Download presentation
Presentation is loading. Please wait.

1
Brady Arrhythmia M.R Samieinasab, MD,
Interventional Electrophysiologist Chamran Heart Hospital

2
Definition: HR slower than 60/min

3
Normal Impulse Conduction
Sinoatrial node AV node Bundle of His Bundle Branches Purkinje fibers

4
Symptom Basis Bradycardia /asystole cardiac output perfusion
Symptoms AV dyssnchrony venous pressures ‘Pacemaker Syndrome’ Symptoms Bradycardia Symptoms: Symptoms of bradycardia usually occur when the heart is not pumping enough blood to meet the body's needs. This often happens when the heart rate is very slow or remains slow for a long period of time. Symptoms related to organ hypo-perfusion include: Dizziness or lightheadedness • Fainting (syncope) or near-fainting Tiredness (fatigue) • Shortness of breath Palpitations • Chest pain (angina) Increased difficulty exercising • Confusion or difficulty concentrating Some people with bradycardia do not have symptoms AV dyssynchrony symptoms: When the cause of bradycardia is a conduction block there might also be a loss of physiologic timing of atrial and ventricular contractions, or AV dyssynchrony: Loss of atrial kick Cannon a waves: Atrial contraction against a closed AV valve can cause pulsation in the neck and abdomen, headache, cough, and jaw pain. Increased atrial pressure: Ventricular pacing is associated with elevated right and left atrial pressures, as well as elevated pulmonary venous and pulmonary arterial pressures, which can lead to symptomatic pulmonary and hepatic congestion.
 or near-fainting. Tiredness (fatigue) • Shortness of breath. Palpitations • Chest pain (angina) Increased difficulty exercising • Confusion or difficulty concentrating. Some people with bradycardia do not have symptoms. AV dyssynchrony symptoms: When the cause of bradycardia is a conduction block there might also be a loss of physiologic timing of atrial and ventricular contractions, or AV dyssynchrony: Loss of atrial kick. Cannon a waves: Atrial contraction against a closed AV valve can cause pulsation in the neck and abdomen, headache, cough, and jaw pain. Increased atrial pressure: Ventricular pacing is associated with elevated right and left atrial pressures, as well as elevated pulmonary venous and pulmonary arterial pressures, which can lead to symptomatic pulmonary and hepatic congestion.")
5
Symptoms of Bradycardia
Usually occurs when heart is not pumping enough blood to meet body's needs. This often happens when the heart rate is very slow or remains slow for a long period of time. Related to organ hypo-perfusion and include: Dizziness or lightheadedness Fainting (syncope) or near-fainting Tiredness (fatigue) Shortness of breath Palpitations Chest pain (angina) Increased difficulty exercising Confusion or difficulty concentrating Some people with bradycardia do not have symptoms Yan, Gan-Xin (2011). Management of Cardiac Arrhythmias. New York: Springer Science. pg. 307.
 or near-fainting. Tiredness (fatigue) Shortness of breath. Palpitations. Chest pain (angina) Increased difficulty exercising. Confusion or difficulty concentrating. Some people with bradycardia do not have symptoms. Yan, Gan-Xin (2011). Management of Cardiac Arrhythmias. New York: Springer Science. pg")
6
Classifications of Bradyarrhythmias
There are two types of bradyarrhythmias Those related to problems with impulse formation Those related to problems with impulse conduction Sinus node AV node

7
Classification of Bradyarrhythmias
Problems with Impulse Formation Sinus Arrest Sinus Bradycardia Chronotropic Incompetence Brady/Tachy syndrome

