Download presentation
Presentation is loading. Please wait.

1
Approach to the comatose patient Stephen Lo

2
Introduction Focus on developing a structured approach to coma Can be also applied to exam questions

3
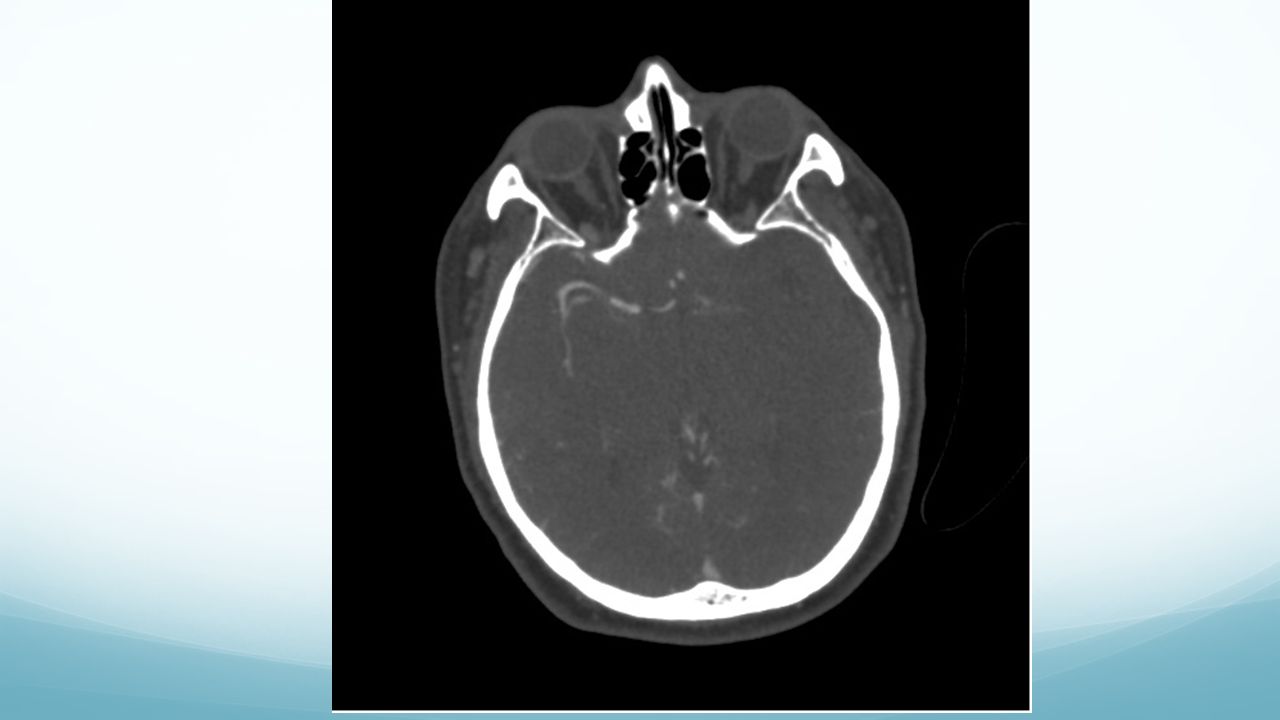
Case 50 year old polynesian lady presented with headache followed by LOC How would you assess and manage this patient?

4
Investigations

5
My approach Initial management Differential diagnosis Investigations Management

6
Initial steps: safety + ensure adequate resources Ask for resources ABC, basic resuscitation

7
Assessment of airway, breathing, and circulation Airway patency Airway protection: What is the GCS Is there protective reflexes present What is the risk of aspiration Are there secretions Rate and pattern of ventilation Circulation: signs of shock, hypotension. Consider maintaining CPP. In this case, I would put Blood sugar levels at the priority of the ABCs

8
Differential diagnosis Need to construct a list of differential diagnosis at this point.

9
Approach to the diagnosis Need a simple way of classifying causes Intracranial Extracranial

10
Intracranial Consider surgical sieve or other pneumonics Need to include the key ones such as: bleed, stroke, infection, trauma, Seizures, rarer causes such as tumours, autoimmune, vasculitis, PRES context specific differentials such as vasospasm, hydocephalus in SAH

11
Extracranial These are generally metabolic in nature. Again, have a sieve that you are familiar with, but need to include the most common ones including: Drugs: direct effect, indirect effects Acid base Hypoxia/hypercarbic Temperature Organ function: Kidney and liver Nutritional Electrolyte disturbance Endocrine Sepsis

