Download presentation
Presentation is loading. Please wait.

1
RISK STRATIFICATION IN ACUTE CORONARY SYNDROMES ADAM OSTER PGY-2 JANUARY 9, 2002 RESIDENT ORAL PRESENTATION

2
RISK STRATIFICATION IN ACS Objectives –Discuss the major risk stratification models –Examine strategies to define the very low risk group –The future of risk stratification

3
The Undifferentiated Chest Pain Patient Risk of ACI Risk of short-term mortality, cardiac events or complications Risk of long-term mortality, events or complications

4
How Predictive are Routine Historic Features? Goodacre et al. How Useful are Clinical Features in the Diagnosis of Acute, Undifferentiated Chest Pain? Academic Emergency Medicine, vol. 9, no. 3, 2002. –Prospectively evaluated 893 CPOU (normal ECG, no CHF or arrhythmia) –ST seg monitoring, troponin T >6hrs, +/-EST or thallium –F/U at 3d and 6mo, 12mo –Endpoints: AMI at presentation and ACS (AMI at any time, pos. EST cardiac death, arrhythmia, revascularisation procedure) –Assessed predictive power of routine historic features
 –ST seg monitoring, troponin T >6hrs, +/-EST or thallium –F/U at 3d and 6mo, 12mo –Endpoints: AMI at presentation and ACS (AMI at any time, pos. EST cardiac death, arrhythmia, revascularisation procedure) –Assessed predictive power of routine historic features.")
5
Goodacre et al. How Useful are Clinical Features in the Diagnosis of Acute, Undifferentiated Chest Pain? Academic Emergency Medicine, vol. 9, no. 3, 2002. Features Predictive of AMI: Multivariate analysis table Didn’t make it to MV analysis Radiation to L arm radiation to throat radiation to back heavy pressure diaphoresis relief after nitro Multivariate analysis table Didn’t make it to MV analysis Radiation to L arm radiation to throat radiation to back heavy pressure diaphoresis relief after nitro

6
Goodacre et al. How Useful are Clinical Features in the Diagnosis of Acute, Undifferentiated Chest Pain? Academic Emergency Medicine, vol. 9, no. 3, 2002. Features Predictive of ACS: These features do not have the sensitivities or specificities to rule in or rule out the diagnoses on their own Many commonly used clinical features were not independent predictors or AMI/ACS maybe underpowered to detect failure of N/V/D may reflect that these features are typically present in larger inf AMI with ECG changes These features do not have the sensitivities or specificities to rule in or rule out the diagnoses on their own Many commonly used clinical features were not independent predictors or AMI/ACS maybe underpowered to detect failure of N/V/D may reflect that these features are typically present in larger inf AMI with ECG changes