8
Practice Rhythm Strips
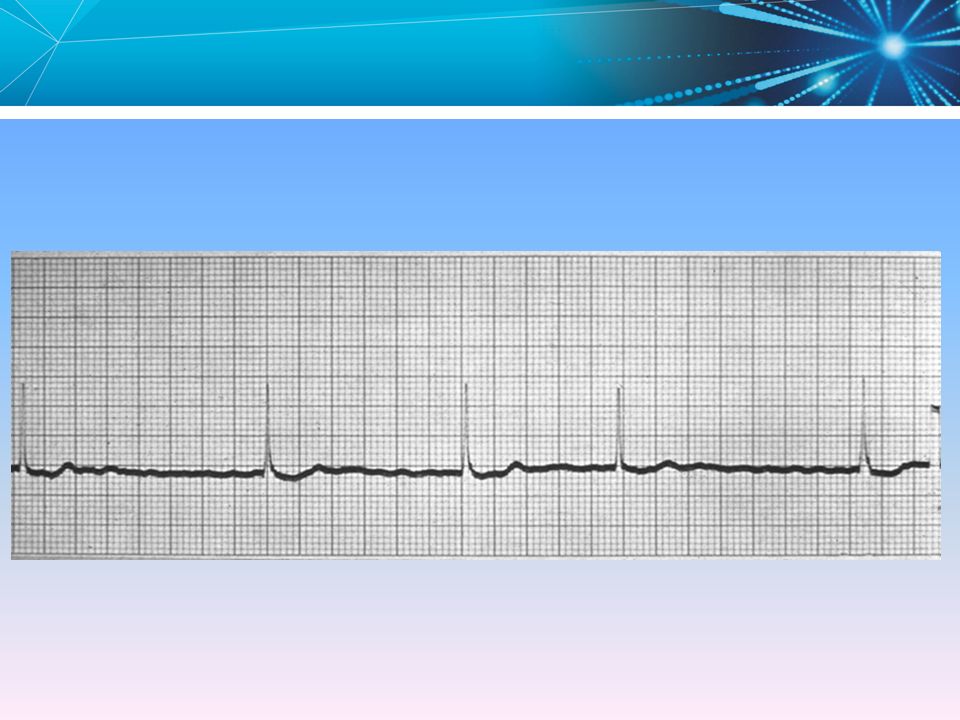
Sinus Bradycardia

9
Sinus Bradycardia Sinus Node depolarizes very slowly
If the patient is symptomatic and the rhythm is persistent and irreversible, may require a pacemaker Sinus bradycardia occurs when the SA node fires at an abnormally slow rate (< 60 bpm).
.")
10
Sinus Bradycardia Causes
Hypothyroidism Drugs During vomiting or vasovagal syncope Increased intracranial pressure Hypoxia, hypothermia Infections Depression Jaundice

11
Practice Rhythm Strips
Sinus Arrest

12
Sinus Pause/Arrest Rate Varies P-P Regularity Irregular R-R Regularity
P wave Present, except during pause P:QRS Ratio 1:1, associated PR Interval Normal QRS Width

13
Sinus Node Exit Block Rate Varies P-P Regularity Irregular
R-R Regularity P wave Present, except during dropped beats P:QRS Ratio 1:1, associated PR Interval Normal QRS Width

14
None, or Regular if antegrade or retrograde R-R Regularity Regular
Rate 40-60bpm P-P Regularity None, or Regular if antegrade or retrograde R-R Regularity Regular P wave Variable (none, antegrade, or retrograde) P:QRS Ratio None, or 1:1 if antegrade or retrograde PR Interval None, short, or retrograde QRS Width Normal 14
 P:QRS Ratio. None, or 1:1 if antegrade or retrograde. PR Interval. None, short, or retrograde. QRS Width. Normal. 14.")
15
Rate? 50-75 bpm Regularity? Phasic variations P waves? normal PR interval? 0.12 s QRS duration? 0.10 s Interpretation? Sinus Arrhythmia

16
Sinus Arrest Failure of sinus node discharge
Absence of atrial depolarization Periods of ventricular asystole May be episodic as in vaso-vagal syncope, or carotid sinus hypersensitivity May require a pacemaker Sinus arrest occurs when there is a pause in the rate at which the SA node fires. With sinus arrest there is no relationship between the pause and the basic cycle length.

