Download presentation
Presentation is loading. Please wait.

1
Pregnancy & Hormonal Disorders

2
Thyroid Disorders & Pregnancy Normal thyroid phsyiology & pregnancy Hypothyroidism & pregnancy Thyrotoxicosis & pregnancy Postpartum thyroid dysfunction Diabetes & Pregnancy Gestational DM Type 1 & Type 2 DM & Pregnancy

4
TSH Low High FT4 FT4 & FT3 Low 1° Hypothyroid Low Central Hypothyroid TRH Stim. If equivocal MRI, etc. High 1° Thyrotoxicosis High 2° thyrotoxicosis Endo consult FT3, rT3 MRI, α-SU RAIU

5
Thyroid & Pregnancy: Normal Physiology Increased estrogen increased TBG (peaks wk 15-20) Higher total T4 & T3: normal FT4 & FT3 if normal thyroid fn. and good assay many automated FT4 assays underestimate true FT4 level if suspect your local FT4 assay is underestimating FT4 can check total T4 & T3 instead (normal pregnant range ~ 1.5x nonpregnant) hCG peak end of 1 st trimester, hCG has weak TSH agonist effect so may cause: slight goitre mild TSH suppression (0.1-0.4 mU/L) in 9% of preg mild FT4 rise in 14% of preg
 hCG peak end of 1 st trimester, hCG has weak TSH agonist effect so may cause: slight goitre mild TSH suppression ( mU/L) in 9% of preg mild FT4 rise in 14% of preg.")
6
Thyroid & Pregnancy: Normal Physiology Fetal thyroid starts working at 12-14 wks T4 & T3 cross placenta but do so minimally Cross placenta well: MTZ > PTU TSH-R Ab (stim or block) ATD (PTU & MTZ): Fetal goitre (can compress trachea after birth) MTZ aplasia cutis scalp defects Other MTZ reported embryopathy: choanal atresia, esophageal atresia, tracheo-esophageal fistula Therefore do NOT use MTZ during pregnancy, use PTU instead
 ATD (PTU & MTZ): Fetal goitre (can compress trachea after birth) MTZ aplasia cutis scalp defects Other MTZ reported embryopathy: choanal atresia, esophageal atresia, tracheo-esophageal fistula Therefore do NOT use MTZ during pregnancy, use PTU instead")
8
No TSH & FTI at end of 1 st trimester as expected from hCG effect Requirement to increase LT4 dose occurred between weeks 4 -20 Despite exponential rise in estradiol throughout pregnancy (note y-axis units) TBG levels plateau at 20 wks
 TBG levels plateau at 20 wks")
9
* Regardless of cause of hypothyroidism (Hashimoto’s, thyroidectomy) initial LT4 dose increase is usually required early (~ week 8), before 1 st prenatal visit!
 initial LT4 dose increase is usually required early (~ week 8), before 1 st prenatal visit!")
10
Thyroid & Pregnancy: Hypothyroidism 85% will need increase in LT4 dose during pregnancy due to increased TBG levels (ave dose increase 48%) Risks: increased spont abort, HTN/preeclampsia, abruption, anemia, postpartum hemorrhage, preterm labour, baby SGA Fetal neuropsychological development (NEJM, 341(8):549-555, Aug 31, 2001): Cognitive testing of children age 7-9 Untreated hyothyroid mothers vs. normal mothers: Average of 7 IQ points less in children Increased risk of IQ < 85 (19% vs. 5%) Retrospective study, data-dredging?
 Retrospective study, data-dredging .")
11
LT4 dose adjustment in Pregnancy: - Optimize TSH preconception (0.4 – 2.5 mU/L) - TSH at pregnancy diagnosis (~3-4 wk gestation), q1mos during 1 st 20 wks and after any LT4 dose change, q2mos 20 wks to term - Instruct women to take 2 extra thyroid pills/wk (q Mon, Thurs) for 29% dose increase once pregnancy suspected (+ commercial preg test) - If starting LT4 during preg: initial dose 2 ug/kg/d and recheck TSH q4wk until euthythyroid TSHDose Adjustment TSH increased but < 10 Increase dose by 50 ug/d TSH 10-20 Increase dose by 50-75 ug/d TSH > 20 Increase dose by 100 ug/d
 - TSH at pregnancy diagnosis (~3-4 wk gestation), q1mos during 1 st 20 wks and after any LT4 dose change, q2mos 20 wks to term - Instruct women to take 2 extra thyroid pills/wk (q Mon, Thurs) for 29% dose increase once pregnancy suspected (+ commercial preg test) - If starting LT4 during preg: initial dose 2 ug/kg/d and recheck TSH q4wk until euthythyroid TSHDose Adjustment TSH increased but < 10 Increase dose by 50 ug/d TSH Increase dose by ug/d TSH > 20 Increase dose by 100 ug/d")
12
Pregnancy: screen for thyroid dysfn ? Universal screening not currently recommended: ACOG, AACE, Endo Society, ATA Controversial! Definitely screen: Goitre, FHx thyroid dysfn., prior postpartum thyroiditis, T1DM Ideally, check TSH preconception: 2.5-5.0 mU/L: recheck TSH during 1 st trimester 0.4-2.5 mU/L: do not need to recheck during preg If TSH not done preconception do at earliest prenatal visit: 0.1-0.4 mU/L: hCG effect (9% preg), recheck in 5wk < 0.1 mU/L: recheck immediately with FT4, FT3, T4, T3
, recheck in 5wk < 0.1 mU/L: recheck immediately with FT4, FT3, T4, T3.")
13
Thyrotoxicosis & Pregnancy Causes: Graves’ disease TMNG, toxic adenoma Thyroiditis Hydatiform mole Gestational hCG-asscociated Thyrotoxicosis Hyperemesis gravidarum hCG 60% TSH, 50% FT4 Resolves by 20 wks gestation Only Rx with ATD if persists > 20 wk

