Download presentation
Presentation is loading. Please wait.

1
Tips for analyzing CTO lesions: First step to success 哈尔滨医科大学附属第一医院 李为民 The First Affiliated Hospital Of Harbin Medical University

2
Long-term Outcomes After PCI for Chronic Total Occlusion Conclusion: Successful PCI of CTOs imparts no long-term survival advantage compared with failed attempts, but certain subgroups may benefit. 1,524 patients in the CREDO Kyoto PCI/CABG Registry Cohort 2 underwent CTO PCI between 2005 and 2007; 1,192 had successful procedures and 332 did not. Yamamoto E, et al. Am J Cardiol. 2013;Epub ahead of print. 3-Year Outcomes: Successful vs. Failed PCI Adjusted HR 95% CI P Value All-Cause Death0.930.64-1.370.69 Cardiac Death0.710.44-1.160.16 CABG0.090.06-0.15< 0.0001 Subgroup analyses found reductions in cardiac death with successful PCI in patients with single-vessel disease (P = 0.01), no history of heart failure (P = 0.004), and LAD lesions (P = 0.04) and in those without diabetes (P = 0.04).
, no history of heart failure (P = 0.004), and LAD lesions (P = 0.04) and in those without diabetes (P = 0.04)..")
3
Success Rate of CTO Morino Y, et al. JACC Cardiovasc Interv. 2011, 4:213-21 ------from J-CTO Registry Overall 1st try Re-try % GW SuccessLesion Success 87.7% 88.6% 86.6%72.2% 89.5% 68.5%

4
Morino Y, et al. JACC Cardiovasc Interv. 2011, 4:213-21 J-CTO SCORE SHEET (1) ≥20mm (1) (1)
 ≥20mm (1) (1)")
5
The Risk Groups of Difficulty and Final Procedural Success Rates J-CTO Score Morino Y, et al. JACC Cardiovasc Interv. 2011, 4:213-21

6
Histopathology of CTO

7
shorter-duration CTO fibrotic plaque calcified lesions. organized thrombus with microchannels Histopathology of CTO 200 μm

8
The longitudinal continuity of microchannels extended to approximately 85% of the entire CTO length, except in the early phase of CTO. J Am Coll Cardiol Img 2010;3:797– 805. Continuous loose tissue is frequently seen in the tapered entry type of CTO as well as in the short-occlusive-length CTO. J Am Coll Cardiol 1993;21:604–11. Histopathology of CTO

9
Understanding of CTO histopathology is important not only to improve success rate, but also to develop new techniques and strategies for CTO-PCI. Hydrophilic wires and low profile tips facilitate crossing.

10
MSCT for CTO Planning Novel imaging approaches for CTO

11
Potential Value of MSCT in CTO-PCI

12
Roles of IVUS in CTO-PCI Identifying true or false lumen Detecting the entry of CTO Landing of stent Retrograde apporach Understanding the complicated situation IVUS has been commonly used in CTO-PCI in Japan Takahiko Suzuki CIT 2011

13
IVUS Guided CTO-PCI Identification of true or false lumen

14
IVUS Guided CTO-PCI

15
Evaluation of Different Techniques

16
The routine PCI technique for CTO is still the antegrade approach If the antegrade approach is not successful and a collateral circulation is present, the retrograde approach can be attempted Combination of both antegrade and retrograde techniques can improve the success rate from 70% up to 90% Current Opinions EuroPCR 2011

17
Strategy for Current CTO-PCI Intervention

18
Wire Selection 2007 首选 Fielder XT 正向微孔道循径

19
Fielder Series Slippy and small tip slippy wire developed 0.8g 0.014

20
X-treme XT-R “Composite core” New Fielder XT with “Composite core” design Durable and Flexible 0.010” tip-Tip load=0.6gf High torque performance for retro/antegrade approach 1.0 X-treme XT-A

21
Gaia First Gaia Second Slip coat coating length 400mm Tip load

22
New CTO Devices ------ Micro Catheters

23
Corsair Micro-Catheter Tapered soft tip PTFE Inner Layer Hydrophilic Polymer coating 8 thin wires wound with 2 larger onesPushability, trackability and support

24
Balloon for CTO-PCI Sprinter Legend RX

25
Rotational atherectomy in CTO-PCI Catheter Cardiovasc Interv. 2010 Sep 1;76(3):366-71 The inability to cross a CTO with a balloon catheter occurs in approximately 7% of all CTOs that are successfully crossed with a guidewire. Rotational atherectomy is a safe and effective technique to overcome this frustrating situation.
: The inability to cross a CTO with a balloon catheter occurs in approximately 7% of all CTOs that are successfully crossed with a guidewire. Rotational atherectomy is a safe and effective technique to overcome this frustrating situation..")
26
Case 1 A 39-year-old male patient presented with effort chest pain for 3 months Without history of Hypertension and Diabetes ECG: ST depression in leads V 2-6 Echo: : LV diameter: 47mm, LVEF 60%