17
Chronotropic Incompetence
The heart rate is unable to change in response to the body’s metabolic demand. Griffen, Brian P. (2011). Manual of Cardiovascular Medicine. Philadelphia: Lippincott, Williams, and Wilkins. (pg. 79).
. Manual of Cardiovascular Medicine. Philadelphia: Lippincott, Williams, and Wilkins. (pg. 79).")
18
Normal, healthy heart is able to increase peak cardiac output by up to 5x baseline with exercise
In chronotropic incompetence, patient may only be able to double cardiac output over baseline An increase in stroke volume only may limit activity and cause symptoms 60 bpm 95 bpm 130 bpm Heart Rate Activity Running [O] - Clinical Need for increases in HR [I] - Go thru the animation to describe that different rates are needed for different activities. OVERVIEW: The purpose of Rate Response is to insure that the HR increases to meet the metabolic needs of the patient during such activities as sleeping, walking and running. It is particularly important for chronotropic incompetent patients and patients that have chronic atrial fibrillation with a slow ventricular response. The pacemaker may provide appropriate rate response for patients who require cardiac pacing support at both submaximal and maximal rates. Submaximal rates are moderate pacing rates near the Activities of Daily Living Rate (ADL Rate) obtained during typical daily activities such as walking or daily chores. Maximal rates are rates (at or near the Upper Sensor Rate) obtained during vigorous activities. To achieve appropriate rate response, the pacemaker provides activity sensor-driven pacing with rate response control in both the ADL rate range and the exertion rate range. Walking Sleeping 1 Nordlander R, Hedman A, Phersson SK. Rate responsive pacing and exercise capacity—a comment. PACE. 1989;12: 2 Stone J, Crossley G. Current sensor technology for heart rate modulation by artificial pacing. Clinical Electrophysiology Review. 1999;3:10-14
 obtained during typical daily activities such as walking or daily chores. Maximal rates are rates (at or near the Upper Sensor Rate) obtained during vigorous activities. To achieve appropriate rate response, the pacemaker provides activity sensor-driven pacing with rate response control in both the ADL rate range and the exertion rate range. Walking. Sleeping. 1 Nordlander R, Hedman A, Phersson SK. Rate responsive pacing and exercise capacity—a comment. PACE. 1989;12: Stone J, Crossley G. Current sensor technology for heart rate modulation by artificial pacing. Clinical Electrophysiology Review. 1999;3:")
19
Practice Rhythm Strips
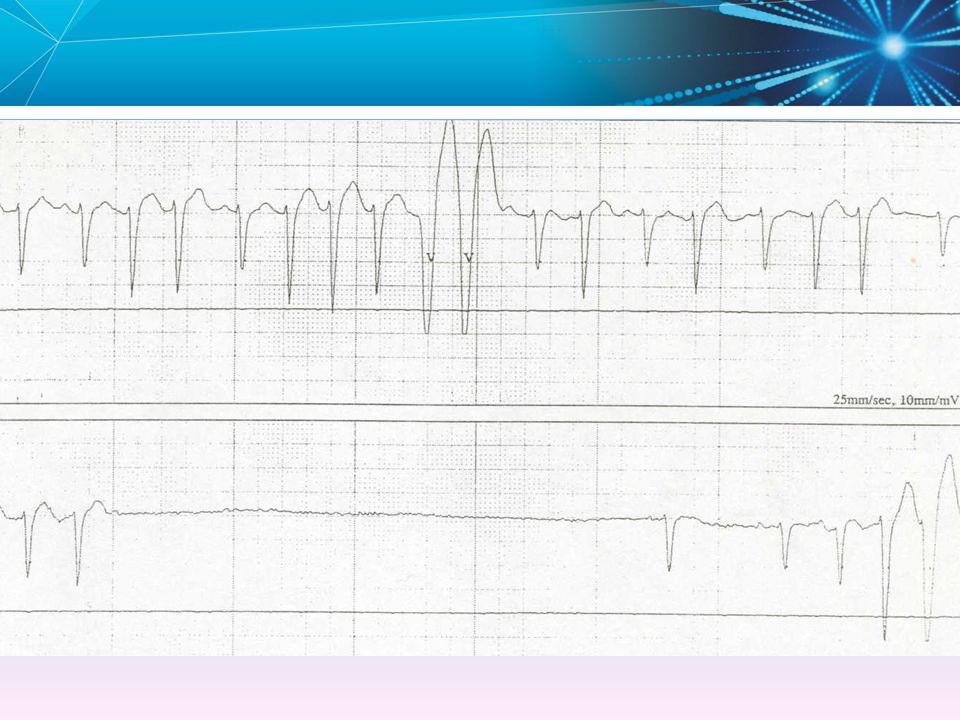
Sinus Node Dysfunction Also: Sick Sinus Syndrome, Bradycardia-tachycardia Syndrome, tachy-brady syndrome Abnormalities in sinus node activity or conduction that result in slow or irregular heart rates or intermittent tachycardia. Atrial tachycardias, most often atrial fibrillation, often are associated with sinus bradycardia or sinus arrest when they terminate. Sinus node dysfunction constitutes a spectrum of cardiac arrhythmias, including sinus bradycardia, sinus arrest, sinoatrial block, and paroxysmal supraventricular tachyarrhythmias alternating with periods of bradycardia or even asystole. Image: The initial rhythm is an atrial flutter with every second flutter wave concealed by the QRS complexes. It suddenly terminates and there is asystole that is finally interrupted by an escape junctional beat.

