Download presentation
Presentation is loading. Please wait.

1
HETEROPHORIAANDVERGENCEABNORMALITIES

2
Heterophoria Heterophoria may present clinically with associated visual symptoms, particularly at times of stress or poor health, when the fusional amplitudes are insufficient to maintain alignment. Both esophoria and exophoria can be classified by the distance at which the angle is greater ( respectively : convergence excess or weakness,divergence weakness or excess, and mixed ) ; vertical phoria are caused by abnormal ocular motility. Treatment involves the following :
 ; vertical phoria are caused by abnormal ocular motility. Treatment involves the following :.")
3
- Orthoptic treatment is of most value in convergence weakness exophoria. - Any significant refractive error should be appropriately corrected. - Symptom relief may otherwise be obtained using temporary stick-on Fresnel prisms and may be subsequently incorporated into spectacles ( maximum usually 10-12 ∆ split between the two eyes ). - Surgery may occasionally be required for larger deviations.
. - Surgery may occasionally be required for larger deviations..")
4
VERGENCE ABNORMALITIES Convergence insufficiency Convergence insufficiency typically affects individuals with excessive visual demand such as students. 1- signs : reduced near point of convergence independent of any heterophoria. 2- treatment : involves orthoptic exercises aimed at normalizing the near point and fusional amplitudes. With good compliance, symptoms should be eliminated within a few weeks but if persistent can be treated with base-in prisms.

5
3- accommodative insufficiency : is occasionally also present. It may be idiopathic ( primary ) or post-viral and typically affects school age children. The minimum reading correction is prescribed to give clear vision but is often difficult to discard. Near reflex insufficiency 1- paresis of the near reflex presents as an exaggerated of convergence and accommodation insufficiency. Mydriasis may be seen on attempted near fixation. In the absence of neurological signs treatment involves reading glasses, base-in prisms and possibly Botulinum toxin ( orthoptic exercises have no effect ) but it is difficult to eradicate.
 or post-viral and typically affects school age children. The minimum reading correction is prescribed to give clear vision but is often difficult to discard. Near reflex insufficiency 1- paresis of the near reflex presents as an exaggerated of convergence and accommodation insufficiency. Mydriasis may be seen on attempted near fixation. In the absence of neurological signs treatment involves reading glasses, base-in prisms and possibly Botulinum toxin ( orthoptic exercises have no effect ) but it is difficult to eradicate..")
6
2- complete paralysis in which no convergence or accommodation can be initiated may be of functional origin or caused by midbrain disease or follow head trauma ( recovery possible ). Near reflex spasm Spasm of the near reflex is a functional condition affecting patients of all ages ( mainly females ). 1- signs : - Diplopia, blurred vision and headaches are accompanied by esotropia, pseudomyopia and miosis. - The spasm may be triggered when testing ocular movements. - Observing miosis is the key to the diagnosis. - Refraction with and without cycloplegia confirms the pseudomyopia, which must not be corrected optically.
. 1- signs : - Diplopia, blurred vision and headaches are accompanied by esotropia, pseudomyopia and miosis. - The spasm may be triggered when testing ocular movements. - Observing miosis is the key to the diagnosis. - Refraction with and without cycloplegia confirms the pseudomyopia, which must not be corrected optically..")
7
2- treatment involves reassurance and advising the patient to look away and cease the activity that triggers the response. If persistent, atropine and a full reading correction are prescribed but it is difficult later to abandon treatment without recurrence. Patients usually seem to live a fairly normal life despite the signs and symptoms.

8
Divergence insufficiency Divergence paresis or paralysis is a rare condition associated with underlying neurological disease, such as intracranial space-occupying lesions, CVA and head trauma. Presentation may be at any age and may be difficult to differentiate from sixth nerve palsy, but is primarily a concomitant esodeviation with reduced or abscent divergence fusional amplitudes. It is difficult to treat ; prisms are the best option.

9
ESOTROPIA

10
Esotropia ( manifest convergent deviation ) may be concomitant or incomitant. In a concomitant esotropia the variability of the angle of deviation is within 5 ∆ in different horizontal gaze positions. In an incomitant deviation the angle differs in various positions of gaze as a result of abnormal innervation or restriction. All squints are different and not all fit neatly into a classification. For example a microtropia may occur with a number of the other categories.

