Download presentation
Presentation is loading. Please wait.

1
Head, Neck, and Regional Lymphatics
Health assessment

2
Lectures objectives Identify the anatomic structures of the head and neck. Identify the lymph nodes of the head and neck. Describe the system-specific health history for the head and neck.

3
Lectures objectives Demonstrate the physical assessment of the head and neck. Describe normal findings in the physical assessment of the head and neck. List common abnormalities found in physical assessment of the head and neck. Explain pathophysiology of common abnormalities found in physical assessment of the head and neck.

4
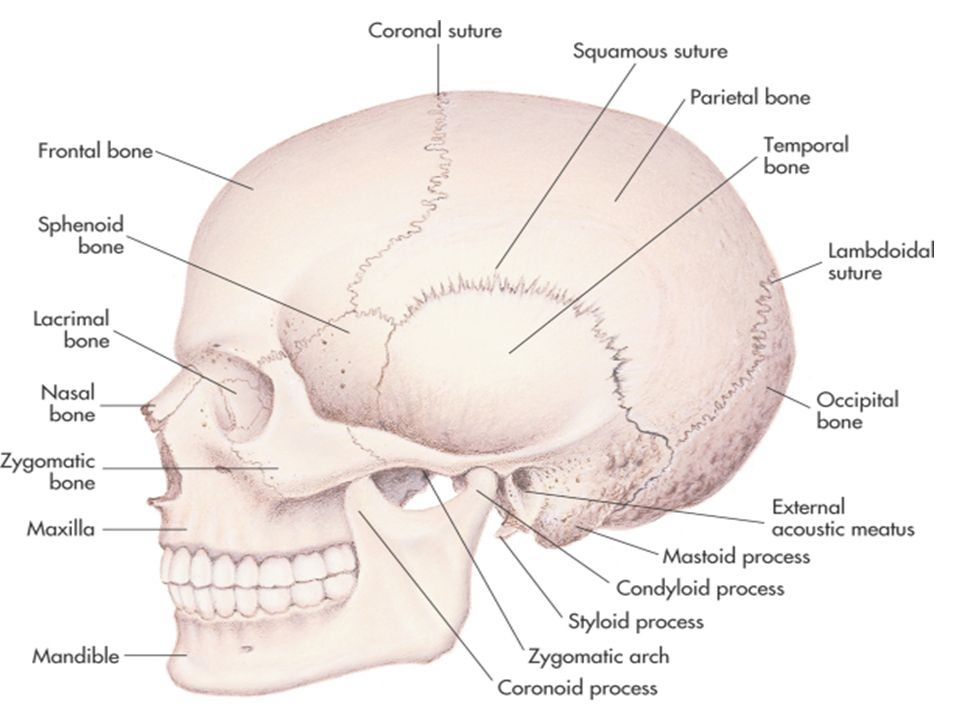
Landmarks of the face. Bones of the skull

6
Overview The integration of body systems and regions begins with the head and neck. The head provides a means of identifying individuals through the uniqueness of hair, eyes, and facial characteristics. With assessment of the head and neck, clues to the client’s nutritional status, airway clearance, tissue perfusion, metabolism, level of activity, sleep, rest, stress, and self-care abilities will be identified.

7
Anatomy and Physiology
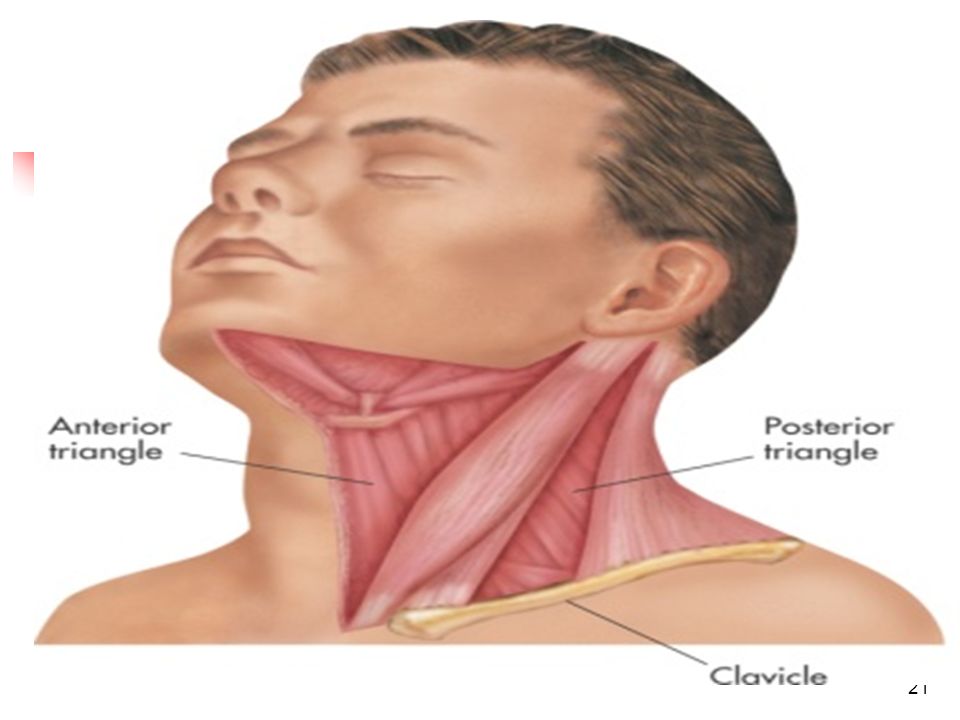
The skull is made up of the bones of the cranium and the face. The cranium includes frontal, parietal, temporal, and occipital bones. The muscles of the face play a role in expression of emotions and assist in neck movement. Movement of the facial muscles is controlled by cranial nerves V and VII. The carotid arteries provide the blood supply to the head; the temporal artery supplies blood to much of the face. The neck is supported and made mobile by vertebral processes and the sternocleidomastoid and trapezius muscles. The hyoid bone, superior to the larynx, is the only bone in the body that does not directly articulate with another bone. It serves as a movable base for the tongue, and an attachment for muscles of the neck. The thyroid gland is in the middle of the neck anterior to the trachea. The isthmus is the center, and the two lobes lie on either side of the trachea. The nine sets of lymph nodes drain the head and neck.