20
Brady/Tachy Syndrome Intermittent episodes of slow and fast rates from the SA node or atria Brady < 60 bpm Tachy > 100 bpm Sinus Node Disease Patient may also have periods of AF and chronotropic incompetence Most common pacing indication Brady-tachy syndrome occurs when the SA node has alternating periods of firing too slowly (< 60 bpm), and too fast (> 100 bpm). Brady-tachy syndrome often manifests itself in periods of atrial tachycardia, flutter, or fibrillation. Cessation of the tachycardia is often followed by long pauses from the SA node. Chronotropic incompetence—condition where the sinus node does not meet metabolic needs by increasing heart rate. Curtis, Anne B. (2011). Fundamentals of Cardiac Pacing. Massachusetts: John and Bartlett Publishers. (pg. 24).
, and too fast (> 100 bpm). Brady-tachy syndrome often manifests itself in periods of atrial tachycardia, flutter, or fibrillation. Cessation of the tachycardia is often followed by long pauses from the SA node. Chronotropic incompetence—condition where the sinus node does not meet metabolic needs by increasing heart rate. Curtis, Anne B. (2011). Fundamentals of Cardiac Pacing. Massachusetts: John and Bartlett Publishers. (pg. 24).")
21
High Vagal Tone Usually in the young
Normal heart rate response during exercise Normal intrinsic heart rate Bradycardia may be severe enough to cause syncope (especially in familial form)
")
22
Bradycardia Classifications
Problems with Impulse Conduction Exit Block First Degree AV block Second Degree AV block Mobitz Type 1 – Wenckebach Mobitz Type 2 Third Degree AV block – Complete heart block Bifasicular/Trifasicular block

23
Exit Block Transient block of impulses from the SA node
Sinus Wenckebach is possible, but rare Pacing is rare unless symptomatic, irreversible, and persistent SA exit block occurs when the SA node fires, but the impulse does not conduct to the pathways that cause the atrium to contract. In SA exit block, there is a relationship between the pattern and the basic cycle length (because the sinus node continues to fire regularly), of approximately two, but less commonly three or four times the normal P-P interval.
, of approximately two, but less commonly three or four times the normal P-P interval.")
24
Rate? 60 bpm Regularity? Regular P waves? Normal PR interval? 0.36 s QRS duration? 0.08 s Interpretation? 1st Degree AV Block

25
First-Degree AV Block PR interval > 200 ms
Delayed conduction through the AV Node Example shows PR Interval = 320 ms Not an indication for pacing Some consider this a normal variant (not an arrhythmia) AV block can be described as a prolongation of the PR interval, the interval from the onset of the P-wave to the onset of the QRS complex. First-degree AV block is defined by a PR interval greater than 0.20 seconds (200 ms). First-degree AV block can be thought of as a delay in AV conduction, but each atrial signal is conducted to the ventricles (1:1 ratio). There are some who feel First-degree AV block is not an arrhythmia but a normal variant. In any case, it is not an indication for a pacemaker.
 AV block can be described as a prolongation of the PR interval, the interval from the onset of the P-wave to the onset of the QRS complex. First-degree AV block is defined by a PR interval greater than 0.20 seconds (200 ms). First-degree AV block can be thought of as a delay in AV conduction, but each atrial signal is conducted to the ventricles (1:1 ratio). There are some who feel First-degree AV block is not an arrhythmia but a normal variant. In any case, it is not an indication for a pacemaker.")
26
Wenckebach Block

27
Second-Degree AV Block – Mobitz I
Progressive prolongation of the PR interval until there is failure to conduct and a ventricular beat is dropped Otherwise known as Wenckebach block Usually not an indication for pacing Second-degree AV block is characterized by intermittent failure of atrial depolarizations to reach the ventricle. There are two patterns of second-degree AV block. Type I is marked by progressive prolongation of the PR interval in cycles preceding a dropped beat. This is also referred to as Wenckebach or Mobitz Type I block. The AV node is most commonly the site of Mobitz I block. The QRS duration is usually normal.

