Download presentation
Presentation is loading. Please wait.

1
Spirometry Study Day 23rd September 2010 Robert Daw
Clinical Lead Nurse for COPD BACHS

2
Anatomy and Physiology of COPD

4
COPD Definition ‘….airflow obstruction is usually progressive, not fully reversible and does not change markedly over several months. The disease is predominantly caused by smoking.’ NICE 2004

5
Asthma Definition ‘….in susceptible individuals, inflammatory symptoms are usually associated with widespread but variable airflow obstruction and an increase in airway response to a variety of stimuli. Obstruction is often reversible, either spontaneously or with treatment.’ BTS and SIGN 2003

6
Spirometry Spirometry is a method of assessing lung function by measuring the volume of air the patient is able to expel out from the lungs after maximal inspiration

7
Spirometry is a reliable method of identifying
Obstructive illness i.e. chronic obstructive pulmonary disease Reversible disease I.e. Asthma Restrictive disease i.e. Pulmonary fibrosis It can be used to grade the severity of COPD

8
Diagnosing COPD At the time of their initial diagnostic evaluation in addition to spirometry all patients should have: CXR FBC BMI

9
Additional Investigations
CT Scan ECG Echo Pulse Oximetry Sputum Culture Transfer factor for carbon monoxide (TLCO) Serial Domiciliary Peak Flows Alpha-1-antitrypsin
 Serial Domiciliary Peak Flows. Alpha-1-antitrypsin.")
10
Lung Volumes

11
Spirometry gives us 3 important measurements
FEV1 The volume of air that the patient is able to breathe out in the first second of forced expiration FVC The total volume of air that the patient can exhale forcibly in one breathe FEV1 / FVC The ratio is expressed as a percentage ALSO Peak Flow The volume of air that the patient is able to breathe out in the first 1000th of a second of forced expiration

12
Indices Measured

13
Spirometry - Maintenance of equipment

14
Spirometry Surveys Cooper B, 2005
Performing spirometry with no training were of poor standard when compared to labs Machines not being compared cared for or calibrated Minimum standards of acceptance Poor Interpretation

15
Calibration or Verification?
This is to check that the spirometer is reading correctly using a known standard. Calibration Calibration is the process in which the signal from a spirometer is adjusted to produce a known output.

16
Why is calibration / verification important
If equipment is not properly calibrated it can lead to false results – i.e. the patient may appear better or worse than they really are.

17
How often should I calibrate?
This depends on the equipment. Most pneumotach based equipment needs calibrating every day. Some equipment can only be calibrated by a trained engineer. In this case it is necessary to perform regular quality control / verification.

18
Verification Syringe This can be performed using a 3 litre syringe or 1 litre syringe depending on spirometer model. Results should be within 3% of calibration syringe Biological Control The person performing the quality control should have normal lung function. Results should not vary by more than 10% from the last time. Equipment should be calibrated if this is not the case.

19
Infection control Spirometers are a potential source of cross infection for patients. As a minimum one way cardboard mouthpieces should be used. Ideally (especially in high TB areas) bacterial filters are the mouthpiece of choice.
 bacterial filters are the mouthpiece of choice.")
20
Cleaning Ease of cleaning the equipment should be considered when purchasing Always use manufacturer guidelines. FLOW HEADS SHOULD BE CLEANED USING MANUFACTUROURS GUIDELINES AFTER EVERY SESSION IF NOT USING BACTERIAL FILTERS

21
Any Questions?

22
Spirometry – Pre Test Procedures

23
Pre-test procedures The patient, ideally, should –
- Avoid alcohol for at least 4 hours - Avoid eating a substantial meal - Wear loose fitting clothing If Reversibility is to be performed - - Avoid taking short acting bronchodilators for at least 4 hours prior to testing - Avoid smoking for 1 hour prior to testing -Be Well!!

24
Contraindications Haemoptysis of unknown origin
Pneumothorax (Need confirmation of resolution) Unstable cardiovascular status Myocardial Infarction (Last 3 months) Thoracic, abdominal or cerebral aneurysms
 Unstable cardiovascular status. Myocardial Infarction (Last 3 months) Thoracic, abdominal or cerebral aneurysms.")
25
Contraindications Recent Eye surgery (3 months)
Recent thoracic or abdominal surgery (3 months) Pregnancy (1st Trimester contraindicated but in 2nd and 3rd Trimester results may be effected by uterus size)
 Pregnancy (1st Trimester contraindicated but in 2nd and 3rd Trimester results may be effected by uterus size)")
26
Spirometry Technique

27
Reinforce and Reassure
Prior to Spirometry Gain verbal consent Check for contraindications and that the patient has been properly prepared for the test Gain an accurate height Make note of Ethnic Origin and Age The room should be a comfortable temperature The patient should be sat in a hard backed chair with their feet able to touch the floor The patient should sit upright with their legs uncrossed A drink of water should be made available The technique and purpose of spirometry should be explained in full prior to the test Spirometry should be performed in the patients own time and they should not feel hurried Reinforce and Reassure

28
Expiratory Relaxed Vital Capacity
Performed due to collapsing alveoli in some patients during Forced Vital Capacity technique This technique would usually be performed before the Forced Vital Capacity readings The reading is sometimes referred to as VC, EVC or RVC Minimum of three readings taken Two best results should be within 150mls of each other Maximum of 4 tests

29
Expiratory Relaxed Vital Capacity
Take as large a breath of air in as possible Pinch your nose or attach a nose clip to prevent air leakage Put the filter into your mouth ensuring that there are no leaks at the sides of your mouth Breathe out for as long as possible. This breath should be in your own time and should not be forced