11
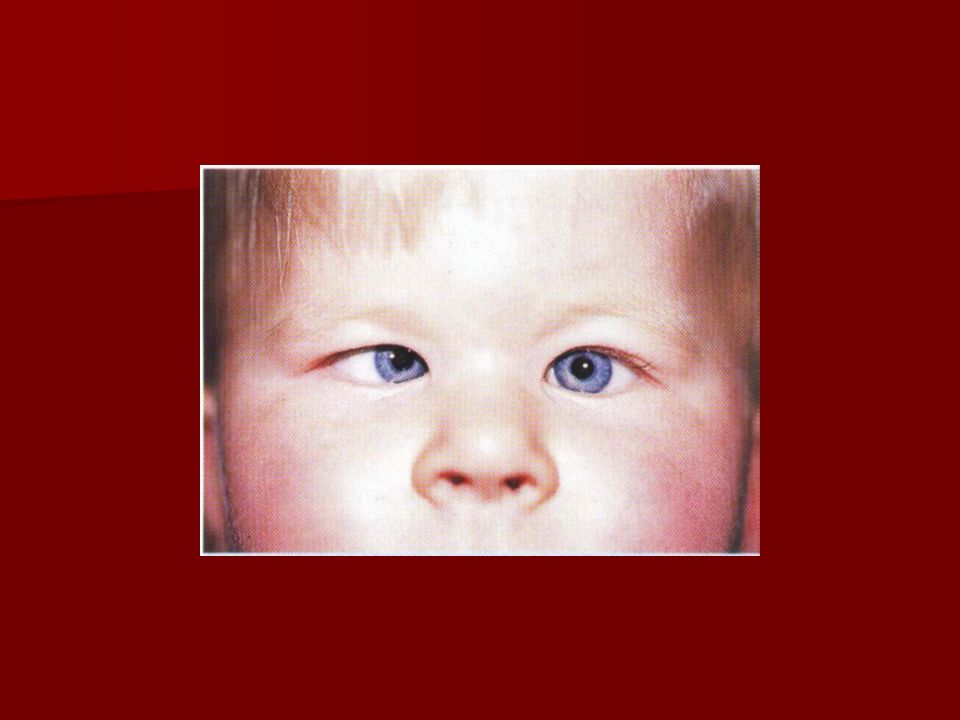
It is more important to understand the part played by binocular function, refractive error and accommodation in the pathophysiology of each individual squint and to tailor treatment accordingly. EARLY ONSET ESOTROPIA Up to 4 months of age infrequent episodes of convergence are normal. After 4 months ocular misalignment is abnormal. Early onset ( congenital, essential, infantile ) esotropia is an idiopathic condition developing within the first 6 months of life in an otherwise normal ifant with no significant refractive error and no limitation of ocular movements.
 esotropia is an idiopathic condition developing within the first 6 months of life in an otherwise normal ifant with no significant refractive error and no limitation of ocular movements..")
12
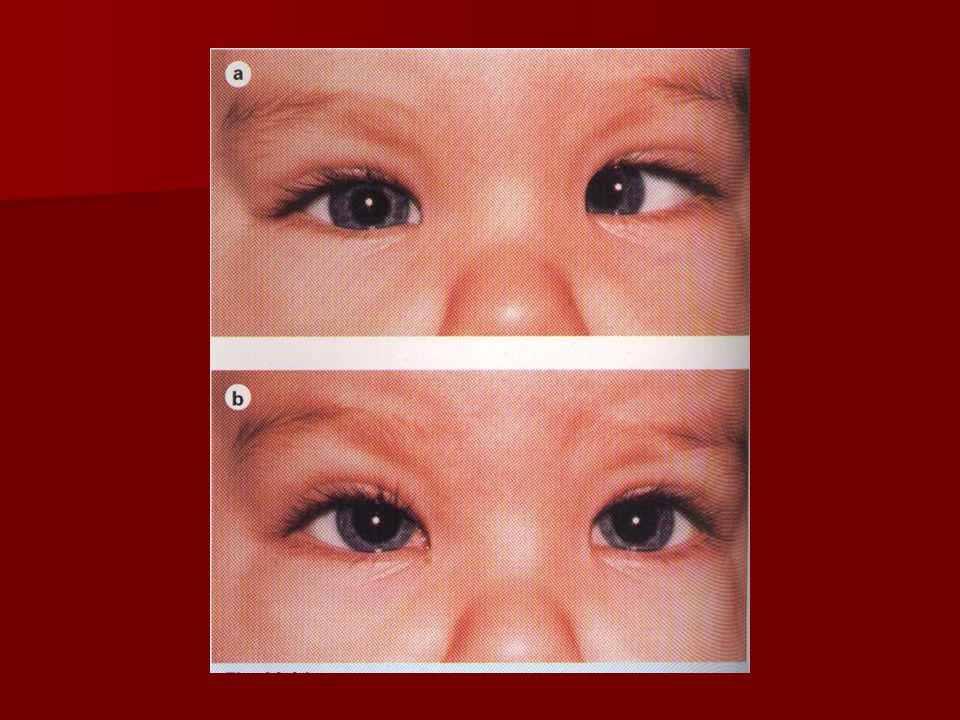
Diagnosis - The angle is usually fairly large ( > 30 ∆ ) and stable. - Fixation in most infants is alternating in the primary position. - There is cross-fixation in side gaze, so that the child uses the left eye in right gaze and the right eye in left gaze. Such cross fixation may give a false impression of bilateral abduction deficits, as in bilateral sixth nerve palsy. - Abduction can, however, usually be demonstrated either by the doll’s head manoeuvre or by rotating the child.