29
Second-Degree AV Block – Mobitz II
Regularly dropped ventricular beats 2:1 block (2 P-waves for every 1 QRS complex) Atrial rate = 75 bpm, Ventricular rate = 42 bpm A “high grade” block, usually an indication for pacing May progress to third-degree, or Complete Heart block (CHB) Mobitz Type II second-degree AV block refers to intermittent dropped beats preceded by constant PR intervals. To differentiate Mobitz I from Mobitz II, note the PR interval in the beats preceding and following the dropped beat If a difference between these two PR intervals is more than 0.02 seconds (20 ms), then it is Mobitz I. If the difference is less than 0.02 seconds, then it is Mobitz II. The infranodal (His bundle) tissue is most commonly the site of Mobitz II block. Unlike the graphic, Mobitz II is often accompanied by a wide QRS complex. Note: Advanced second-degree block refers to the block of two or more consecutive P-waves (i.e., 3:1 block).
 Atrial rate = 75 bpm, Ventricular rate = 42 bpm. A high grade block, usually an indication for pacing. May progress to third-degree, or Complete Heart block (CHB) Mobitz Type II second-degree AV block refers to intermittent dropped beats preceded by constant PR intervals. To differentiate Mobitz I from Mobitz II, note the PR interval in the beats preceding and following the dropped beat. If a difference between these two PR intervals is more than 0.02 seconds (20 ms), then it is Mobitz I. If the difference is less than 0.02 seconds, then it is Mobitz II. The infranodal (His bundle) tissue is most commonly the site of Mobitz II block. Unlike the graphic, Mobitz II is often accompanied by a wide QRS complex. Note: Advanced second-degree block refers to the block of two or more consecutive P-waves (i.e., 3:1 block).")
30
Rate? 40 bpm Regularity? Regular P waves? Nl, 2 of 3 no QRS PR interval? 0.14 s QRS duration? 0.08 s Interpretation? Advanced AV Block

31
Third-Degree AV Block Complete Heart Block
No impulse conduction from the atria to the ventricles Atrial rate = 130 bpm, Ventricular rate = 37 bpm Complete A – V disassociation Usually a wide QRS as ventricular rate is idioventricular Third-degree AV block is also referred to as complete heart block. Characterized by a complete dissociation between P-waves and QRS complexes. The QRS complexes are not caused by conduction of the P-waves through the AV node to the ventricles. The QRS is initiated at a site below the AV node (such as in the His bundle or the Purkinje fibers). This “escape rhythm” is normally 40–60 bpm if initiated by the His bundle (a junctional rhythm) and <40 bpm if initiated by the Purkinje fibers.
. This escape rhythm is normally 40–60 bpm if initiated by the His bundle (a junctional rhythm) and <40 bpm if initiated by the Purkinje fibers.")
32
Fascicular Block Bifascicular block is when 2 (with the exception of complete left BBB) of the conduction system pathways below the AV Node are blocked. They are defined as one of the following: Right bundle branch block and left posterior hemiblock Right bundle branch block and left anterior hemiblock - marked by prolonged QRS (> 120 ms or .12 seconds or longer) Complete left bundle branch block Right bundle branch block and left posterior hemiblock Right bundle branch block and left anterior hemiblock Complete left bundle branch block
 of the conduction system pathways below the AV Node are blocked. They are defined as one of the following: Right bundle branch block and left posterior hemiblock. Right bundle branch block and left anterior hemiblock - marked by prolonged QRS (> 120 ms or .12 seconds or longer) Complete left bundle branch block. Right bundle branch block and left posterior hemiblock. Right bundle branch block and left anterior hemiblock. Complete left bundle branch block.")
33
Trifascicular Block Complete block in the right bundle branch, and
Complete or incomplete block in both divisions of the left bundle branch Identified by EP Study Trifascicular block occurs when 3 of the conduction system pathways are blocked below the AV Node. Trifascicular block can have the appearance of AV nodal block. Combinations that constitute trifascicular block are: Right bundle branch block, complete left anterior fascicular block, and complete left posterior fascicular block Combination of complete block in one or two subdivisions of the common bundle, and incomplete block in one or two subdivisions

35
Knowledge Checkpoint Answer: Sinus bradycardia

36
Knowledge Checkpoint . Answer: First Degree AV Block

38
Diagnostic Test for Bradyarrhythmia:
EKG Holter Monitoring Implantable Loop Recorder EPS

39
Sinus Bradycardia Because of severe sinus bradycardia, Junctional ‘escape’ beats have appeared.

41
Investigation of the Site of AV Conduction Disease by Electrophysiologic Study (EPS)
")
43
Management : Drug Electrolyte Imbalance Hypothyroidism Post MI
PPM Implantation

