Download presentation
Presentation is loading. Please wait.

1
Intertrochanteric Fractures Optimal Treatment in 2007 Michael R. Baumgaertner, MD Original Authors: Steve Morgan, MD; March 2004; New Author: Michael R. Baumgaertner, MD; Revised January 2007

2
Lecture Objectives Review: F Principles of treatment Understand & Optimize F Variables influencing patient and fracture outcome Introduce: F Recent Evidenced based med Suggest: F Technical Tips to avoid common problems Review: F Principles of treatment Understand & Optimize F Variables influencing patient and fracture outcome Introduce: F Recent Evidenced based med Suggest: F Technical Tips to avoid common problems

3
Hip Fracture PATIENT Outcome Predictors Pre-injury physical & cognitive status Ability to visit a friend or go shopping Presence of home companion Postoperative ambulation Postoperative complications (Cedar, Thorngren, Parker, others) Pre-injury physical & cognitive status Ability to visit a friend or go shopping Presence of home companion Postoperative ambulation Postoperative complications (Cedar, Thorngren, Parker, others) Uncontrolled Surgeon Controlled!
 Pre-injury physical & cognitive status Ability to visit a friend or go shopping Presence of home companion Postoperative ambulation Postoperative complications (Cedar, Thorngren, Parker, others) Uncontrolled Surgeon Controlled!")
4
A public heath care cri $ i $ : 130,000 IT Fx / year in U.S. & will double by 2050… We must do better!! 1-2 units PRBC transfused 3-5+ days length of stay 1-2 units PRBC transfused 3-5+ days length of stay Even when surgery is “successful”: 4-12% fixation failure

5
Preoperative Management the evidence suggests: “Tune up” correctable comorbidities Operate within 48°; avoid night surgery Maintain extremity in position of comfort General versus spinal anaesthesia? “Tune up” correctable comorbidities Operate within 48°; avoid night surgery Maintain extremity in position of comfort General versus spinal anaesthesia? Anderson, JBJS(B) ‘93 Zuckerman, JBJS(A) ‘95 Davis, Anaesth & IntCare ‘81; Valentin, Br J Anaesth ‘86 Buck’s traction of no value (RCT) Randomized, prospective trials (RCTs): no difference
 ‘93 Zuckerman, JBJS(A) ‘95 Davis, Anaesth & IntCare ‘81; Valentin, Br J Anaesth ‘86 Buck’s traction of no value (RCT) Randomized, prospective trials (RCTs): no difference.")
6
Intertrochanteric Femur Anatomic considerations Capsule inserts on IT line anteriorly, but at midcervical level posteriorly Muscle attachments determine deformity Capsule inserts on IT line anteriorly, but at midcervical level posteriorly Muscle attachments determine deformity

7
Plain Films l AP pelvis l Cross-table lateral Plain Films l AP pelvis l Cross-table lateral l ER Traction view when in any doubt!! l ER Traction view when in any doubt!! Radiographs

8
Uncontrolled factors Bone Quality Fracture Geometry Controlled factors Quality of Reduction Implant Placement Implant Selection Uncontrolled factors Bone Quality Fracture Geometry Controlled factors Quality of Reduction Implant Placement Implant Selection Kaufer, CORR 1980 Factors Influencing Construct Strength: This lecture will examine each factor

9
“STABILITY” The ability of the reduced fracture to support physiologic loading Fracture Stability relates not only to the # of fragments but the fracture plane as well Uncontrolled factor: Fracture geometry

10
AO / OTA 31 Fracture Classification in 2006

11
StableUnstable Uncontrolled factor: Fracture geometry

12
AO/OTA31A3: The highly unstable “pertrochanteric” fractures! Uncontrolled factor: Fracture geometry

13
A 33 year old pt with intertrochanteric fracture following a fall from height- Note the dense, cancellous bone throughout the proximal femur; nothing like a geriatric fracture Uncontrolled factor: Bone quality

