Download presentation
Presentation is loading. Please wait.

1
G OOD M ORNING ! Monday, August 6 th, 2012

2
N EONATES : F IRST S TOOL Healthy full term neonates: 60% stool in first 8 hours 91% by 16 hours 98.5% by 24 hours >99% by 48 hours Premature neonates: 95% stool by 48 hours

3
I LLNESS S CRIPT Predisposing Conditions Age, gender, preceding events (trauma, viral illness, etc), medication use, past medical history (diagnoses, surgeries, etc) Pathophysiological Insult What is physically happening in the body, organisms involved, etc. Clinical Manifestations Signs and symptoms Labs and imaging

5
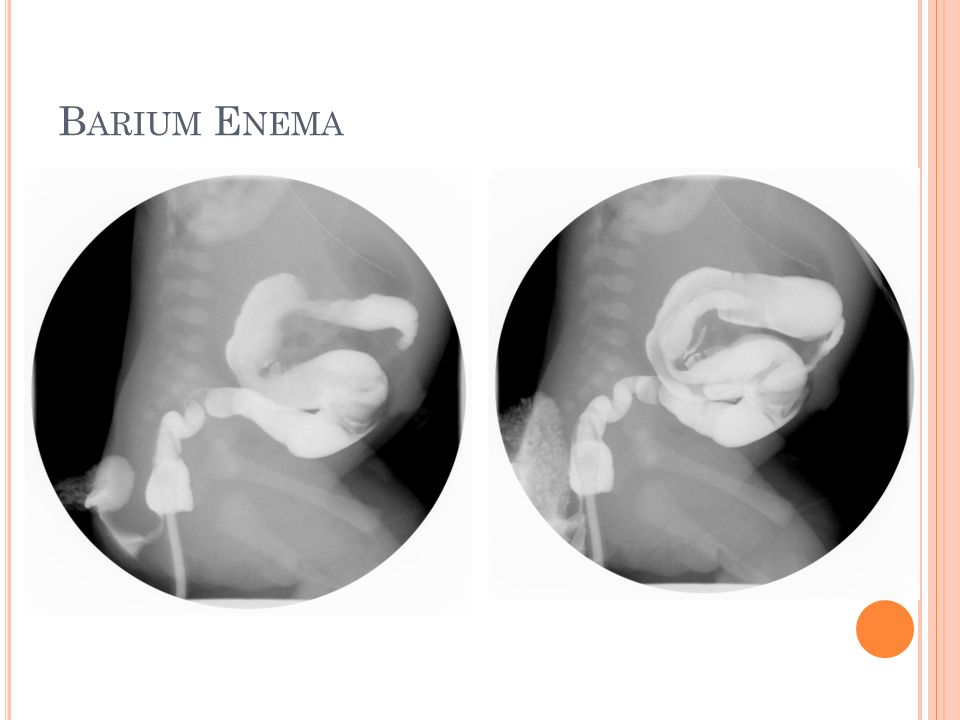
B ARIUM E NEMA

9
H IRSCHSPRUNG : P REDISPOSING C ONDITIONS Sporadic or familial (4 gene mutations identified) Male predominance (3.8:1) Slightly more common in African-American and Asian ethnicities 70% are isolated birth defect 30% associated with other disorders Trisomy 21 Waardenburg, Laurence-Moon-Biedl, Smith-Lemli- Opitz, MEN type IIa, congenital central hypoventilation syndrome (Haddad syndrome)
 Male predominance (3.8:1) Slightly more common in African-American and Asian ethnicities 70% are isolated birth defect 30% associated with other disorders Trisomy 21 Waardenburg, Laurence-Moon-Biedl, Smith-Lemli- Opitz, MEN type IIa, congenital central hypoventilation syndrome (Haddad syndrome)")
10
H IRSCHSPRUNG : P ATHOPHYSIOLOGY Congenital absence of ganglion cells in the myenteric and submucousal colonic plexuses Failure of migration of ganglion cell precursors to migrate from the neural crest to GI tract (5-12 WGA) Begins at the internal anal sphincter and extends proximally to a variable distance The earlier the arrest in migration occurs, the longer the segment involved Abnormal innervation disrupts the inhibitory paraympathetic nerves results in sustained contraction of the aganglionic segment Leads to colonic obstruction 80% are short segment (S-HSD) Distal to splenic flexure; often limited to rectosigmoid 20% are long segment (L-HSD) Rarely can affect entire colon and small intestine
 Begins at the internal anal sphincter and extends proximally to a variable distance The earlier the arrest in migration occurs, the longer the segment involved Abnormal innervation disrupts the inhibitory paraympathetic nerves results in sustained contraction of the aganglionic segment Leads to colonic obstruction 80% are short segment (S-HSD) Distal to splenic flexure; often limited to rectosigmoid 20% are long segment (L-HSD) Rarely can affect entire colon and small intestine")
11
H IRSCHSPRUNG : C LINICAL M ANIFESTATIONS ** Failure to pass meconium in first 24hrs of life** Abdominal distension Bilious emesis Diarrhea Feeding intolerance Short-segment HD: Presents later in childhood Intractable constipation Ribbon-like stools Abdominal distension FTT Rectal exam: increased tone, empty rectal vault, explosive release of stool

13
B ARIUM ENEMA Transition zone Narrow-diameter rectosigmoid colonic segment Dilated/hypertrophied proximal colon

14
H IRSCHSPRUNG : D IAGNOSIS Barium enema: suggestive; but absence of transition zone does not rule out HD Anorectal manometry Tests response to balloon inflation in the region of the internal and external sphincters Normally, balloon inflation/dilation of rectum induces relaxation of internal sphincter Absence of this relaxation indicates HD Rectal biopsy (Gold standard)** Suction rectal biopsy at 2 and 5cm from anal verge Looking for absence of ganglion cells Acetylcholinesterase staining shows hyperplastic axons due to absence of ganglion cells If inconclusive, may need full thickness biopsy
** Suction rectal biopsy at 2 and 5cm from anal verge Looking for absence of ganglion cells Acetylcholinesterase staining shows hyperplastic axons due to absence of ganglion cells If inconclusive, may need full thickness biopsy")
15
H IRSCHSPRUNG : C OMPLICATIONS ** Enterocolitis** Bacterial infection secondary to stasis/dilated colon Watery, explosive foul-smelling stools, +/- bleeding Abdominal distension Fever Hemodynamic instability 20% mortality Sepsis Bowel Perforation Stricture formation after surgery

16
T REATMENT Surgery Remove all or most of the aganglionic segment Reanastomose normal proximal bowel to the distal rectum or anal canal Goal: to establish regular defecation and maintain continence Most have a good outcome, however 30% remain constipated or never develop fecal continence

17
T HANK YOU !! Noon conference: NICU Radiology (Dr. Congeni)
")
Similar presentations










 Clase 10: Fisiología del colon Dr. Michel Baró A.>")