7
Pope et al. Missed Diagnoses of Acute Cardiac Ischemia in the Emergency Department. New England Journal of Medicine vol. 342, no. 16, 2000. 10 689 patients Data collected for 30d (hospitalised patients) or at 24 to 72hrs for non- hospitalised patients Outcomes assigned by physicians at study sites using pre-defined criteria
 or at 24 to 72hrs for non- hospitalised patients Outcomes assigned by physicians at study sites using pre-defined criteria.")
8
Pope et al. Missed Diagnoses of Acute Cardiac Ischemia in the Emergency Department. New England Journal of Medicine vol. 342, no. 16, 2000. Final Diagnosis –1866 (17%) ACI –894 (8.5%) AMI –972 (9%) unstable angina –21% non-ischemic cardiac problem –55% non-cardiac
 ACI –894 (8.5%) AMI –972 (9%) unstable angina –21% non-ischemic cardiac problem –55% non-cardiac.")
9
Pope et al. Missed Diagnoses of Acute Cardiac Ischemia in the Emergency Department. New England Journal of Medicine vol. 342, no. 16, 2000. 22 missed unstable angina (2.26%) –MC diagnosis; stable angina, atypical chest pain
 –MC diagnosis; stable angina, atypical chest pain.")
10
Pope et al. Missed Diagnoses of Acute Cardiac Ischemia in the Emergency Department. New England Journal of Medicine vol. 342, no. 16, 2000. 19 missed AMIs (2.1% of 894) –MC diagnosis; non-cardiac chest pain, pulmonary conditions and stable angina
 –MC diagnosis; non-cardiac chest pain, pulmonary conditions and stable angina.")
11
Pope et al. Missed Diagnoses of Acute Cardiac Ischemia in the Emergency Department. New England Journal of Medicine vol. 342, no. 16, 2000. Factors associated with non-hospitalisation for patients with missed ACI –female –<55 –non-white –chief complaint of SOB –normal ECG –30d adjusted risk of mortality 1.7 times higher if not hospitalised (95% CI 0.7 to 5.2) Low rate of missed ACI/AMI diagnosis but associated with a poor outcome Low rate of missed ACI/AMI diagnosis but associated with a poor outcome
 Low rate of missed ACI/AMI diagnosis but associated with a poor outcome Low rate of missed ACI/AMI diagnosis but associated with a poor outcome.")
12
ACI Prediction Pozen et al. The Usefulness of a Predictive Instrument to Reduce Inappropriate Admission to the Coronary Care Unit. Annals of Internal Medicine, Vol. 92, 1980. –Original predictive instrument derived from 2801 patient encounters, 1979-1980. Designed to predict unstable angina and AMI Of 59 candidate clinical variables, 7 found to be predictive of ACI estimate (0-100%) provides patients likelihood of having ACI
 provides patients likelihood of having ACI.")
13
Pozen et al. The Usefulness of a Predictive Instrument to Reduce Inappropriate Admission to the Coronary Care Unit. Annals of Internal Medicine, Vol. 92, 1980. Chest Pain or Pressure or left arm pain? Chief Complaint Yes but not Chief Complaint No No Previous MI Prev. MI or nitro use Both MI and Nitro use No Previous MI Prev. MI or nitro use Both MI and Nitro use No Previous MI Prev. MI or nitro use Both MI and Nitro use ST and T analysis

14
Pozen et al. The Usefulness of a Predictive Instrument to Reduce Inappropriate Admission to the Coronary Care Unit. Annals of Internal Medicine, Vol. 92, 1980. Original was programmed onto a handheld calculator. This is the Table Version Original was programmed onto a handheld calculator. This is the Table Version