29
6F BL 3.0 Runthrough × Fielder XT √ Finecross ×

30
Pilot 50 × Pilot 150 √ Legend 1.25×6mm × Minitrack 1.2×8mm × Ryujin 1.25×15mm × Multi-wire plaque crushing

31
沿 Pilot 150 Ryujin 1.25×15mm 球囊挤撬

33
Case 2 A 72-year-old woman was admitted with effort chest pain for 6 months Hypertension (20y) ECG: ST depression in II, III, avF leads Echo: inferior wall dyskinesia; EF: 52%
 ECG: ST depression in II, III, avF leads Echo: inferior wall dyskinesia; EF: 52%")
36
6F JR 4.0 Runthrough × Fielder XT √ MiniTREK 1.2×6mm × Transradial

37
Transfemoral 6F AL 0.75 Pilot 50 √ MiniTREK 1.2×6mm ×

38
Seesaw balloon-wire cutting miniTREK 1.2×6 mm Sprinter 1.25×6mm

40
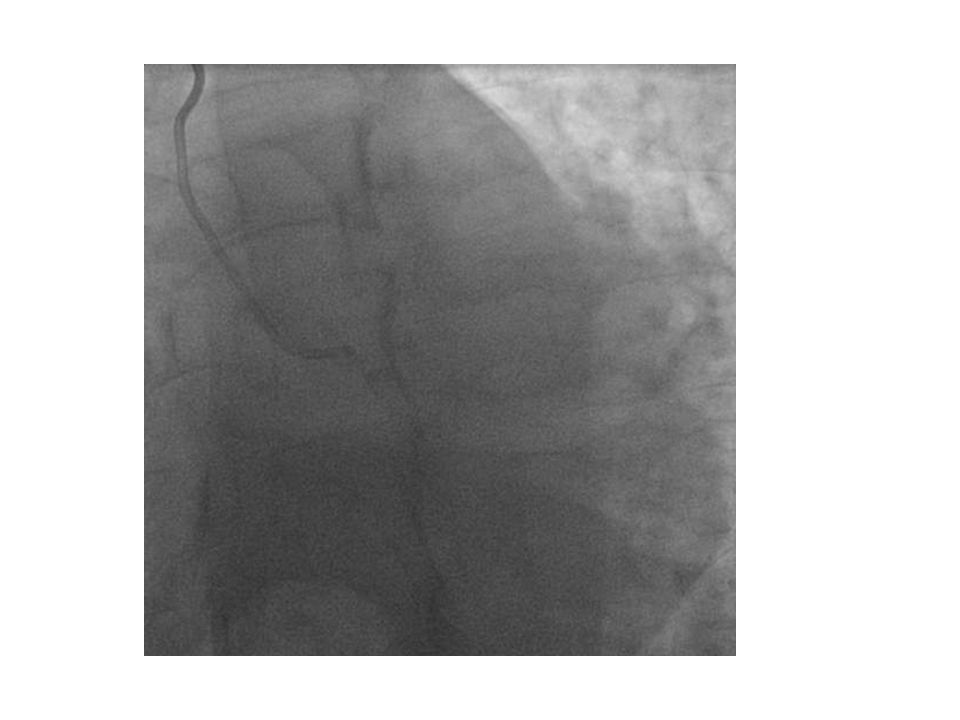
Case 3 A 62-year-old man Chest discomfort on exertion for 5 months Hypertension (10y) and DM type II (10y) ECG: ST-T changes in V2-V6 leads Echo: anterior wall dyskinesia,LV diameter: 55mm, LVEF 48%
 and DM type II (10y) ECG: ST-T changes in V2-V6 leads Echo: anterior wall dyskinesia,LV diameter: 55mm, LVEF 48%")
43
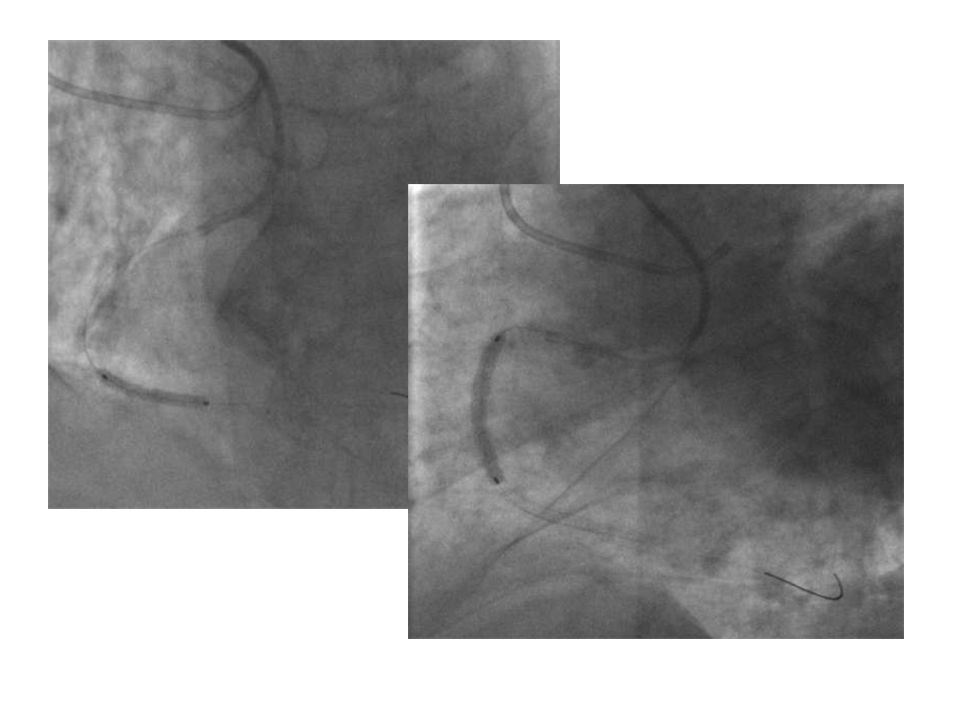
6F BL 3.0 Pilot 50 × Fielder XT √ Finecross ×