12
Mimics of coma Severe peripheral neuropathy Guillain Barre syndrome Botulism Critical illness neuropathy Locked in syndrome Akinetic mutism

13
Assessment History and examination to rule out or in your differentials Catagorize into three broad categories based on patient’s signs Coma with focal signs: Suggests an intracranial event Coma with meningism: Suggests meningitis, SAH Coma without signs: Suggests a very diffuse intracranial lesion or an extracranial cause

14
Investigations Consider all your options Systemic investigations CT head Lumbar puncture: MCS, PCR, antibodies CT angiogram EEG MRI SSEPs Cerebral angiogram

15
What’s your management now? Medical management Specific management Position of patient, CO2 control, BP control, Osmotherapy, sedation, sugar, seizure control, temperature General management Interventions Radiological interventions Surgical management

16
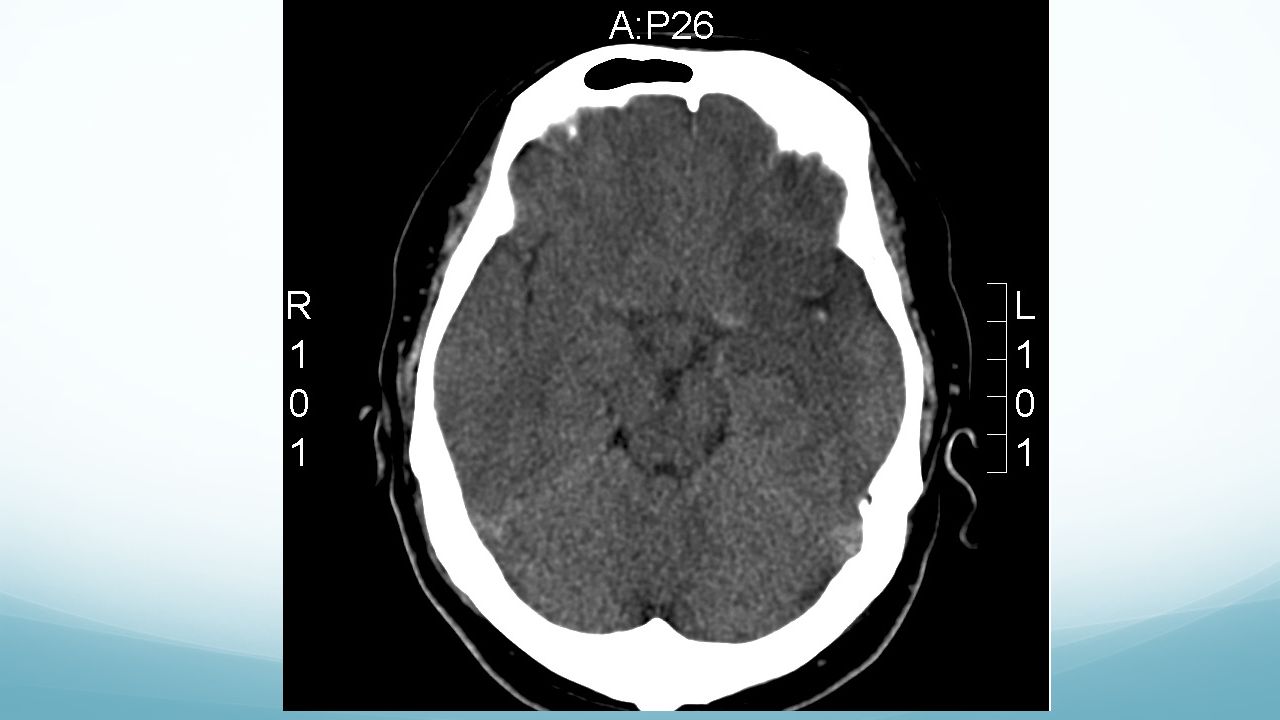
Case 2 49 yo male thai chef that was found collapsed at home, brought in by ambulance. How would you manage this patient?

17
Assessment ABC: Noisy breathing GCS: E1V2M5 Sats: 84 % on 6L BP 190/80, HR 90/min

18
Further clinical assessment Right side movement less than left Pupils equal and reactive

19
Investigations

23
Finding underlying causes Thromboembolic Consider source of clot Bleeding Is there an underlying abnormality Infection Are there underlying structural abnormality or immunosuppression Epilepsy Adult onset always need to consider cause

24
Further investigations ASD on echo Paradoxical embolus and therefore infarct

25
Other learning points That an extensive unilateral lesion can also cause reduced LOC

Similar presentations








 of the lining surrounding the brain & spinal cord (meninges) Life-threatening condition ~135,000.>")