15
Selker et al. A Tool for Judging Coronary Care Unit Admission Appropriateness,Valid for Both Real Time and Retrospective Use: A Time-Insensitive Predictive Instrument (TIPI) for Acute Cardiac Ischemia: A Multicentre Study. Medical Care. Vol. 29.1991. Prospectively tested OPI (N=2320) –Intervention vs Control proven ACI; no change in admission patterns proven no ACI; sig. lower CCU admission rates (24% to 17%, p=0.03) ED d/c home; 51% vs 44% patients with <50% prob ACI; –22% reduction in FP diagnosis (p=0.002) patients with >50% prob ACI; –no stat sig. diagnostic benefit Instrument most helpful in making a correct diagnosis in patients with atypical or less definitive symptoms In higher probability patients, physician judgement alone suffices Instrument most helpful in making a correct diagnosis in patients with atypical or less definitive symptoms In higher probability patients, physician judgement alone suffices
 for Acute Cardiac Ischemia: A Multicentre Study. Medical Care. Vol Prospectively tested OPI (N=2320) –Intervention vs Control proven ACI; no change in admission patterns proven no ACI; sig. lower CCU admission rates (24% to 17%, p=0.03) ED d/c home; 51% vs 44% patients with <50% prob ACI; –22% reduction in FP diagnosis (p=0.002) patients with >50% prob ACI; –no stat sig. diagnostic benefit Instrument most helpful in making a correct diagnosis in patients with atypical or less definitive symptoms In higher probability patients, physician judgement alone suffices Instrument most helpful in making a correct diagnosis in patients with atypical or less definitive symptoms In higher probability patients, physician judgement alone suffices.")
16
Selker et al. A Tool for Judging Coronary Care Unit Admission Appropriateness,Valid for Both Real Time and Retrospective Use: A Time-Insensitive Predictive Instrument (TIPI) for Acute Cardiac Ischemia: A Multicentre Study. Medical Care. Vol. 29.1991. patients proved not to have ACI –ave. predicted probability 24% patients proved to have ACI –ave. predicted probability 62%
 for Acute Cardiac Ischemia: A Multicentre Study. Medical Care. Vol patients proved not to have ACI –ave. predicted probability 24% patients proved to have ACI –ave. predicted probability 62%.")
17
Original ACI Predictive Instrument Critique of Selker Study –Although prospective and controlled, randomisation method was different among the 3 study hospitals –Blinding of predicted probability to clinicians determining ultimate diagnosis questionable –Gold Standard poorly defined –Outcome of those discharged home not published –Generalisability to different settings (e.g Telemetry Units) OPI should be used in conjunction with EP judgement No specific cutoff point was determined OPI should be used in conjunction with EP judgement No specific cutoff point was determined
 OPI should be used in conjunction with EP judgement No specific cutoff point was determined OPI should be used in conjunction with EP judgement No specific cutoff point was determined")
18
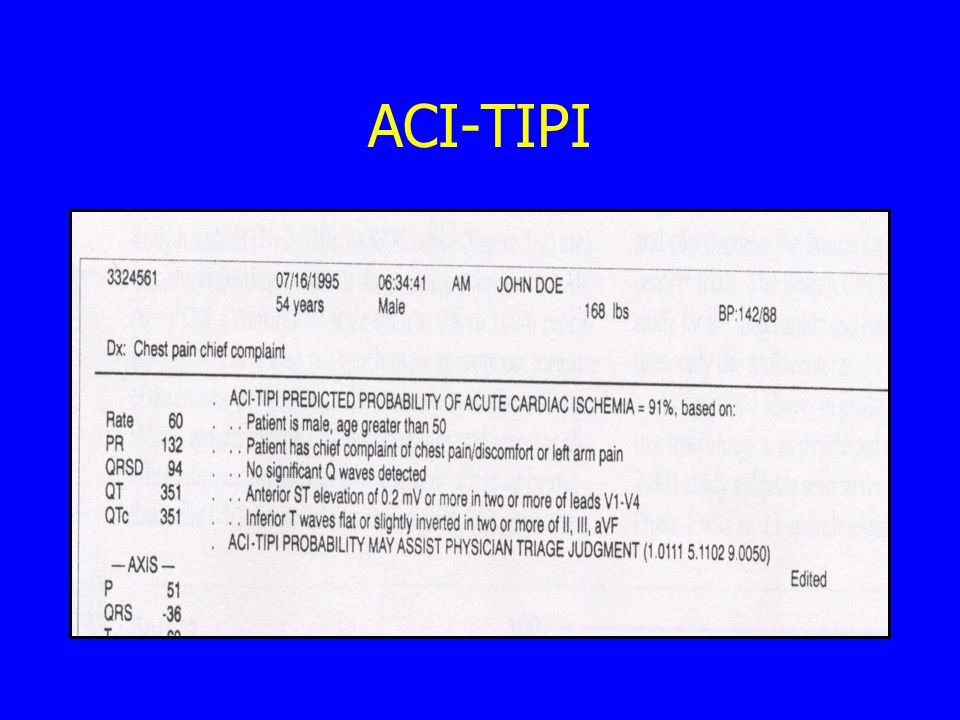
ACI-TIPI Acute Coronary Ischemia, Time- Insensitive Predictive Instrument –next generation of ACI predictive tools modified the clinical variables computerised interpretation of ECG designed for prospective and retrospective use (time- insensitive) prediction printed onto ECG change in performance –designed to predict AMI > unstable angina in order to produce less false negatives for AMI By giving more weight to greater ST deviation
 prediction printed onto ECG change in performance –designed to predict AMI > unstable angina in order to produce less false negatives for AMI By giving more weight to greater ST deviation")
19
ACI-TIPI

21
Age, sex chest pain or pressure or left arm pain as primary complaint pathologic Q waves presence and degree of ST segment elevation or depression T wave elevation or inversion