14
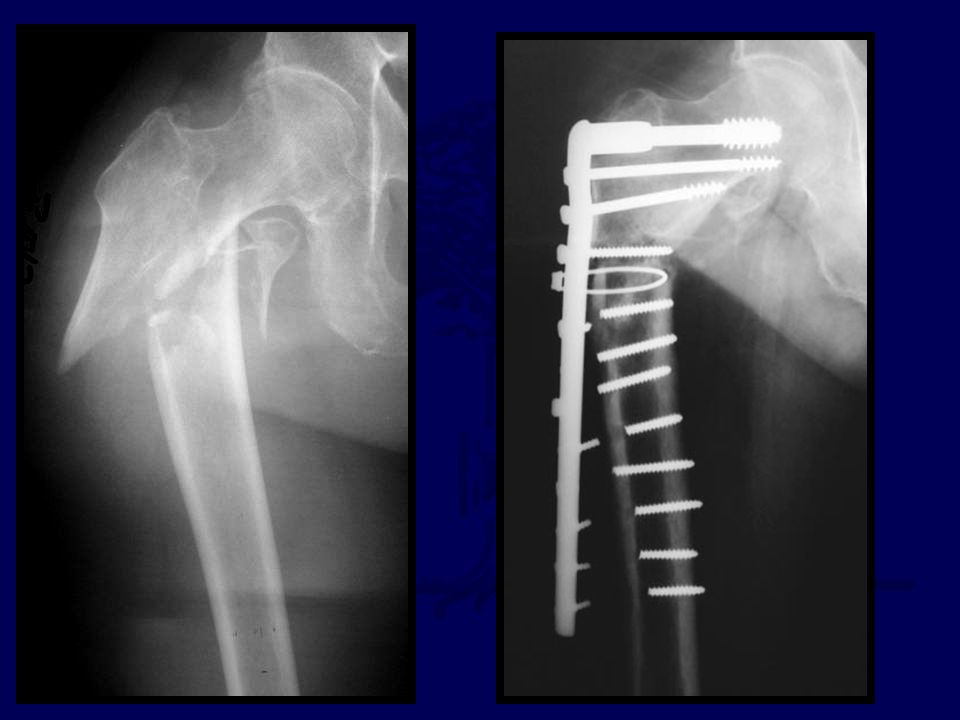
83 yo white woman with unstable intertrochanteric fracture: Note the marked loss of trabeculae Uncontrolled factor: Bone quality

15
Implants must be placed where the remaining trabeculae reside!

16
Can / Should we strengthen the bone- implant interface? PMMA 12 to 37% increase load to failure Choueka, Koval et al., ActaOrthop ‘ 96 CPPC 15% increased yield strength, stiffer Moore, Goldstein, et al., JOT ‘ 97 Elder, Goulet, et al., JOT ‘ 00 Clinical Factors in 2007 influence use delivery, cost, complications must be considered PMMA 12 to 37% increase load to failure Choueka, Koval et al., ActaOrthop ‘ 96 CPPC 15% increased yield strength, stiffer Moore, Goldstein, et al., JOT ‘ 97 Elder, Goulet, et al., JOT ‘ 00 Clinical Factors in 2007 influence use delivery, cost, complications must be considered Hydroxy-apatite (HA) coated screws Reduced cut out in poorly positioned fixation Moroni, et al. CORR ‘ 04 Hydroxy-apatite (HA) coated screws Reduced cut out in poorly positioned fixation Moroni, et al. CORR ‘ 04 Uncontrolled factor: Bone quality
 coated screws Reduced cut out in poorly positioned fixation Moroni, et al. CORR ‘ 04 Hydroxy-apatite (HA) coated screws Reduced cut out in poorly positioned fixation Moroni, et al. CORR ‘ 04 Uncontrolled factor: Bone quality.")
17
Kauffer, CORR 1980 Uncontrolled factors l Fracture Geometry l Bone Quality Surgeon controlled factors l Quality of Reduction l Implant Placement l Implant Selection Uncontrolled factors l Fracture Geometry l Bone Quality Surgeon controlled factors l Quality of Reduction l Implant Placement l Implant Selection Kaufer, CORR ‘80 Factors Influencing Construct Strength: Need to get these right!!

18
Fracture Reduction No role for displacement osteotomy Limited role for reduction & fixation of trochanteric fragments (biology vs stability) Surgical goal: Biplanar, anatomic alignment of proximal & shaft fragments Mild valgus reduction for instability to offset shortening No role for displacement osteotomy Limited role for reduction & fixation of trochanteric fragments (biology vs stability) Surgical goal: Biplanar, anatomic alignment of proximal & shaft fragments Mild valgus reduction for instability to offset shortening When employing sliding hip screws… RCT Gargan, et al. JBJS (B) ‘94 RCT Desjardins, et al. JBJS (B) ‘93 Surgeon controlled factor
 ‘94 RCT Desjardins, et al. JBJS (B) ‘93 Surgeon controlled factor.")
19
Fracture Reduction Discuss sequence of reduction steps Consider adjuncts to fracture reduction Joystick Elevator Crutch etc. PEARL : look for soon to be published article in JOT on the role of exploiting the anteriormedial cortex in stable, bone on bone reduction for fractures with “sag” deformity seen on lateral! Discuss sequence of reduction steps Consider adjuncts to fracture reduction Joystick Elevator Crutch etc. PEARL : look for soon to be published article in JOT on the role of exploiting the anteriormedial cortex in stable, bone on bone reduction for fractures with “sag” deformity seen on lateral! Surgeon controlled factor