44
Classification of Recommendations and Level of Evidence
Class I Benefit >>> Risk Procedure/ Treatment SHOULD be performed/ administered Class IIa Benefit >> Risk Additional studies with focused objectives needed IT IS REASONABLE to perform procedure/ administer treatment Class IIb Benefit ≥ Risk Additional studies with broad objectives needed; Additional registry data would be helpful Procedure/Treatment MAY BE CONSIDERED Class III Risk ≥ Benefit No additional studies needed Procedure/Treatment should NOT be performed/administered SINCE IT IS NOT HELPFUL AND MAY BE HARMFUL Level of Evidence: Level A: Data derived from multiple randomized clinical trials or meta-analyses Multiple populations evaluated; Level B: Data derived from a single randomized trial or nonrandomized studies Limited populations evaluated; Level C: Only consensus of experts opinion, case studies, or standard of care Very limited populations evaluated

45
Common Pacing Indications
The AHA and ACC have defined the indications for pacing based on the underlying arrhythmia At its simplest patients with the following conditions are commonly indicated for a pacemaker: Symptomatic bradycardia Sinus Node Disease (SND), or Sick Sinus Syndrome Complete Heart Block Chronotropic Incompetence Usually excludes “low grade” blocks (Mobitz I and 1st degree) Epstein et al. “ACC/AHA/HRS Guidelines for Device-Based Therapy.” JACC Vol. 51, No. 21, 2008.
, or Sick Sinus Syndrome. Complete Heart Block. Chronotropic Incompetence. Usually excludes low grade blocks (Mobitz I and 1st degree) Epstein et al. ACC/AHA/HRS Guidelines for Device-Based Therapy. JACC Vol. 51, No. 21,")
46
Sinus Node Dysfunction
IIa IIb III Permanent pacemaker implantation is indicated for sinus node dysfunction (SND) with documented symptomatic bradycardia, including frequent sinus pauses that produce symptoms. Permanent pacemaker implantation is indicated for symptomatic chronotropic incompetence. Permanent pacemaker implantation is indicated for symptomatic sinus bradycardia that results from required drug therapy for medical conditions. I IIa IIb III I IIa IIb III
 with documented symptomatic bradycardia, including frequent sinus pauses that produce symptoms. Permanent pacemaker implantation is indicated for symptomatic chronotropic incompetence. Permanent pacemaker implantation is indicated for symptomatic sinus bradycardia that results from required drug therapy for medical conditions. I. IIa. IIb. III. I. IIa. IIb. III.")
47
Sinus Node Dysfunction (cont’d)
IIa IIb III Permanent pacemaker implantation is reasonable for SND with heart rate less than 40 bpm when a clear association between significant symptoms consistent with bradycardia and the actual presence of bradycardia has not been documented. Permanent pacemaker implantation is reasonable for syncope of unexplained origin when clinically significant abnormalities of sinus node function are discovered or provoked in electrophysiological studies. Permanent pacemaker implantation may be considered in minimally symptomatic patients with chronic heart rate less than 40 bpm while awake. I IIa IIb III I IIa IIb III

48
Sinus Node Dysfunction (cont’d)
IIa IIb III Permanent pacemaker implantation is not indicated for SND in asymptomatic patients. Permanent pacemaker implantation is not indicated for SND in patients for whom the symptoms suggestive of bradycardia have been clearly documented to occur in the absence of bradycardia. Permanent pacemaker implantation is not indicated for SND with symptomatic bradycardia due to nonessential drug therapy. I IIa IIb III I IIa IIb III