22
ACI-TIPI original predictive instrument and ACI- TIPI had virtually identical area under ROC curve (0.89) when tested prospectively and simultaneously with OPI (N=2320) higher sensitivity for AMI than OPI
 when tested prospectively and simultaneously with OPI (N=2320) higher sensitivity for AMI than OPI")
23
Selker et al. Annals of Internal Medicine. Vol 129. No. 11, 1998. –N=10 689 with chest pain or Sx c/w ischemia –ACI-TIPI prediction either printed or not printed on ECG; 7 alternating months of intervention and control –outcomes: triage to CCU, telemetry,ward or home, patient diagnosis and patient outcomes –diagnosis assigned by blinded site physician on basis of all available information after 30d period –also looked at triage decisions relative to capacity of CCU vs telemetry unit and level of training of EP

24
Selker et al. Annals of Internal Medicine. Vol 129. No. 11, 1998. Patients with ACI (unstable angina or AMI) –intervention not associated with a change in admission –mean predicted probability of ACI 59%
 –intervention not associated with a change in admission –mean predicted probability of ACI 59%.")
25
Selker et al. Annals of Internal Medicine. Vol 129. No. 11, 1998. Patients with Stable Angina –intervention associated with reduction in CCU admission of 50% (26% to 13%) 95% CI -70% to -17% –increase in discharge home from 20% to 22% (RRI 10%) 95% CI -29 to 70%, p=0.02
 95% CI -70% to -17% –increase in discharge home from 20% to 22% (RRI 10%) 95% CI -29 to 70%, p=0.02.")
26
Selker et al. Annals of Internal Medicine. Vol 129. No. 11, 1998. Patients without ACI –intervention associated with reduction in CCU admission of 16% (15% to 12%, –95% CI -30% to 0% –increased in ED discharge to home from 49% to 52%, RRI of 6% –0-14%, p=0.09 –reductions in admission were greatest in low (<10%) probability group (OR 0.51) –CI 0.28-0.91 –mean predicted probability of ACI, 21%
 probability group (OR 0.51) –CI –mean predicted probability of ACI, 21%.")
27
Selker et al. Annals of Internal Medicine. Vol 129. No. 11, 1998. 30 day mortality –patients discharged home control 0.2% intervention 0.5%, p=0.2

28
ACI-TIPI Summary –0-100% probability of ACI –tested in ED and found to be accurate for ACI and non-ACI –incorporated into the conventional 12-lead ECG –time-insensitive

29
ACI-TIPI Future Studies –prospective trial in various types of EDs –effect on time to disposition decision –increase in discharge home and decreased utilisation of in-hospital resources and personnel for cardiac work-up –pre-hospital use –applicability to population subgroups

30
Goldman Chest Pain Protocol Goldman et al. Prediction of the Need for Intensive Care in Patients Who Come to the Emergency Departments With Acute Chest Pain. New England Journal of Medicine. Vol 334. 1996. –Designed to predict the risk of major complications in patients presenting to the ED with chest pain –an aid to triaging to ICU/CCU setting –derivation of decision rule N=10 682 [1982-1984] –validation of CDR N=4676 [1990-1994] –validation at other sites N=1033 [1997-1999] Goldman: lots of research in this area. Decided to focus not on prediction of AMI but on prediction of complication in ACS patients Goldman: lots of research in this area. Decided to focus not on prediction of AMI but on prediction of complication in ACS patients