20
Apex of the femoral head Defined as the point where a line parallel to, and in the middle of the femoral neck intersects the joint Surgeon controlled factor: Implant position

21
Screw Position: TAD Tip-Apex Distance = X ap + X lat Tip-Apex Distance = X ap + X lat X X X ap X Surgeon controlled factor: Implant position

22
Baumgaertner, Curtin, Lindskog, Keggi JBJS (A) ‘95
 ‘95")
23
Probability of Cut Out Increasing TAD -> Risk of Cut Out Baumgaertner, Curtin, Lindskog, Keggi JBJS (A) ‘95 Surgeon controlled factor: Implant position
 ‘95 Surgeon controlled factor: Implant position")
24
Logistic Regression Analysis Multivariate (dependent variable:Cut Out) l Reduction Quality p = 0.6 l Screw Zone p = 0.6 l Unstable Fracture p = 0.03 l Increasing Age p = 0.002 l Increasing TAD p = 0.0002 Multivariate (dependent variable:Cut Out) l Reduction Quality p = 0.6 l Screw Zone p = 0.6 l Unstable Fracture p = 0.03 l Increasing Age p = 0.002 l Increasing TAD p = 0.0002 Baumgaertner, Curtin, Lindskog, Keggi JBJS (A) ‘95 Surgeon controlled factor: Implant position
 l Reduction Quality p = 0.6 l Screw Zone p = 0.6 l Unstable Fracture p = 0.03 l Increasing Age p = l Increasing TAD p = Multivariate (dependent variable:Cut Out) l Reduction Quality p = 0.6 l Screw Zone p = 0.6 l Unstable Fracture p = 0.03 l Increasing Age p = l Increasing TAD p = Baumgaertner, Curtin, Lindskog, Keggi JBJS (A) ‘95 Surgeon controlled factor: Implant position")
25
Dead Center and Very Deep (TAD<25mm) Dead Center and Very Deep (TAD<25mm) l Best bone l No moment arm for rotational instability l Maximum slide l Validates reduction l Best bone l No moment arm for rotational instability l Maximum slide l Validates reduction Optimal Screw Placement Surgeon controlled factor: Implant position
 Dead Center and Very Deep (TAD<25mm) l Best bone l No moment arm for rotational instability l Maximum slide l Validates reduction l Best bone l No moment arm for rotational instability l Maximum slide l Validates reduction Optimal Screw Placement Surgeon controlled factor: Implant position")
26
What ’ s the big deal? IM vs Plate Fixation Surgeon controlled factor: Implant selection

27
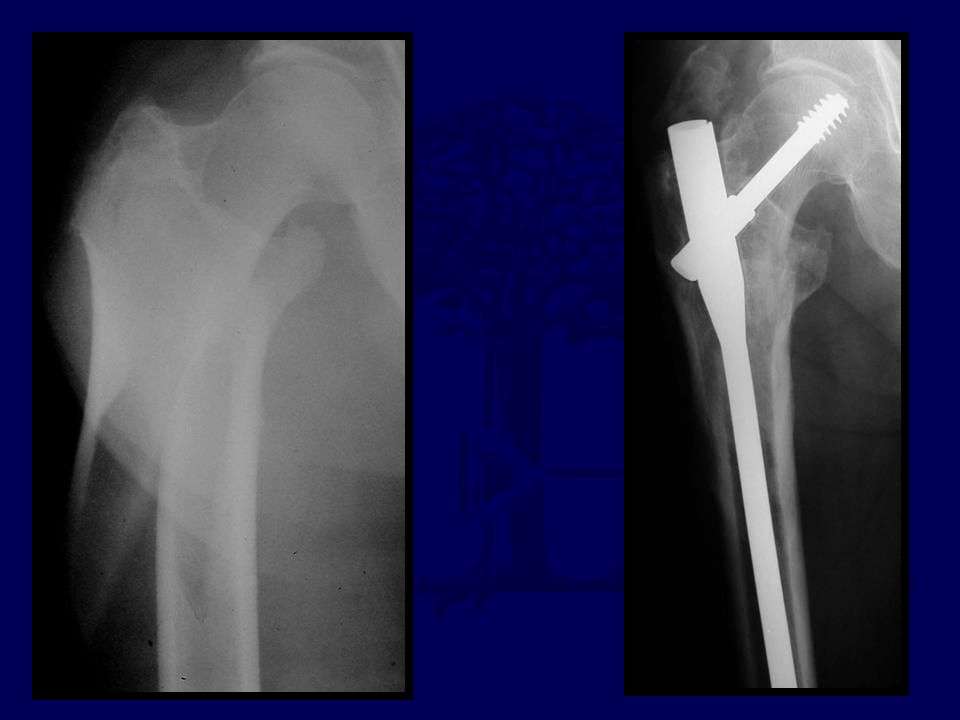
Percutaneous Procedure EBL, Muscle stripping, Complications, Rehab time Percutaneous Procedure EBL, Muscle stripping, Complications, Rehab time IM Fixation: Theoretical Biologic Advantages IM Fixation: Theoretical Biologic Advantages Surgical wounds s/p ORIF with IMHS