13
- Should these fail, uniocular patching for a few hours will often unmask the ability of the other eye to abduct. - Nystagmus is usually horizontal. - Latent nystagmus is only seen when one eye is covered and the fast phase beats towards the side of the fixing eye. This means that the direction of the fast phase reverses according to which eye is covered. - Manifest latent nystagmus is the same except that nystagmus is present with both eyes open, but the amplitude increases when one is covered.

14
- The refractive error is usually normal for the age of the child ( about + 1 to +2D ). - Asymmetry of optokinetic nystagmus. - Inferior oblique overaction may be present initially or develop later. - Dissociated vertical deviation ( DVD ) develops in 80 % by the age of 3 years.
 develops in 80 % by the age of 3 years..")
17
INITIAL TREATMENT Early ocular alignment gives the best chance of the child developing some form of binocular function. Ideally, the eyes should be surgically aligned by the age of 12 months, and at the very latest by the age of 2 years, but only amblyopia or significant refractive errors have been corrected. The initial procedure can be either recession of both medial recti or unilateral medial rectus recession with lateral rectus resection. Very large angles may require recessions of 6.5 mm or more.

18
Associated inferior oblique overaction should also be addressed. An acceptable goal is alignment of the eyes to within 10 ∆ associated with peripheral fusion and central suppression. This small-angle residual strabismus is often stable, even though bifoveal fusion is not achieved.

20
SUBSEQUENT TREATMENT 1-undercorrection may require further recession of the medial recti, resection of one or both lateral recti or surgery to the other eye. 2- inferior oblique overaction may develop subsequently, most commonly at age 2 years. The parents should therefore be warned that further surgery may be necessary despite an initially good result. Initially unilateral, it frequently becomes bilateral within 6 months. Inferior oblique weakening procedures include disinsertion, recession and myectomy.