31
Goldman et al. Prediction of the Need for Intensive Care in Patients Who Come to the Emergency Departments With Acute Chest Pain. New England Journal of Medicine. Vol 334. 1996. Outcomes (defined apriori) –Major events (requiring ICU/CCU care) VF, CA, 3rd degree block, pacemaker insertion, emergent cardioversion, cardiogenic shock, IABP, intubation, recurrent chest pain requiring PCI< CABG within 72hrs –Intermediate Events (no ICU/CCU) A. flutt., Mobitz Type I or II (no pacemaker), sinus brad., pulmonary edema, infarct extension
 –Major events (requiring ICU/CCU care) VF, CA, 3rd degree block, pacemaker insertion, emergent cardioversion, cardiogenic shock, IABP, intubation, recurrent chest pain requiring PCI< CABG within 72hrs –Intermediate Events (no ICU/CCU) A. flutt., Mobitz Type I or II (no pacemaker), sinus brad., pulmonary edema, infarct extension.")
32
Goldman et al. Prediction of the Need for Intensive Care in Patients Who Come to the Emergency Departments With Acute Chest Pain. New England Journal of Medicine. Vol 334. 1996. Risk of major event within 72hrs (derivation phase) –age >60 –male –pain same as prior infarction or worse than previous angina –SBP<100 –Crackles above the bases bilaterally –abnormality on ECG STE or Q waves not known to be old STD or T wave inversion not known to be old
 –age >60 –male –pain same as prior infarction or worse than previous angina –SBP<100 –Crackles above the bases bilaterally –abnormality on ECG STE or Q waves not known to be old STD or T wave inversion not known to be old.")
33
Goldman et al. Prediction of the Need for Intensive Care in Patients Who Come to the Emergency Departments With Acute Chest Pain. New England Journal of Medicine. Vol 334. 1996. Grouped into 4 risk groups based on risk of major event at 24hrs –very low –low –moderate –high

34
Goldman et al. Prediction of the Need for Intensive Care in Patients Who Come to the Emergency Departments With Acute Chest Pain. New England Journal of Medicine. Vol 334. 1996. Rate of events by risk group at 72hrs

35
Goldman et al. Prediction of the Need for Intensive Care in Patients Who Come to the Emergency Departments With Acute Chest Pain. New England Journal of Medicine. Vol 334. 1996. After initial 12hrs the risk of a major event depended more on the occurrence of an event than the initial risk category

36
Goldman et al. Prediction of the Need for Intensive Care in Patients Who Come to the Emergency Departments With Acute Chest Pain. New England Journal of Medicine. Vol 334. 1996. Critique –ECG and cardiac enzymes at discretion of physician –derivation set 28% of eligible patients not enrolled or ultimately did not contribute to results in of discharged patients 35% did not follow-up –validation set 17% of discharged patients followed-up

37
Goldman et al. Prediction of the Need for Intensive Care in Patients Who Come to the Emergency Departments With Acute Chest Pain. New England Journal of Medicine. Vol 334. 1996. Critique –validation set event rate > derivation set (2.8 vs 1.8, p<0.01) –revascularisation procedures more common in validation set than derivation set
 –revascularisation procedures more common in validation set than derivation set.")
38
Application of Goldman Clinical Decision Rule Reily et al. Impact of A Clinical Decision Rule on Hospital Triage of Patients With Suspected Acute Cardiac Ischemia in the Emergency Department. JAMA, no.288. Vol.3, 2002. –Pre-intervention and intervention cohort –Outcomes assessed; Safety and Efficiency Safety -- percent of patients triaged to CCU/telemetry who had cardiac events within 72hrs Efficiency -- proportion of patients who did not experience a cardiac event triaged to non-monitored ward or ED CPOU

39
Reily et al. Impact of A Clinical Decision Rule on Hospital Triage of Patients With Suspected Acute Cardiac Ischemia in the Emergency Department. JAMA, 288, vol.3, 2002. Included patients without chest pain Excluded patients discharged home –but studied a separate cohort of patients discharged home directly from ED for complications within 72hrs to monitor the safety of the discharge decision added LBBB (not known to be old) to ECG evidence of acute ischemia Intention-to-treat analysis Adam Oster: Eps responsible for admitting patients but cardiology consult and permission required for CCU/telemetry admissions Adam Oster: Eps responsible for admitting patients but cardiology consult and permission required for CCU/telemetry admissions
 to ECG evidence of acute ischemia Intention-to-treat analysis Adam Oster: Eps responsible for admitting patients but cardiology consult and permission required for CCU/telemetry admissions Adam Oster: Eps responsible for admitting patients but cardiology consult and permission required for CCU/telemetry admissions.")
40
Reily et al. Impact of A Clinical Decision Rule on Hospital Triage of Patients With Suspected Acute Cardiac Ischemia in the Emergency Department. JAMA, 288, vol.3, 2002.