14
Thyrotoxicosis & Pregnancy Risks: Maternal: stillbirth, preterm labor, preeclampsia, CHF, thyroid storm during labor Fetal: SGA, possibly congenital malformation (if 1 st trimester thyrotoxicosis), fetal tachycardia, hydrops fetalis, neonatal thyrotoxicosis
, fetal tachycardia, hydrops fetalis, neonatal thyrotoxicosis")
15
Thyrotoxicosis & Pregnancy Diagnosis difficult: hCG effect: Suppressed TSH (9%) +/- FT4 (14%) until 12 wks Enhanced if hyperemesis gravidarum: 50-60% with abnormal TSH & FT4, duration to 20 wks FT4 assays reading falsely low T4 elevated due to TBG (1.5x normal) NO RADIOIODINE Measure: TSH, FT4, FT3, T4, T3, thyroid antibodies? Examine: goitre? orbitopathy? pretibial myxedema?

16
Pregnant & Suppressed TSH TSH < 0.1TSH 0.1 – 0.4 Recheck in 5 wks FT4, FT3, T4, T3 Thyroid Ab’s Examine NormalizesStill suppressed Very High TFT’s: TSH undetectable very high free/total T4/T3 hyperthyroid symptoms no hyperemesis TSH-R ab + orbitopathy goitre, nodule/TMNG pretibial myxedema Treat Hyperthyroidism (PTU) Hyperemesis Gravidarum Abnormal TFT’s past 20 wk Don’t treat with PTU
 Hyperemesis Gravidarum Abnormal TFT’s past 20 wk Don’t treat with PTU")
17
Thyrotoxicosis & Pregnancy: Rx No RAI ever (destroy fetal thyroid) PTU Start 100 mg tid, titrate to lowest possible dose Monitor qmos on Rx: T4, T3, FT4, FT3 TSH less useful (lags, hCG suppression) Aim for high-normal to slightly elevated hormone levels T4 150-230 nM, T3 3.8-4.6 nM, FT4 26-32 pM 3 rd trimester: titrate PTU down & d/c prior to delivery if TFT’s permit to minimize risk of fetal goitre Consider fetal U/S wk 28-30 to R/O fetal goitre If allergy/neutropenia on PTU: 2 nd trimester thyroidectomy
 PTU Start 100 mg tid, titrate to lowest possible dose Monitor qmos on Rx: T4, T3, FT4, FT3 TSH less useful (lags, hCG suppression) Aim for high-normal to slightly elevated hormone levels T nM, T nM, FT pM 3 rd trimester: titrate PTU down & d/c prior to delivery if TFT’s permit to minimize risk of fetal goitre Consider fetal U/S wk to R/O fetal goitre If allergy/neutropenia on PTU: 2 nd trimester thyroidectomy")
18
Thyrotoxicosis & Lactation ATD generally don’t get into breast milk unless at higher doses: PTU > 450-600 mg/d MTZ > 20 mg/d Generally safe PTU > MTZ for preg lactating Take ATD dose just after breast-feeding Should provide 3-4h interval before lactates again