28
GAMMA The First to Reach the Market

29
Gamma Clinical Results Complications : +++ Advantages : Advantages : ± Complications : +++ Bridle JBJS(B) '91 Boriani Orthopaedics '91 Lindsey Trauma '91 Halder JBJS(B) '92 Bridle JBJS(B) '91 Boriani Orthopaedics '91 Lindsey Trauma '91 Halder JBJS(B) '92 Williams Injury '92 Leung JBJS(B) '92 Aune ActOrthopScan '94 Williams Injury '92 Leung JBJS(B) '92 Aune ActOrthopScan '94
 91 Boriani Orthopaedics 91 Lindsey Trauma 91 Halder JBJS(B) 92 Bridle JBJS(B) 91 Boriani Orthopaedics 91 Lindsey Trauma 91 Halder JBJS(B) 92 Williams Injury 92 Leung JBJS(B) 92 Aune ActOrthopScan 94 Williams Injury 92 Leung JBJS(B) 92 Aune ActOrthopScan 94")
30
Gamma Nail vs. CHS 1996 trials 1996 Meta-analysis of ten randomized trials x CHS (p < 0.001) Required Re-ops: Gamma 2 x CHS (p < 0.01) IM fixation may be superior for inter/subtroch extension & reverse obliquity fractures “ CHS is a forgiving implant when used by inexperienced surgeons, the Gamma nail is not” Shaft fractures: Gamma 3 x CHS (p < 0.001) Required Re-ops: Gamma 2 x CHS (p < 0.01) IM fixation may be superior for inter/subtroch extension & reverse obliquity fractures “ CHS is a forgiving implant when used by inexperienced surgeons, the Gamma nail is not” Parker, International Orthopaedics '96 MJParker, International Orthopaedics '96 Surgeon controlled factor: Implant selection
 Required Re-ops: Gamma 2 x CHS (p < 0.01) IM fixation may be superior for inter/subtroch extension & reverse obliquity fractures CHS is a forgiving implant when used by inexperienced surgeons, the Gamma nail is not Shaft fractures: Gamma 3 x CHS (p < 0.001) Required Re-ops: Gamma 2 x CHS (p < 0.01) IM fixation may be superior for inter/subtroch extension & reverse obliquity fractures CHS is a forgiving implant when used by inexperienced surgeons, the Gamma nail is not Parker, International Orthopaedics 96 MJParker, International Orthopaedics 96 Surgeon controlled factor: Implant selection.")
31
IM Fixation: Clinical Results RCT, IMHS vs CHS, N = 135 Baumgaertner, Curtin, Lindskog, CORR ‘98 No difference for stable fxs Faster & less bloody for unstable fxs Fewer IM complications than Gamma Weaknesses: No stratification of unstable fractures Learning curve issues No anatomic outcomes, wide functional outcomes No difference for stable fxs Faster & less bloody for unstable fxs Fewer IM complications than Gamma Weaknesses: No stratification of unstable fractures Learning curve issues No anatomic outcomes, wide functional outcomes Surgeon controlled factor: Implant selection

32
IM Fixation: Clinical Results Longer surgery, less blood loss Improved post-op mobility @ 1 & 3 months * Improved community ambulation @ 6 & 12 months * 45% less sliding, LLD* Longer surgery, less blood loss Improved post-op mobility @ 1 & 3 months * Improved community ambulation @ 6 & 12 months * 45% less sliding, LLD* Well analyzed RCT, IMHS vs CHS, N = 100 ( * p < 0.05) Hardy, et. al JBJS(A) ‘98 Surgeon controlled factor: Implant selection
 ‘98 Surgeon controlled factor: Implant selection.")
33
IM Fixation: Mechanical Advantages ? ? ! ! Surgeon controlled factor: Implant selection

34
Key point It is not the reduced lever arm that offers the clinically significant mechanical advantage, but rather the intramedullary buttress that the nail provides to resist excessive fracture collapse

35
The nail substitutes for the incompetent posteromedial cortex

36
31.A33 2 weeks 7 months The nail substitutes for the incompetent lateral cortex