22
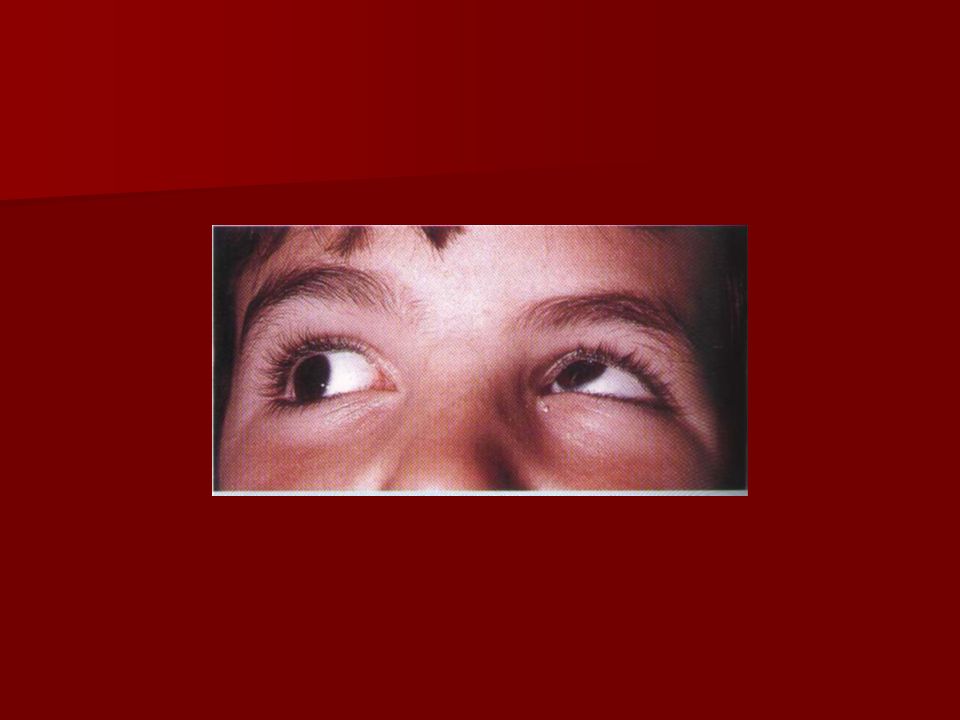
3- DVD may appear several years after the initial surgery, particularly in children with nystagmus. It is characterized by the following : - up-drift with excyclotorsion of the eye when under cover or spontaneously during periods of visual inattention. - When the cover is removed the affected eye will move down without a corresponding down-drift of the other eye. Thus DVD does not obey Hering law. Although it is usually bilateral, it may be asymmetrical. Surgical treatment is indicated when the condition is cosmetically unacceptable. Superior rectus recession with or without posterior fixation sutures or inferior oblique anterior transposition are useful for DVD, although full

23
elimination is seldom possible.

24
4- amblyopia subsequently develops in about 50% of cases as unilateral fixation preference commonly develops postoperatively. 5- an accommodative element should be suspected if the eyes are initially straight or almost straight after surgery and then start to reconverge. It is therefore important to perform repeated refractions on all children and to correct any new accommodative elements accordingly.

25
DIFFERENTIAL DIAGNOSIS 1- congenital bilateral sixth nerve palsy, which is rare and can be excluded as described above.( video ) 2- secondary ( sensory ) esotropia due to organic eye disease. 3- nystagmus blockage syndrome in which convergence dampens a horizontal nystagmus. Nystagmus can be elicited on abduction and the infant adopts a face turn to fixate in the adducted position.

26
4- Duane syndrome type 1 and 3 ( video ) 5- Mobius syndrome.( video ) 6- strabismus fixux.
 5- Mobius syndrome.( video ) 6- strabismus fixux.")
27
ACCOMMODATIVE ESOTROPIA Near vision involves both accommodation and convergence. Accommodation is the process by which the eye focuses on a near target, by altering the curvature of the crystalline lens. Simultaneously the eyes converge, in order to fixate bi-foveally on the target. Both accommdation and convergence are quantitatively related to the proximity of the target, and have a fairly constant relationship to each other ( AC/A ratio ). Abnormalities of the AC/A ratio are important cause of certain types of esotropia.
. Abnormalities of the AC/A ratio are important cause of certain types of esotropia..")
28
Refractive accommodative esotropia Here the AC/A ratio is normal and esotropia is a physiological response to excessive hypermetropia, usually between +2 and +7 D. The considerable degree of accommodation required to focus clearly, even on a distant target, is accompanied by a proportionate amount of convergence, which is beyond the patient ’ s fusional divergence amplitude. It can not therefore be controlled and a manifest convergent squint results.