49
Acquired Atrioventricular Blocks in Adults
IIa IIb III Permanent pacemaker implantation is indicated for third-degree and advanced second-degree atrioventricular (AV) block at any anatomic level associated with bradycardia with symptoms (including heart failure) or ventricular arrhythmias presumed to be due to AV block. Permanent pacemaker implantation is indicated for third-degree and advanced second-degree AV block at any anatomic level associated with arrhythmias and other medical conditions that require drug therapy that results in symptomatic bradycardia. I IIa IIb III
 block at any anatomic level associated with bradycardia with symptoms (including heart failure) or ventricular arrhythmias presumed to be due to AV block. Permanent pacemaker implantation is indicated for third-degree and advanced second-degree AV block at any anatomic level associated with arrhythmias and other medical conditions that require drug therapy that results in symptomatic bradycardia. I. IIa. IIb. III.")
50
Acquired Atrioventricular Blocks in Adults (cont’d)
IIa IIb III Permanent pacemaker implantation is indicated for third-degree and advanced second-degree AV block at any anatomic level in awake, symptom-free patients in sinus rhythm, with documented periods of asystole greater than or equal to 3.0 seconds or any escape rate less than 40 bpm, or with an escape rhythm that is below the AV node. Permanent pacemaker implantation is indicated for third-degree and advanced second-degree AV block at any anatomic level in awake, symptom-free patients with atrial fibrillation (AF) and bradycardia with 1 or more pauses of at least 5 seconds or longer. I IIa IIb III
 and bradycardia with 1 or more pauses of at least 5 seconds or longer. I. IIa. IIb. III.")
51
Acquired Atrioventricular Blocks in Adults (cont’d)
IIa IIb III Permanent pacemaker implantation is indicated for third-degree and advanced second-degree AV block at any anatomic level after catheter ablation of the AV junction. Permanent pacemaker implantation is indicated for third-degree and advanced second-degree AV block at any anatomic level associated with postoperative AV block that is not expected to resolve after cardiac surgery. I IIa IIb III

52
Acquired Atrioventricular Blocks in Adults (cont’d)
IIa IIb III B Permanent pacemaker implantation is indicated for asymptomatic persistent third-degree AV block at any anatomic site with average awake ventricular rates of 40 bpm or faster if cardiomegaly or left ventricular (LV) dysfunction is present or if the site of block is below the AV node. Permanent pacemaker implantation is indicated for second- or third-degree AV block during exercise in the absence of myocardial ischemia. I IIa IIb III
 dysfunction is present or if the site of block is below the AV node. Permanent pacemaker implantation is indicated for second- or third-degree AV block during exercise in the absence of myocardial ischemia. I. IIa. IIb. III.")
53
Acquired Atrioventricular Blocks in Adults (cont’d)
Permanent pacemaker implantation is reasonable for persistent third-degree AV block with an escape rate greater than 40 bpm in asymptomatic adult patients without cardiomegaly. Permanent pacemaker implantation is reasonable for asymptomatic second-degree AV block at intra- or infra-His levels found at electrophysiological study. Permanent pacemaker implantation is reasonable for first- or second-degree AV block with symptoms similar to those of pacemaker syndrome or hemodynamic compromise. I IIa IIb III I IIa IIb III B I IIa IIb III B

54
Acquired Atrioventricular Blocks in Adults (cont’d)
IIa IIb III B Permanent pacemaker implantation is reasonable for asymptomatic type II second-degree AV block with a narrow QRS. When type II second-degree AV block occurs with a wide QRS, including isolated right bundle-branch block, pacing becomes a Class I recommendation. (See Section 2.1.3, “Chronic Bifascicular Block” of the full text guidelines.)
")
55
Acquired Atrioventricular Blocks in Adults (cont’d)
IIa IIb III B Permanent pacemaker implantation is not indicated for asymptomatic first-degree AV block. (See Section 2.1.3, “Chronic Bifascicular Block” of the full-text guidelines.) Permanent pacemaker implantation is not indicated for asymptomatic type I second-degree AV block at the supra-His (AV node) level or that which is not known to be intra- or infra-Hisian. Permanent pacemaker implantation is not indicated for AV block that is expected to resolve and is unlikely to recur (e.g., drug toxicity, Lyme disease, or transient increases in vagal tone or during hypoxia in sleep apnea syndrome in the absence of symptoms). I IIa IIb III I IIa IIb III B
 Permanent pacemaker implantation is not indicated for asymptomatic type I second-degree AV block at the supra-His (AV node) level or that which is not known to be intra- or infra-Hisian. Permanent pacemaker implantation is not indicated for AV block that is expected to resolve and is unlikely to recur (e.g., drug toxicity, Lyme disease, or transient increases in vagal tone or during hypoxia in sleep apnea syndrome in the absence of symptoms). I. IIa. IIb. III. I. IIa. IIb. III. B.")
56
Chronic Bifascicular Block
IIa IIb III B Permanent pacemaker implantation is indicated for advanced second-degree AV block or intermittent third-degree AV block. Permanent pacemaker implantation is indicated for type II second-degree AV block. Permanent pacemaker implantation is indicated for alternating bundle-branch block. I IIa IIb III B I IIa IIb III