41
98.6% follow-up groups similar 35 major complications in intervention group Safety Outcome –94% vs 89%, NS. Efficiency Outcome –36% vs 21% (RRI 15%, CI 8%-21%, p<0.001) largest change in triaging patterns between pre-intervention and intervention group occurred in very low risk patients. No sig. Different changes in higher risk groups Much larger sample sizes would be needed to narrower confidence intervals for the decisions rules safety (around 15000) largest change in triaging patterns between pre-intervention and intervention group occurred in very low risk patients. No sig. Different changes in higher risk groups Much larger sample sizes would be needed to narrower confidence intervals for the decisions rules safety (around 15000)
 largest change in triaging patterns between pre-intervention and intervention group occurred in very low risk patients. No sig. Different changes in higher risk groups Much larger sample sizes would be needed to narrower confidence intervals for the decisions rules safety (around 15000) largest change in triaging patterns between pre-intervention and intervention group occurred in very low risk patients. No sig. Different changes in higher risk groups Much larger sample sizes would be needed to narrower confidence intervals for the decisions rules safety (around 15000).")
42
Reily et al. Impact of A Clinical Decision Rule on Hospital Triage of Patients With Suspected Acute Cardiac Ischemia in the Emergency Department. JAMA, 288, vol.3, 2002. Patients discharged home (subgroup analysis) N=326 –no complications in 300 –26 LTFU no recorded deaths Adam Oster: follow-up would miss small, uncomplicated MIs Adam Oster: follow-up would miss small, uncomplicated MIs
 N=326 –no complications in 300 –26 LTFU no recorded deaths Adam Oster: follow-up would miss small, uncomplicated MIs Adam Oster: follow-up would miss small, uncomplicated MIs.")
43
Braunwald Risk Stratification Braunwald E. Unstable Angina: A Classification. Circulation. 1989; vol. 2 no. 7 –Derived scoring system in 1989 for unstable angina –designed to aid in clinical decision making and clinical trials

44
Braunwald E. Unstable Angina: A Classification. Circulation. 1989; vol. 2 no. 7.

45
Prospective Validation of the Braunwald Classification Calvin et al. Risk Stratification in Unstable Angina. JAMA. 1995. Vol 273, no. 2 –determined elements of the Braunwald RS that predict risk of complications –Consecutive patients admitted to CCU with UA, N=393 –Outcomes: in-hospital death, MI, CHF, VT or VF –all patients treated at discretion of physician eligibility criteria: ischemic type chest pain either responsive to NO or assoc with STD lasting >20mins at rest or exertional chest pain increasing in frequency MI ruled out eligibility criteria: ischemic type chest pain either responsive to NO or assoc with STD lasting >20mins at rest or exertional chest pain increasing in frequency MI ruled out