37
IM Fixation: Selected Clinical Results 5° in neck shaft angle @ 6 wks (all) shaft medialization @ 4mo * 5° in neck shaft angle @ 6 wks (all) shaft medialization @ 4mo * RCT, IMscrew vs CHS, N = 46 (* p < 0.05) Pajarinen, Int Orth ‘04 Improved post-op mobility (4 months)* less sliding, shaft medialization* Improved post-op mobility (4 months)* less sliding, shaft medialization* RCT, IMscrew vs CHS, N = 108 Pajarinen, JBJS(B) ‘05 RCT, IMscrew vs CHS, N = 436 Ahrengart, CORR ‘02 less sliding, shaft medialization* Surgeon controlled factor: Implant selection
 shaft 4mo * 5° in neck shaft 6 wks (all) shaft 4mo * RCT, IMscrew vs CHS, N = 46 (* p < 0.05) Pajarinen, Int Orth ‘04 Improved post-op mobility (4 months)* less sliding, shaft medialization* Improved post-op mobility (4 months)* less sliding, shaft medialization* RCT, IMscrew vs CHS, N = 108 Pajarinen, JBJS(B) ‘05 RCT, IMscrew vs CHS, N = 436 Ahrengart, CORR ‘02 less sliding, shaft medialization* Surgeon controlled factor: Implant selection")
38
Trochanteric Stabilizing Plate plate adjunct to limit shaft medialization major (≥20mm screw slide) collapse op time, blood loss ? complications, length of rehab major (≥20mm screw slide) collapse op time, blood loss ? complications, length of rehab Madsen, JOT '98 Madsen, JOT '98 Su, Trauma ‘03 Su, Trauma ‘03 Bong, Trauma ‘04 CHS Improvements: 1975-2006 Surgeon controlled factor: Implant selection
 collapse op time, blood loss . complications, length of rehab Madsen, JOT 98 Madsen, JOT 98 Su, Trauma ‘03 Su, Trauma ‘03 Bong, Trauma ‘04 CHS Improvements: Surgeon controlled factor: Implant selection.")
39
Bi-axial Sliding Hip Screw Biomechanical 50% medial cortical load Olsson, ActaOrthop Scan ‘87 Clinical mechanical failure op-time & blood loss complications Medoff, JBJS(A) ‘91 Lunsjö, JBJS(B) ‘96 Watson, CORR ‘98 Biomechanical 50% medial cortical load Olsson, ActaOrthop Scan ‘87 Clinical mechanical failure op-time & blood loss complications Medoff, JBJS(A) ‘91 Lunsjö, JBJS(B) ‘96 Watson, CORR ‘98 CHS Improvements: 1975-2006 Surgeon controlled factor: Implant selection
 ‘91 Lunsjö, JBJS(B) ‘96 Watson, CORR ‘98 Biomechanical 50% medial cortical load Olsson, ActaOrthop Scan ‘87 Clinical mechanical failure op-time & blood loss complications Medoff, JBJS(A) ‘91 Lunsjö, JBJS(B) ‘96 Watson, CORR ‘98 CHS Improvements: Surgeon controlled factor: Implant selection")
40
Reverse Oblique Fractures IM Fixation: Best Indications Surgeon controlled factor: Implant selection Intertroch + subtrochanteric fractures

41
Haidukewych, JBJS(A) 2001 Retrospective review of 49 consecutive R/ob. fractures @ Mayo: overall 30% failure rate Poor Implant Position:80% failure Implant Type: Compression Hip Screw:56% failure (9/16) 95° blade / DCS: 20% failure (5/25) IMHipScrew:0% failure (0/3) Retrospective review of 49 consecutive R/ob. fractures @ Mayo: overall 30% failure rate Poor Implant Position:80% failure Implant Type: Compression Hip Screw:56% failure (9/16) 95° blade / DCS: 20% failure (5/25) IMHipScrew:0% failure (0/3) Reverse Oblique Fractures Surgeon controlled factor: Implant selection
 95° blade / DCS: 20% failure (5/25) IMHipScrew:0% failure (0/3) Retrospective review of 49 consecutive R/ob. Mayo: overall 30% failure rate Poor Implant Position:80% failure Implant Type: Compression Hip Screw:56% failure (9/16) 95° blade / DCS: 20% failure (5/25) IMHipScrew:0% failure (0/3) Reverse Oblique Fractures Surgeon controlled factor: Implant selection.")
43
PFN vs 95° sliding screw plate(DCS) RCT of 39 cases done by Swiss AO surgeons PFN (IM) vs Plate Open reductions Op-time Blood tx Failure rate Major reoperations PFN vs 95° sliding screw plate(DCS) RCT of 39 cases done by Swiss AO surgeons PFN (IM) vs Plate Open reductions Op-time Blood tx Failure rate Major reoperations All Significantly reduced! Sadowski,Hoffmeyer JBJS(A) 2002 Reverse Oblique Fractures Surgeon controlled factor: Implant selection
 2002 Reverse Oblique Fractures Surgeon controlled factor: Implant selection.")
44
Recovery room control X-ray shows loss of medial support, but nail prevents excessive collapse