19
Neonatal Grave’s Rare, 1% infants born to Graves’ moms 2 types: Transplacental trnsfr of TSH-R ab (IgG) Present at birth, self-limited Rx PTU, Lugol’s, propanolol, prednisone Prevention: TSI in mom 2 nd trimester, if 5X normal then Rx mom with PTU (crosses placenta to protect fetus) even if mom is euthyroid (can give mom LT4 which won’t cross placenta) Child develops own TSH-R ab Strong family hx of Grave’s Present @ 3-6 mos 20% mortality, persistant brain dysfunction
 Present at birth, self-limited Rx PTU, Lugol’s, propanolol, prednisone Prevention: TSI in mom 2 nd trimester, if 5X normal then Rx mom with PTU (crosses placenta to protect fetus) even if mom is euthyroid (can give mom LT4 which won’t cross placenta) Child develops own TSH-R ab Strong family hx of Grave’s 3-6 mos 20% mortality, persistant brain dysfunction")
20
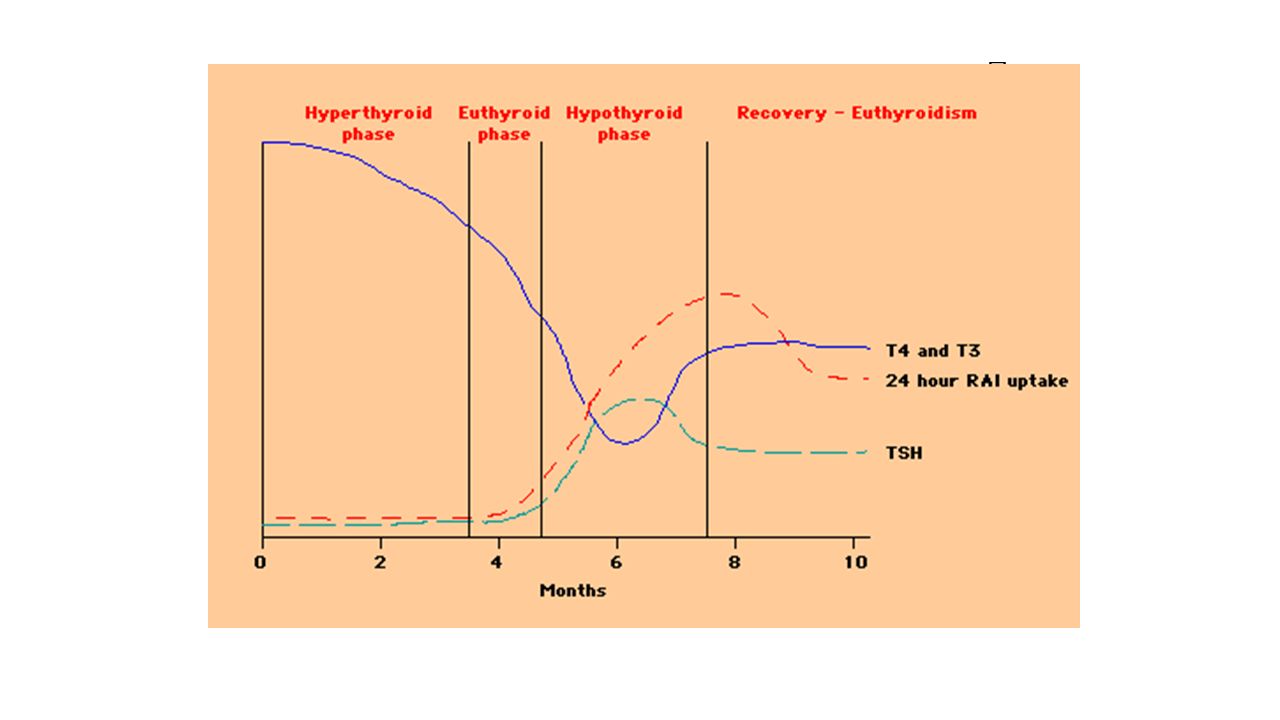
Postpartum & Thyroid 5% (3-16%) postpartum women (25% T1DM) Up to 1 year postpartum (most 1-4 months) Lymphocytic infiltration (Hashimoto’s) Postpartum Exacerbation of all autoimmune dx 25-50% persistant hypothyroidism Small, diffuse, nontender goitre Transiently thyrotoxic Hypothyroid
 postpartum women (25% T1DM) Up to 1 year postpartum (most 1-4 months) Lymphocytic infiltration (Hashimoto’s) Postpartum Exacerbation of all autoimmune dx 25-50% persistant hypothyroidism Small, diffuse, nontender goitre Transiently thyrotoxic Hypothyroid")
22
Postpartum & Thyroid Distinguish Thyrotoxic phase from Grave’s: No Eye disease, pretibial myxedema Less severe thyrotoxic, transient (repeat thyroid fn 2-3 mos) RAI (if not breast-feeding) Rx: Hyperthyroid symptoms: atenolol 25-50 mg od Hypothyroid symptoms:LT4 50-100 ug/d to start Adjust LT4 dose for symtoms and normalization TSH Consider withdrawal at 6-9 months (25-50% persistent hypothyroid, hi-risk recur future preg)
 RAI (if not breast-feeding) Rx: Hyperthyroid symptoms: atenolol mg od Hypothyroid symptoms:LT ug/d to start Adjust LT4 dose for symtoms and normalization TSH Consider withdrawal at 6-9 months (25-50% persistent hypothyroid, hi-risk recur future preg)")
23
Postpartum & Thyroid Postpartum depression When studied, no association between postpartum depression/thyroiditis Overlapping symtoms, R/O thyroid before start antidepressents Screening for Postpartum Thyroiditis HOW: TSH q3mos from 1 mos to 1 year postpartum? WHO: Symptoms of thyroid dysfn. Goitre T1DM Postpartum thyroiditis with prior pregnancy

Similar presentations











 2.Free T4 (normal range 0.7- 2.1 ng/dL) 3.Free T3 (normal range 1.4 - 4.4 pg/dL)>")