46
Calvin et al. Risk Stratification in Unstable Angina. JAMA. 1995. Vol. 273, no. 2 4 clinical factors associated with development of the composite endpoint (n=30) –MI <14d prior to presentation (OR 5.72, 1.92- 16.97) –need to IV nitro (OR 2.33, 1.31-4.17) –lack of bBlocker or CCB use prior to presentation (OR 3.83, 1.55-9.42) –baseline STD (OR 2.81, 1.45-5.47) Example of calculation male with previous <14d MI and no use of bblocker 5.72x3.82=21.8 (CI 2.5-159) not prospectively validated wide confidence intevals likely underpowered novel in that uses intensity of therapy as an element to classify Example of calculation male with previous <14d MI and no use of bblocker 5.72x3.82=21.8 (CI 2.5-159) not prospectively validated wide confidence intevals likely underpowered novel in that uses intensity of therapy as an element to classify
 –MI <14d prior to presentation (OR 5.72, ) –need to IV nitro (OR 2.33, ) –lack of bBlocker or CCB use prior to presentation (OR 3.83, ) –baseline STD (OR 2.81, ) Example of calculation male with previous <14d MI and no use of bblocker 5.72x3.82=21.8 (CI ) not prospectively validated wide confidence intevals likely underpowered novel in that uses intensity of therapy as an element to classify Example of calculation male with previous <14d MI and no use of bblocker 5.72x3.82=21.8 (CI ) not prospectively validated wide confidence intevals likely underpowered novel in that uses intensity of therapy as an element to classify.")
47
Thrombolysis in Myocardial Infarction (TIMI) Risk Stratification Antman et al. JAMA. 2000. Vol. 284, No.7. –TIMI RS based on data from TIMI 11b (N=3910) and ESSENCE (N=3171) –Test cohort (TIMI UFH) –Validation cohort (TIMI and ESSENCE enoxaparin groups and ESSENCE UFH) –TIMI RS derived in test cohort
 and ESSENCE (N=3171) –Test cohort (TIMI UFH) –Validation cohort (TIMI and ESSENCE enoxaparin groups and ESSENCE UFH) –TIMI RS derived in test cohort.")
48
TIMI Risk Stratification Antman et al. JAMA. 2000. Vol. 284, No.7. Endpoints –all-cause death, new or recurrent MI or UR at 14d post-randomisation Eligibility (1 of following) –admitted patients who presented within 24hrs with symptoms of unstable angina/NSTEMI –transient STE or STD or 0.05mV (TIMI) or 0.01mV (ESSENCE) –known CAD* –increased Troponin
 –admitted patients who presented within 24hrs with symptoms of unstable angina/NSTEMI –transient STE or STD or 0.05mV (TIMI) or 0.01mV (ESSENCE) –known CAD* –increased Troponin.")
49
TIMI Risk Stratification Antman et al. JAMA. 2000. Vol. 284, No.7 All patients received ASA randomised to enoxaparin or UFH Derivation cohort; –tested 12 candidate variables ageST deviation at least 3 CAD risk factors>2 anginal events in 24hrs significant coronary stenosisuse of ASA in last 7d prior MIelevated cardiac markers prior CABGprior history of CHF prior PTCA

50
TIMI Risk Stratification Antman et al. JAMA. 2000. Vol. 284, No.7 Derivation cohort –7 variables remained statistically significant after multivariate analysis Age >65 at least 3 CAD RF STD severe anginal symptoms prior stenosis >50% use of ASA over previous 7d elevated serum cardiac markers *paraneter estimates (odds ratios) for each variable of similar magnitude
 for each variable of similar magnitude.")
51
TIMI Risk Stratification Antman et al. JAMA. 2000. Vol. 284, No.7 Small numbers of patients in extreme risk scores required combining criteria of known stenosis >50%, insensitive to missing data and remained a significant predictor derivation of RS

52
TIMI Risk Stratification Antman et al. JAMA. 2000. Vol. 284, No.7 Validation Phase –different rate of increase for rate of composite endpoint in UFH vs enoxaparin –merged the databases –TIMI RS and treatment were both significant predictors of risk of the composite endpoint

53
TIMI Risk Stratification Antman et al. JAMA. 2000. Vol. 284, No.7 Predicting the individual components of the composite endpoint all statistically sig.

54
TIMI Risk Stratification Antman et al. JAMA. 2000. Vol. 284, No.7 Caveats and Critique –tested on admitted patients with unstable angina/NSTEMI –Validation Phase not prospective –cohort who qualified for enrolment in a phase III study; ?generalisabilty to all-comers with chest pain –enrolment criteria for TIMI 11b changed during the trial –duration of treatment different between UFH (3-8d) and enoxaparin (8d or hospital discharge) –elevated CKMB was both a predictor of an endpoint as well as part of the definition of an endpoint –CKMB was the marker in TIMI but now use Troponin without study to prove similarly predictive Initially used history of CAD as entry criteria but then switched to STD or pos. CKMB
 and enoxaparin (8d or hospital discharge) –elevated CKMB was both a predictor of an endpoint as well as part of the definition of an endpoint –CKMB was the marker in TIMI but now use Troponin without study to prove similarly predictive Initially used history of CAD as entry criteria but then switched to STD or pos. CKMB.")
55
TIMI Risk Stratification Antman et al. JAMA. 2000. Vol. 284, No.7 Support –consider using on chest pain patients to be admitted –simple to use and to communicate to consultants –cannot use to determine who is at low risk –cannot use to determine who is safe for discharge