46
Intertroch/ subtrochanteric fxs Greater mechanical demands, poorer fracture healing Surgeon controlled factor: Implant selection

48
Long Gamma Nail for IT-ST Fxs Barquet, JOT 2000 52 consecutive fractures; 43 with 1 year f/u l 100% union l 81 minutes, 370cc EBL The authors describe the key percutaneous reduction techniques that lead to successful management of these difficult fractures Barquet, JOT 2000 52 consecutive fractures; 43 with 1 year f/u l 100% union l 81 minutes, 370cc EBL The authors describe the key percutaneous reduction techniques that lead to successful management of these difficult fractures Surgeon controlled factor: Implant selection

49
Reduction Aids

50
Unstable Pertroch Fractures (OTA31A.3) “Evidence-based bottom line:” Unacceptable failure rates with CHS Better results with 95° devices Best results with I M devices* Best “functional outcome” not known “Evidence-based bottom line:” Unacceptable failure rates with CHS Better results with 95° devices Best results with I M devices* Best “functional outcome” not known Kregor, et al (Evidence Based Working Group) JOT ‘05 347 articles reviewed: 10 relevant; 5 RCTs* Surgeon controlled factor: Implant selection
 Evidence-based bottom line: Unacceptable failure rates with CHS Better results with 95° devices Best results with I M devices* Best functional outcome not known Evidence-based bottom line: Unacceptable failure rates with CHS Better results with 95° devices Best results with I M devices* Best functional outcome not known Kregor, et al (Evidence Based Working Group) JOT ‘ articles reviewed: 10 relevant; 5 RCTs* Surgeon controlled factor: Implant selection")
51
AO / OTA 31 CHS

52
Grossly displaced Stable (31A.1) fracture treated with ORIF Surgeon controlled factor: Implant selection
 fracture treated with ORIF Surgeon controlled factor: Implant selection")
53
There is no data to support nailing over sideplate fixation for A1 fractures Surgeon controlled factor: Implant selection

54
AO / OTA 31 CHS NAIL ????

55
IM Fixation (TGN) vs. CHS Randomized/prospective trial of 210 pts. Utrilla, et al. JOT 4/05 Patients l All ambulatory, no ASA Vs Fractures l Excluded inter/subtrochs fractures (31A.3) Surgeons l Only 4, all experienced (excluded first 3 TGNs) Technique l All got spinals, Closed reduction, percutaneous fixation l All overreamed 2mm, all got 130° x 11mm nail, one distal interlock prn rotational instability (rarely used) Patients l All ambulatory, no ASA Vs Fractures l Excluded inter/subtrochs fractures (31A.3) Surgeons l Only 4, all experienced (excluded first 3 TGNs) Technique l All got spinals, Closed reduction, percutaneous fixation l All overreamed 2mm, all got 130° x 11mm nail, one distal interlock prn rotational instability (rarely used) Surgeon controlled factor: Implant selection
 Surgeons l Only 4, all experienced (excluded first 3 TGNs) Technique l All got spinals, Closed reduction, percutaneous fixation l All overreamed 2mm, all got 130° x 11mm nail, one distal interlock prn rotational instability (rarely used) Patients l All ambulatory, no ASA Vs Fractures l Excluded inter/subtrochs fractures (31A.3) Surgeons l Only 4, all experienced (excluded first 3 TGNs) Technique l All got spinals, Closed reduction, percutaneous fixation l All overreamed 2mm, all got 130° x 11mm nail, one distal interlock prn rotational instability (rarely used) Surgeon controlled factor: Implant selection.")
56
Results Skin to skin time unchanged Fewer blood transfusions needed Better walking ability in Unstable fractures with IM No shaft fxs Fewer re-ops needed in IM group (1 vs 4) Conclusion IM fixation or CHS for stable fxs Unlocked TGN for most Unstable fxs Results Skin to skin time unchanged Fewer blood transfusions needed Better walking ability in Unstable fractures with IM No shaft fxs Fewer re-ops needed in IM group (1 vs 4) Conclusion IM fixation or CHS for stable fxs Unlocked TGN for most Unstable fxs IM Fixation (TGN) vs. CHS Randomized/prospective trial of 210 pts. Utrilla, et al. JOT 4/05 Surgeon controlled factor: Implant selection

57
IM Hip Screws Author’s Take Increasing data to support use for unstable fracture patterns Improved anatomy and early function Iatrogenic problems decreasing with current designs and technique Indicated only for the geriatric fracture Increasing data to support use for unstable fracture patterns Improved anatomy and early function Iatrogenic problems decreasing with current designs and technique Indicated only for the geriatric fracture Surgeon controlled factor: Implant selection

