26-14.84 90-120kg1.931.1-3.39 RCOG – the stats behind the recommendations
 SLE Obstetric haemorrhage Transfusion (all) Stillbirth in current pregnancyNot recorded Caesarean section during labour Caesarean section without labour Preterm live-birth (<37 weeks) Pregnancy hypertension Parity > Weight >120kg kg RCOG – the stats behind the recommendations")
Similar presentations









 Prophylaxis Policy Mary-Anne Davies Patient Safety Specialist Accreditation Coordinator.>")

>")







 in obstetrics Dr. Yasir Katib MBBS, FRCSC, Perinatologist.>")