29
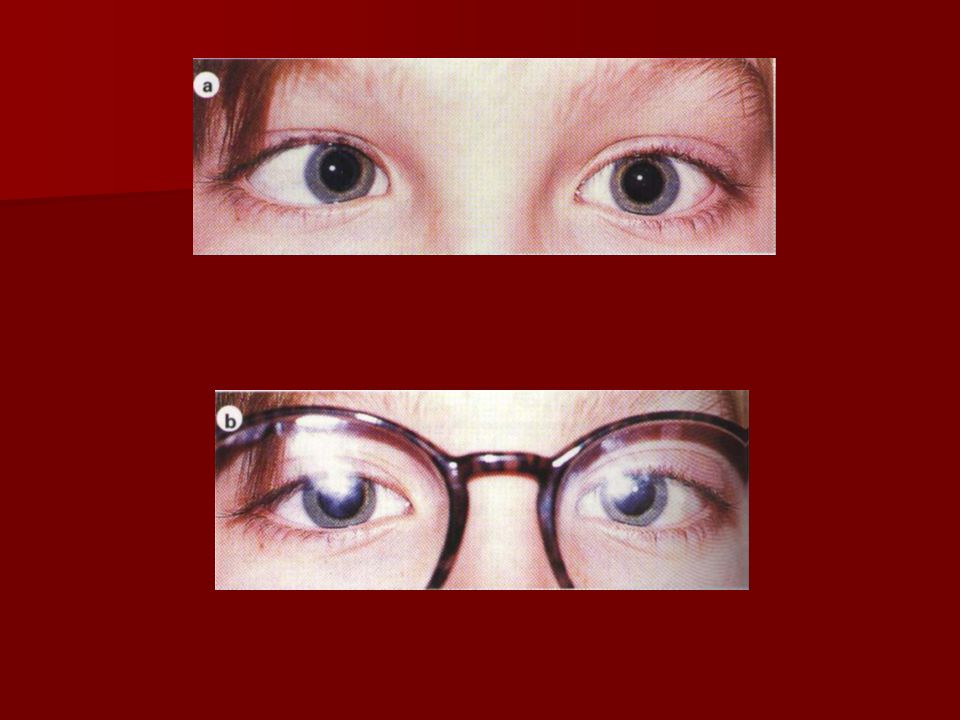
The magnitude of the deviation varies little ( usually < 10 ∆ ) between distance and near. The deviation typically presents at the age of 18 months to 3 years ( range of 6 months to 7 years ). 1- fully accommodative esotropia is eliminated by optical correction of hypermetropia and BSV is present at all distances with glasses but the deviation is present when glasses are not worn.
. 1- fully accommodative esotropia is eliminated by optical correction of hypermetropia and BSV is present at all distances with glasses but the deviation is present when glasses are not worn..")
31
2- constant accommodative esotropia is reduced, but not eliminated, by full correction of hypermetropia. Amblyopia and bilateral congenital superior oblique weakness are frequent. Most cases show suppression of the squinting eye although ARC may occur, but of lower grade than in microtropia.

33
Non-refractive accommodative esotropia This is associated with a high AC/A ratio in which a unit increase of accommodation is accompanied by a disproportionately large increase of convergence. This occurs independently of refractive error, although hypermetropia frequently coexists. It can be subdivided into : 1- convergence excess : - High AC/A ratio due to increased accommodative convergence ( accommodation is normal, convergence is increased ). - Normal near point of accommodation. - Straight eyes with BSV for distance. - Esotropia for near, usually with suppression. - Straight eyes through bifocals.
. - Normal near point of accommodation. - Straight eyes with BSV for distance. - Esotropia for near, usually with suppression. - Straight eyes through bifocals..")
34
2- hypoaccommodative convergence excess: - High AC/A ratio due to decreased accommodation ( accommodation is weak, necessitating increased effort, which produces overconvergence ). - Remote near point of accommodation. - Straight eyes with BSV for distance. - Esotropia for near, usually with suppression.

35
Medical treatment Refractive error should be corrected, as previously described. In children under the age of 6 years, the full cycloplegic refraction revealed on retinoscopy should be prescribed ( with a deduction only for the working distance ). In the fully accommodative refractive esotrope this will control the deviation for both near and distance. After the age of 8 years, refraction should be performed without cycloplegia and the maximal amount of ‘ plus ‘ that can be tolerated ( manifest hypermetropia ) prescribed.
. In the fully accommodative refractive esotrope this will control the deviation for both near and distance. After the age of 8 years, refraction should be performed without cycloplegia and the maximal amount of ‘ plus ‘ that can be tolerated ( manifest hypermetropia ) prescribed..")
36
For convergence excess esotropia bifocals may be prescribed to relieve accommodation ( and thereby accommodative convergence ), thus allowing the child to maintain bi-foveal fixation and ocular alignment at near. The minimum add required to achieve this is prescribed. The most satisfactory form of bifocals is the executive type in which the intersection crosses the lower border of the pupil.

37
The strength of the lower segment should be gradually reduced and eliminated by the early teenage years. Bifocals are best suited to hypoaccommodative esotropia and where the AC/A ratio is not overly excessive, when there is a reasonable chance of discarding bifocal correction with time. At higher levels surgery is the better long-term option. The ultimate prognosis for complete withdrawal of spectacles is related to the magnitude of the AC/A ratio and also the degree of hypermetropia and associated astigmatism. Spectacles may be needed only for close work.