58
IM Hip Screw: Contraindications young patients (excess bone removal) basal neck fxs (iatrogenic displacement) stable fractures requiring open reduction (inefficient) stable fractures with very narrow canals (inefficient) young patients (excess bone removal) basal neck fxs (iatrogenic displacement) stable fractures requiring open reduction (inefficient) stable fractures with very narrow canals (inefficient) Surgeon controlled factor: Implant selection
 basal neck fxs (iatrogenic displacement) stable fractures requiring open reduction (inefficient) stable fractures with very narrow canals (inefficient) young patients (excess bone removal) basal neck fxs (iatrogenic displacement) stable fractures requiring open reduction (inefficient) stable fractures with very narrow canals (inefficient) Surgeon controlled factor: Implant selection")
59
Technical Tips

60
Patient Set-up Position for nailing: l Hip Adducted l Unobstructed AP & lateral imaging l Fracture Reduced(?) Position for nailing: l Hip Adducted l Unobstructed AP & lateral imaging l Fracture Reduced(?) Strong traction (without well leg countertraction) abducts fractured hip and prevents gaining proper entrance site
 Position for nailing: l Hip Adducted l Unobstructed AP & lateral imaging l Fracture Reduced( ) Strong traction (without well leg countertraction) abducts fractured hip and prevents gaining proper entrance site")
62
Both feet in txnBoth feet in txn Fx: flexed & addFx: flexed & add Well leg extended & abductedWell leg extended & abducted Lateral Xray: a little different, but adequate Lateral Xray: a little different, but adequate The solution is the “Scissors position” for the extremities

63
Guide Pin Insertion

64
(Usually by hand…) Guide Pin Insertion Ostrum, JOT 05: The entrance is at the trochanteric tip or slightly MEDIAL
 Guide Pin Insertion Ostrum, JOT 05: The entrance is at the trochanteric tip or slightly MEDIAL")
65
Ream a channel for implant! (don’t just displace the fracture as you pass reamer through it) Medial directed force prevents fracture gapping during entrance reaming
 Medial directed force prevents fracture gapping during entrance reaming.")
66
Achieve a Neck-Shaft Axis > 130° Use at least a 130° nail Varus Corrections Advance nail Increase traction ABDUCT extremity!! (adduction only necessary at time of nail insertion) Use at least a 130° nail Varus Corrections Advance nail Increase traction ABDUCT extremity!! (adduction only necessary at time of nail insertion)
 Use at least a 130° nail Varus Corrections Advance nail Increase traction ABDUCT extremity!. (adduction only necessary at time of nail insertion).")
67
Allow all patients to WBAT Patients “self regulate” force on hip No increased rate of failure X-rays post-op, then 6 & 12 weeks Allow all patients to WBAT Patients “self regulate” force on hip No increased rate of failure X-rays post-op, then 6 & 12 weeks Postoperative Management Koval, et. al,JBJS(A)’98
’98.")
68
Where’s the evidence?? Unanswered questions

69
Minimally invasive PLATE fixation ?? 2 hole DHS Bolhofner Dipaola PCCP Gotfried 2 hole DHS Bolhofner Dipaola PCCP Gotfried

70
Which nail design is best ?? Proximal diameter? Nail Length? Distal interlocking? Proximal screw ? Sleeve or no sleeve? Loch & Kyle, JBJS(A)‘98 One or two needed ? ? Nobody knows!
‘98 One or two needed . Nobody knows!.")
71
Proximal fixation: 1 or 2 screws? Kubiak, JOT ‘04 IMHS vs Trigen in vitro (cadaveric) testing Results: No difference in fx sliding or collapse No difference in rigidity or stability Trigen with higher ultimate strength @ failure Clinical significance?? IMHS vs Trigen in vitro (cadaveric) testing Results: No difference in fx sliding or collapse No difference in rigidity or stability Trigen with higher ultimate strength @ failure Clinical significance?? Nobody knows!
 testing Results: No difference in fx sliding or collapse No difference in rigidity or stability Trigen with higher ultimate failure Clinical significance . IMHS vs Trigen in vitro (cadaveric) testing Results: No difference in fx sliding or collapse No difference in rigidity or stability Trigen with higher ultimate failure Clinical significance . Nobody knows!.")
72
Small Screws protect lateral wall Only relevant for plate fixation? Gotfried, CORR ‘04 Im, JOT ‘05

73
But… the “Z effect” 7/70, 10% Werner-Tutschku, Unfall ’02 5/45 11% Tyllianakis Acta Orthop Belgica ‘04 Small Screws protect lateral wall Only relevant for plate fixation? Gotfried, CORR ‘04 Im, JOT ‘05