44
Pilot 150 × ? Seesaw balloon- wire cutting ×

45
Tornus

47
Case 4 A 56-year-old man Chest pain on exertion for 2 years Hypertension (10y) and hyperlipidemia (5y) ECG: ST-T changes in V1-V4 leads Echo: LV diastolic dysfunction CTA: pro-LAD CTO
 and hyperlipidemia (5y) ECG: ST-T changes in V1-V4 leads Echo: LV diastolic dysfunction CTA: pro-LAD CTO")
48
CTO in the proximal of LAD

50
6F BL 3.0 Finecross Fielder XT × Transradial

51
Conquest pro ×

52
Finecross JR4.0 SH

53
Finecross JR4.0 SH Sion Knuckle

54
Conquest pro

55
正向 Finecross Tip injection

57
A 72-year-old woman Paroxysmal chest pain for 3 days, Hypertension (15y) and DM type II (5y) ECG: ST-T changes in V 4 -V 6 leads Echo: Inferior wall dyskinesia,LV diameter: 54mm, LVEF 42% Case 5
 and DM type II (5y) ECG: ST-T changes in V 4 -V 6 leads Echo: Inferior wall dyskinesia,LV diameter: 54mm, LVEF 42% Case 5")
61
Finecross XB RCA Fielder XT

62
Finecross × legend 1.25×6mm ×

63
Pilot 150 ×

64
Corsair

65
Tip injection

66
Runthrough

69
Histopathology research reported that that loose tissue and microchannels ( average size of 200μm ) are frequently seen in CTO Microchannel tracking should be performed with a 0.8g-1.0g tip- strength hydrocoated wire with taper tip. (Fielder XT, 0.8g, 230μm) AS the weak support of Fielder XT , the subsequent balloon passage through the occlusion is still difficult,however,multi-wire plaque crushing 、 Seesaw balloon-wire cutting technique and Tornus are effective approachs for facilitating balloon passage through CTOs Take home message
 AS the weak support of Fielder XT , the subsequent balloon passage through the occlusion is still difficult,however,multi-wire plaque crushing 、 Seesaw balloon-wire cutting technique and Tornus are effective approachs for facilitating balloon passage through CTOs Take home message.")
70
Summary Analysis of CAG combined with MSCT is key step to achieve success. Contralateral CAG shoud be performed when necessary Choice of devices depends on analysis of CAG and Understanding of CTO histopathology. antegrade approach is still the routine technique for PCI of CTOs Combination of both antegrade and retrograde techniques can improve the success rate

71
马克思主义活的灵魂就是 具体问题具体分析 毛泽东《矛盾论》

72
哈医大一院心内科 Thank you for your patience Learn from yesterday, live for today, hope for tomorrow. The important thing is not to stop questioning. ------ Albert Einstein

Similar presentations















, FSCAI>")

