38
Surgery The aim of surgery is to restore or enhance BSV or to improve the appearance of the squint. Surgery should only be considered if spectacles do not fully correct the deviation and every attempt has been made to treat amblyopia. - Bilateral medial rectus recessions are performed in patients in whom the deviation for near is greater than that for distance. - If there is no significant difference between distance and near measurements, and equal vision in both eyes, some perform unilateral medial rectus recession combined with lateral rectus resection, whereas others prefer bilateral medial rectus recessions. - In patients with residual amblyopia surgery is

39
Usually performed on the amblyopic eye. - In constant accommodative esotropia surgery to improve appearance is best delayed until requested by the child to avoid early consecutive exotropia and should only aim to correct the residual squint present with glasses on. TREATMENT OF AMBLYOPIA IS VERY IMPORTANT BEFORE CONTEMPLATING SURGERY.

40
MICROTROPIA Microtropia ( monofixation syndrome ),may be primary or follow surgery for a large deviation. It may occur in apparent isolation, but it is often associated with other conditions such as anisometropic amblyopia. Microtropia is more a description of binocular status than a specific diagnosis. For example a patient with fully accommodative esotropia may control to a microtropia rather than true bifoveal BSV with glasses. It is characterized by the following :

41
1- very small angle manifest deviation measuring 8∆ or less, which may or may not be detectable on cover testing. 2- central suppression scotoma of the deviating eye. 3- ARC with reduced stereopsis and variable peripheral fusional amplitudes. 4- anisometropia is often present, commonly with hypermetropia or hypermetropic astigmatism. 5- symptoms are rare unless there is an associated decompensating heterophoria. 6- treatment involves corrections of refractive errors and occlusion for amblyopia as indicated. Most patients remain stable and symptom free.

42
OTHER ESOTROPIAS NEAR ESOTROPIA 1-signs - No significant refractive error. - Orthophoria or small esophoria with BSV for distance. - Esotropia for near but normal or low AC/A ratio. - Normal near point of accommodation. 2- treatment is usually bilateral medial rectus recessions.

43
DISTANCE ESOTROPIA This typically affects healthy young adults who are often myopic. 1- signs - Intermittent or constant esotropia for distance. - Minimal or no deviation for near. - Normal bilateral abduction. - Fusional divergence amplitudes may be reduced. - Absence of neurological disease. 2- treatment is with prisms, until spontaneous resolution, or surgery in persistent cases.

44
NB It is important to distinguish this from sixth nerve paresis, which may be difficult on clinical grounds and investigation should be considered. Acute ( late onset ) esotropia This presents for no apparent reason around 5-6 years of age. 1- signs - Sudden onset of diplopia and esotropia. - Normal ocular motility and no significant refractive error. - Underlying sixth nerve palsy must be excluded. 2- treatment is aimed at quickly re-establishing BSV to prevent suppression with prisms, botulinum toxin or surgery.
 esotropia This presents for no apparent reason around 5-6 years of age. 1- signs - Sudden onset of diplopia and esotropia. - Normal ocular motility and no significant refractive error. - Underlying sixth nerve palsy must be excluded. 2- treatment is aimed at quickly re-establishing BSV to prevent suppression with prisms, botulinum toxin or surgery..")
45
Secondary ( sensory ) esotropia This is caused by a unilateral reduction in VA which interferes with or abolishes fusion, such as cataract, optic atrophy or hypoplasia, macular scarring or retinoblastoma. FUNDUS EXAMINATION UNDER MYDRIASIS IS THEREFORE ESSENTIAL IN ALL CHILDREN WITH STRABISMUS. CONSECUTIVE ESOTROPIA This follows surgical overcorrection of an exodeviation. If it occurs following surgery for an intermittent exotropia in a child it should not be allowed to persist for more than 6 weeks without further intervention.

46
Cyclic esotropia This is a very rare condition characterized by alternating manifest esotropia with suppression and BSV, each lasting 24 hours. The condition may persist for months or years and the patient may eventually develop a constant esotropia requiring surgery. Earlier correction of the full manifest angle can be successfully performed during the intermittent phase.

Similar presentations











 Journal of American Association for Peadiatric Ophthalmology and strabismus 2008.>")
 may turn in, out, up, or down can be present in one or both eyes cross-eyed, squint. Vergence Duction.>")






 591-8860>")


>")