8
Health History Determine presence/absence of age- and gender-specific diseases of the head and neck Common chief complaints Neck pain or stiff neck Hoarseness Neck mass Headache Head injury

9
Evaluating Chief Complaint
Determine the following characteristics Quality Associated manifestations Aggravating factors Alleviating factors Setting Timing

10
Past Health History Medical conditions Surgeries Medications
Injuries or accidents

11
Family Health History Determine if family history of Thyroid disease
Headache

12
General Approach to Head and Neck Assessment
Greet patient, explain assessment techniques Environment Quiet Warm Private Adequate lighting Upright sitting position Compare right and left sides Systematic approach EQUIPMENT Tape measure ◆ Stethoscope ◆ Cup of water (for evaluation of thyroid gland)
")
13
Assessment of the Head Inspection Palpation Shape Symmetry Contour
Masses Depression Tenderness

14
Inspection and Palpation of the Scalp
Lesions or masses Normal findings Scalp is shiny, intact, without lesions or masses Abnormal findings Bleeding, lesions, masses, hematomas

15
Assessment of the Face Inspection Normal findings Shape Symmetry
Symmetrical features Palpebral fissures equal Shape can be oval, round, or slightly square

16
Assessment of the Face Abnormal findings Deformed or absent structures
Asymmetry More or less pronounced facial features Diseases which may alter facial features: Bell’s palsy, A temporary disorder affecting cranial nerve VII and producing a unilateral facial paralysis

17
acromegaly An enlargement of the skull and cranial bones due to increased growth hormone
hydrocephalus The enlargement of the head caused by inadequate drainage of cerebrospinal fluid, resulting in abnormal growth of the skull

18
Mandible Palpate and auscultate the temporo-mandibular joint when the client opens and closes the mouth Normal findings No discomfort, joint articulates smoothly without clicking or crepitus Abnormal findings Pain, tenderness, crepitus

19
Neck Inspection Palpation Normal findings Abnormal findings
Full ROM, pain free, symmetrical muscles, no masses Abnormal findings Limited ROM, pain, asymmetrical muscles, masses

22
Thyroid Gland Inspection Palpation Auscultation Normal findings
Symmetrical movement with swallowing Adam’s apple more pronounced in males No masses, tenderness, or enlargement Absent bruit Abnormal findings Mass Enlarged gland Goiter Asymmetrical enlargement Presence of a nodule or bruit

23
hyperthyroidism The excessive production of thyroid hormones, resulting in enlargement of the gland, exophthalmos (bulging eyes), fine hair, weight loss, diarrhea, and other alterations. hypothyroidism Metabolic disorder causing enlarged thyroid due to iodine deficiency.