57
Chronic Bifascicular Block (cont’d)
IIa IIb III B Permanent pacemaker implantation is reasonable for syncope not demonstrated to be due to AV block when other likely causes have been excluded, specifically ventricular tachycardia (VT). Permanent pacemaker implantation is reasonable for an incidental finding at electrophysiological study of a markedly prolonged HV interval (greater than or equal to 100 milliseconds) in asymptomatic patients. Permanent pacemaker implantation is reasonable for an incidental finding at electrophysiological study of pacing-induced infra-His block that is not physiological. I IIa IIb III B I IIa IIb III B
. Permanent pacemaker implantation is reasonable for an incidental finding at electrophysiological study of a markedly prolonged HV interval (greater than or equal to 100 milliseconds) in asymptomatic patients. Permanent pacemaker implantation is reasonable for an incidental finding at electrophysiological study of pacing-induced infra-His block that is not physiological. I. IIa. IIb. III. B. I. IIa. IIb. III. B.")
58
Chronic Bifascicular Block (cont’d)
IIa IIb III Permanent pacemaker implantation may be considered in the setting of neuromuscular diseases such as myotonic muscular dystrophy, Erb dystrophy (limb-girdle muscular dystrophy), and peroneal muscular atrophy with bifascicular block or any fascicular block, with or without symptoms. Permanent pacemaker implantation is not indicated for fascicular block without AV block or symptoms. Permanent pacemaker implantation is not indicated for fascicular block with first-degree AV block without symptoms. I IIa IIb III B I IIa IIb III B
, and peroneal muscular atrophy with bifascicular block or any fascicular block, with or without symptoms. Permanent pacemaker implantation is not indicated for fascicular block without AV block or symptoms. Permanent pacemaker implantation is not indicated for fascicular block with first-degree AV block without symptoms. I. IIa. IIb. III. B. I. IIa. IIb. III. B.")
59
Hypersensitive CSS and Neurocardiogenic Syncope
IIa IIb III Permanent pacing is indicated for recurrent syncope caused by spontaneously occurring carotid sinus stimulation (CSS) and carotid sinus pressure that induces ventricular asystole of more than 3 seconds. Permanent pacing is reasonable for syncope without clear, provocative events and with a hypersensitive cardioinhibitory response of 3 seconds or longer. Permanent pacing may be considered for significantly symptomatic neurocardiogenic syncope associated with bradycardia documented spontaneously or at the time of tilt-table testing. I IIa IIb III I IIa IIb III B
 and carotid sinus pressure that induces ventricular asystole of more than 3 seconds. Permanent pacing is reasonable for syncope without clear, provocative events and with a hypersensitive cardioinhibitory response of 3 seconds or longer. Permanent pacing may be considered for significantly symptomatic neurocardiogenic syncope associated with bradycardia documented spontaneously or at the time of tilt-table testing. I. IIa. IIb. III. I. IIa. IIb. III. B.")
60
Hypersensitive CSS and Neurocardiogenic Syncope (cont’d)
IIa IIb III Permanent pacing is not indicated for a hypersensitive cardioinhibitory response to carotid sinus stimulation without symptoms or with vague symptoms. Permanent pacing is not indicated for situational vasovagal syncope in which avoidance behavior is effective and preferred. I IIa IIb III

61
Knowledge Checkpoint Name the four most common pacemaker indications.
Answer: Symptomatic bradycardia Sinus Node Dysfunction or Sick Sinus Syndrome Chronotropic Incompetence Complete Heart Block

62
Indicated? or Not Indicated?
Knowledge Checkpoint Permanent pacing is _______________ for situational vasovagal syncope in which avoidance behavior is effective and preferred. Indicated? or Not Indicated? Answer: Not indicated

63
Indicated? or Not Indicated?
Knowledge Checkpoint Permanent pacemaker implantation is ______________ for sinus node dysfunction (SND) with documented symptomatic bradycardia, including frequent sinus pauses that produce symptoms. Indicated? or Not Indicated? Answer: Indicated
 with documented symptomatic bradycardia, including frequent sinus pauses that produce symptoms. Indicated or Not Indicated Answer: Indicated.")
64
Indicated? or Not Indicated?
Knowledge Checkpoint Permanent pacemaker implantation is _____________ for symptomatic chronotropic incompetence. Indicated? or Not Indicated? Answer: Indicated

Similar presentations












 Heart Blocks>")



 Autonomic Nervous System.>")


>")

 Rates of automaticity – Too fast (tachycardia) – Too slow (bradycardia) – Too irritable (Premature) – Absent (block)>")