56
DEFINING THE LOW RISK GROUP Previous studies not designed to define the low risk group (or group safe to discharge home) Many studies evaluating Troponin to define low risk group Only one which uses combination of RS criteria and serum marker in an attempt to define
 Many studies evaluating Troponin to define low risk group Only one which uses combination of RS criteria and serum marker in an attempt to define")
57
Combining Goldman and Troponin Limkakeng et al. Combination of Goldman Risk and Initial Cardiac Troponin I for Emergency Department Chest Pain Patient Risk Stratification. Academic Emergency Medicine, Vol. 8, No. 7, 2001. –Prospective cohort study of consecutive ED chest pain patients –Goldman RS score calculated and presentation TnI determined –followed those with Goldman RS <4% and single negative TnI Testing the hypothesis that low Goldman RS and neg TnI would confer a risk of death, MI or UR of <1%

58
Limkakeng et al. Combination of Goldman Risk and Initial Cardiac Troponin I for Emergency Department Chest Pain Patient Risk Stratification. Academic Emergency Medicine, Vol. 8, No. 7, 2001. >24 yrs c/o chest pain had an ECG patients followed daily for complications and interventions 30d follow-up for 91% of participants ECG classified by treating EP TnI collected EPs blinded to Goldman Final data set included those with Goldman <4% and negative TnI Primary endpoints –death, AMI, UR

59
Limkakeng et al. Combination of Goldman Risk and Initial Cardiac Troponin I for Emergency Department Chest Pain Patient Risk Stratification. Academic Emergency Medicine, Vol. 8, No. 7, 2001. Of 2322 pts 1657 had low Goldman RS 998 had low Goldman and initially negative TnI (<0.3ng/ml) 49 patients experienced an endpoint (4.9%) AMI N=23 (2.3%) Death N=10 (1.0%) PCI/stent/CABG N= 23 (2.3%) 4 patients initially discharged home experienced a cardiac event some patients experienced more than 1 endpoint
 49 patients experienced an endpoint (4.9%) AMI N=23 (2.3%) Death N=10 (1.0%) PCI/stent/CABG N= 23 (2.3%) 4 patients initially discharged home experienced a cardiac event some patients experienced more than 1 endpoint.")
60
Limkakeng et al. Combination of Goldman Risk and Initial Cardiac Troponin I for Emergency Department Chest Pain Patient Risk Stratification. Academic Emergency Medicine, Vol. 8, No. 7, 2001. Sensitivity and NPV to detect a 30d endpoint better with combined predictors than either alone neither criteria alone or in combination achieved <1% likelihood of a 30d endpoint variable times to TnI determination

61
Hamm et al. Emergency Room Triage of Patients With Acute Chest Pain by Means of Rapid Testing for Cardiac Troponin T or Troponin I. New England Journal of Medicine vol. 337, 1997. N=773 with chest pain of <12hrs absence of STE TnT or TnI drawn at least 6hrs after onset of chest symptoms 603 patient had neg. TnI on serial testing –AMI in 1 –death in 1 62 pts with initially neg. markers who subsequently tested positive Unsafe to discharge based on initially neg. Trop Still must wait for maximal sensitivity to consider using to RS Unsafe to discharge based on initially neg. Trop Still must wait for maximal sensitivity to consider using to RS

62
Summary 4 major RS models –ACI-TIPI probability of ACI in undiff. CP –Goldman Risk of Complications in Chest Pain –Braunwald Death, MI, UR in UA patients –TIMI Death, MI, UR within 14d in admitted CP None able to identify the low risk chest pain patient or the patient safe to discharge Home

63
The Future of Risk Stratification Combination of ACI-TIPI with Troponin Prospectively validate TIMI

Similar presentations
















 Definition of ACS Signs and symptoms of ACS Gender and age related difference in ACS Pathophysiology.>")