24
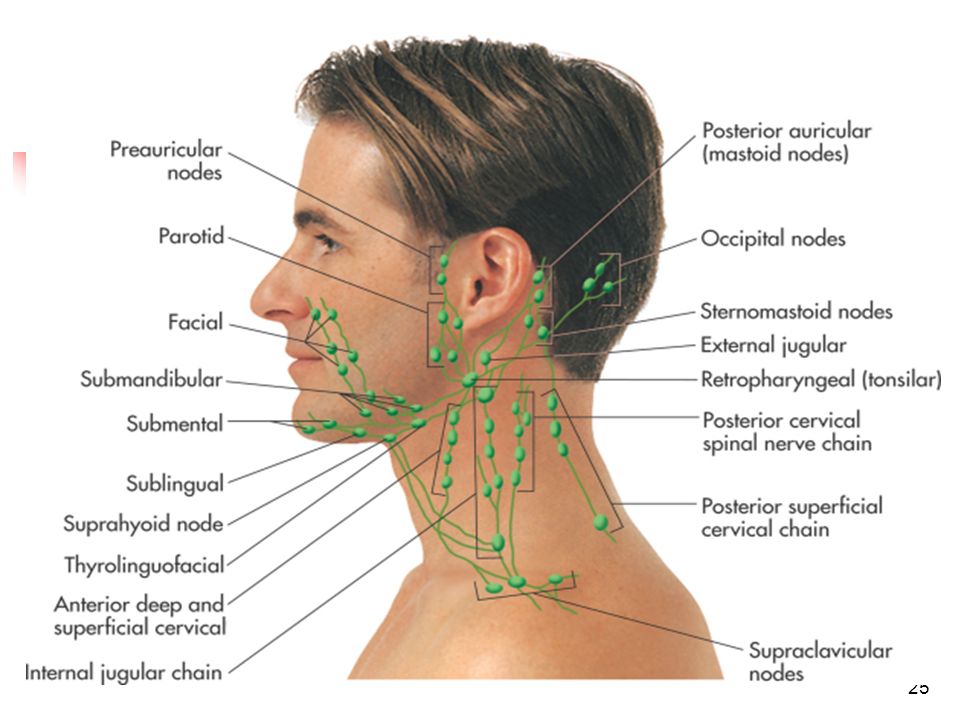
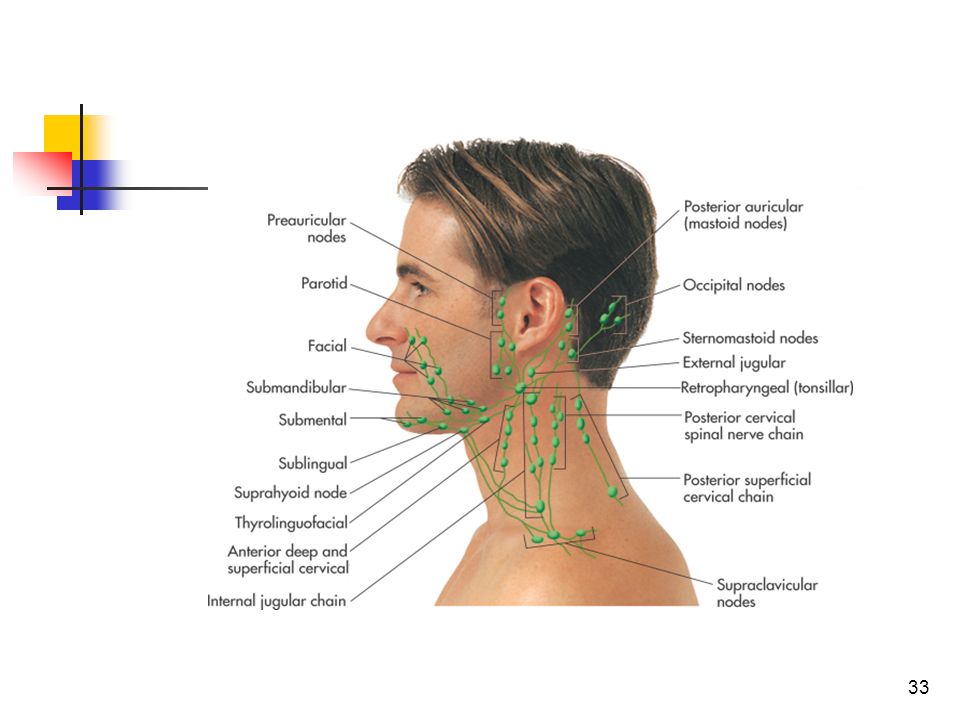
Lymph Nodes Location Inspection Palpation Preauricular Postauricular
Occipital Submental Submandibular Anterior and posterior cervical chains Tonsilar Supraclavicular

26
Lymph Nodes Normal findings Abnormal findings
Unable to palpate or see nodes Abnormal findings Enlarged nodes Able to palpate or see nodes Tenderness Firm, hard nodes

27
Position of the thumbs to evaluate the midline position of the trachea

28
Cushing syndrome. Facies include a rounded or “moon-shaped” face with thin, erythematous skin. Hirsutism may also be present, especially if the condition is caused by an adrenal cancer

29
Hyperthyroid facies. Note fine, moist skin with fine hair, prominent eyes and lid retraction, and staring or startled expression

30
Down syndrome. Note depressed nasal bridge, epicanthal folds, mongoloid slant of eyes, low-set ears, and large tongue

31
Hydrocephalus, with characteristic enlarged head, bulging fontanel, dilated scalp veins,

32
Early acromegaly. Note the coarsening of features with broadening of the nasal alae and prominence of the zygomatic arches

34
Left facial palsy. Facies include asymmetry of one side of the face, eyelid not closing completely, drooping lower eyelid and corner of mouth, and loss of nasolabial fold.

Similar presentations