74
Thigh pain from short, locked nails? Periprosthetic fracture: Still an issue? Anterior cortex perforation with long nails? Cost/ benefit? -Nobody knows- 6% impinge/ 2% fx Robinson, JBJS(A) 05 Long vs.short nails?
 05 Long vs.short nails .")
75
Just when you think you know whats best- - Don’t forget Ex-Fix! RCT n=40 Exfix +HA vs DHS Faster ops, fewer txfusions, no comps Moroni, et al. JBJS(A) 4/05 ?
 4/05 .")
76
Ex-fix (HApins) vs DHS Randomized/prospective trial of 40 pts. Moroni, et al. JBJS(A) 4/05 Patients l 65yo+ walking women with osteoporosis Results l Faster operations with Fewer transfusions l Less post op pain, similar final function l No pin site infxs, no increased post op care l Increased pin torque on removal @ 12 wks l One nonunion Patients l 65yo+ walking women with osteoporosis Results l Faster operations with Fewer transfusions l Less post op pain, similar final function l No pin site infxs, no increased post op care l Increased pin torque on removal @ 12 wks l One nonunion
 4/05 Patients l 65yo+ walking women with osteoporosis Results l Faster operations with Fewer transfusions l Less post op pain, similar final function l No pin site infxs, no increased post op care l Increased pin torque on 12 wks l One nonunion Patients l 65yo+ walking women with osteoporosis Results l Faster operations with Fewer transfusions l Less post op pain, similar final function l No pin site infxs, no increased post op care l Increased pin torque on 12 wks l One nonunion.")
77
Conclusions: Remember Kaufer’s Variables Uncontrolled factors Fracture Geometry Bone Quality Surgeon controlled factors Quality of Reduction Implant Placement Implant Selection Uncontrolled factors Fracture Geometry Bone Quality Surgeon controlled factors Quality of Reduction Implant Placement Implant Selection

78
Position screw centrally and very deep (TAD≤20mm) Implants have different traits-choose wisely Conclusions:
 Implants have different traits-choose wisely Conclusions:")
79
Things change Conclusions: Healing is no longer “success” Deformity & function matter Perioperative insult counts Healing is no longer “success” Deformity & function matter Perioperative insult counts

81
Audience Response Questions! (save 5-8 minutes for these)
")
82
81 y.o. female slipped & fell 3 part IT fx Post-op X-rays Discuss: Did the surgeon do a good job? Did the surgeon do a good job? Yes or No

83
Did the surgeon do a good job? Yes No Yes No Answer before advancing.

84
A.The reduction is satisfactory B. The TAD (screw position) is OK C. Both are satisfactory D. Neither are satisfactory …Choose Best Answer Now, consider specifically:

85
3months 6 months

86
Post op

87
The TAD was acceptable but the reduction was grossly short

88
Did the surgeon do a good job? Yes No Yes No

90
27yo jogger struck by car, closed, isolated injury

91
27yo jogger struck by car I’d reduce & fix with: A. 95° blade B. DCS plate C. “Recon” Nail D. DHS E. Intramedullary hip screw (PFN, TFN, IMHS, GAMMA)
.")
93
A.The reduction is satisfactory B. The TAD is satisfactory C. Both are satisfactory D. Neither are satisfactory

94
* *

95
Progressive pain 11-14 weeks (varus + plate is rarely good)
")
96
I’d Bonegraft & revise with: A. 95° blade B. DCS plate C. “Recon” Nail D. DHS E. IMHS F Other

97
95° DCS + autoBG

98
71 yo renal txplnt pt c CHF What to do??

99
If my patient, I would use: 1. Hip screw and sideplate 2. Hip screw and IM nail (TFN) 3. Reconstruction Nail (2 proximal medullary-cephalic screws) 4. Blade Plate 5. Other 1. Hip screw and sideplate 2. Hip screw and IM nail (TFN) 3. Reconstruction Nail (2 proximal medullary-cephalic screws) 4. Blade Plate 5. Other
 3. Reconstruction Nail (2 proximal medullary-cephalic screws) 4. Blade Plate 5. Other 1. Hip screw and sideplate 2. Hip screw and IM nail (TFN) 3. Reconstruction Nail (2 proximal medullary-cephalic screws) 4. Blade Plate 5. Other.")
100
percutaneous reduction

101
Uneventful Healing, WBAT 6wks12wks

102
Return to Lower Extremity Index E-mail OTA about Questions/Comments If you would like to volunteer as an author for the Resident Slide Project or recommend updates to any of the following slides, please send an e-mail to ota@aaos.orgota@aaos.org

Similar presentations




 ARTHROPLASTY –In biologic ‘old’ patients (> 60-80 yr)>")


