30
Forced Vital Capacity (FVC)
A minimum of three readings should be taken There should be less than 5% or 150mls variance between the best two results The technique should be repeated until this is achieved or the patient is exhausted and can no longer perform the technique Time should be given to the patient to recover between readings

31
Forced Vital Capacity (FVC)
Take as large a breath of air in as possible Put the filter into your mouth ensuring there are no leaks at the side of your mouth Pinch your nose or attach a nose clip to prevent air leakage ‘Blast’ as quickly as possible and for as long as possible

32
Could we have a volunteer please ?
Demonstration Could we have a volunteer please ?

33
Technique Problems

34
The Normal Curve Volume Time
The vertical scale indicates total volume (l) the patient has blown out The horizontal scale indicates the total time (s) the patient has been blowing out for Note the initial part of the curve which is steep followed by a gradual flattening of the curve
 the patient has blown out. The horizontal scale indicates the total time (s) the patient has been blowing out for. Note the initial part of the curve which is steep followed by a gradual flattening of the curve.")
35
The Normal Curve Flow Volume Loop
The vertical scale indicates litres of air breathed out per second (L/s) at that moment in time The horizontal scale indicates total volume expired (L) Note the sharp peak at the beginning of the curve followed by an initially sharp trough that gradually flattens out
 at that moment in time. The horizontal scale indicates total volume expired (L) Note the sharp peak at the beginning of the curve followed by an initially sharp trough that gradually flattens out.")
36
Technique Problems Cough
This curve suggests the patient has coughed during a FVC reading Note the peaks and troughs that occur throughout the curve This will effect the FVC reading

37
Technique Problems Poor Effort
This curve suggests the patient has not blown as hard as they can during the FVC technique Note the rounded top to the peak at the beginning of the curve This will effect the FEV1 reading

38
Technique Problems Slow Start
This curve suggests the patient has started off blowing slowly during a FVC technique Note the peak in L/s comes in the middle of the curve rather than at the beginning This will effect the FEV1 reading

39
Technique Problems Inspiration
This curve indicates the patient has breathed in at the beginning of the technique This usually occurs when the patient puts the filter in their mouth before they have finished breathing in Note the negative L/s reading at the beginning of the curve This could effect all readings

40
Technique Problems Inspiration
This curve suggests the patient has breathed in at the end of the FVC technique This usually occurs when the patient attempts to take an extra breath in to prolong expiration Note the negative L/s at the end of the curve This could effect the FVC reading

41
Refreshments

42
Workshop

43
Correction Factors Ethnic Origin Correction Factor Caucasian 100%
BTS Guidelines Only Ethnic Origin Correction Factor Caucasian 100% Afro-Caribbean Reduce by 13% (87%) Asian Reduce by 7% (93%)
 Asian. Reduce by 7% (93%)")
44
References SPIROMETRY IN PRACTICE
A PRACTICAL GUIDE TO USING SPIROMETRY IN PRIMARY CARE 2ND Edition BTS 2005 GENERAL CONSIDERATIONS FOR LUNG FUNCTION TESTING ATS/ERS TASK FORCE: STANDARDISATION OF LUNG FUNCTION TESTING European Respiratory Journal 2005 STANDARDISATION OF SPIROMETRY

45
Spirometry Interpretation

46
Accurate Interpretation
Use Best Test (Less than 5% Variance from next best) Best Test – FVC, FEV1 or FVC & FEV1 If spirometer selects best test, CHECK Minimum number of tests <3 Is Interpretation correct?
 Best Test – FVC, FEV1 or FVC & FEV1. If spirometer selects best test, CHECK. Minimum number of tests <3. Is Interpretation correct")
47
Accurate Interpretation
Curve shape – effort, cough, extra breath etc Relaxed Expiratory Vital Capacity (EVC) recorded and used when better than FVC Accurate height Correction Factors
 recorded and used when better than FVC. Accurate height. Correction Factors.")
48
Recap FEV1 The volume of air that the patient is able to breathe out in the first second of forced expiration FVC The total volume of air that the patient can exhale forcibly in one breathe FEV1 / FVC The ratio is expressed as a percentage Peak Flow The volume of air that the patient is able to breathe out in the first 1000th of a second of forced expiration

49
ABREVIATIONS VITAL CAPACITY FORCED VITAL CAPACITY
VC, RVC, EVC FORCED VITAL CAPACITY Forced vital capacity describes the technique FVC RATIO Ratio, FER, FEV1%, FEV1/VC, FEV1/FVC

50
Predicted Values Done in 70’s Need modernising
Use age, height and sex to make prediction of ability Need to use correction factors for different ethnic origins Accurate height essential These can be reported as Percentage of Predicted Ranges Standard Residuals

51
Correction Factors Ethnic Origin Correction Factor Caucasian 100%
BTS Guidelines Only Ethnic Origin Correction Factor Caucasian 100% Afro-Caribbean Reduce by 13% (87%) Asian Reduce by 7% (93%)
 Asian. Reduce by 7% (93%)")
52
Predicted Values Done in 70’s Need modernising
Use age, height and sex to make prediction of ability Need to use correction factors for different ethnic origins Accurate height essential These can be reported as Percentage of Predicted Ranges Standard Residuals

53
Percentage of Predicted
Most frequently referred to value within the community Need to be aware that this gives an absolute value and clearly there is variability within normality Measured x 100 = % Predicted Predicted

54
% Predicted (Example) Ceri 55 years old 155 cm tall
FEV1 measured:1.64 l x 100 FEV1 predicted: l FEV1 % predicted: 76%

55
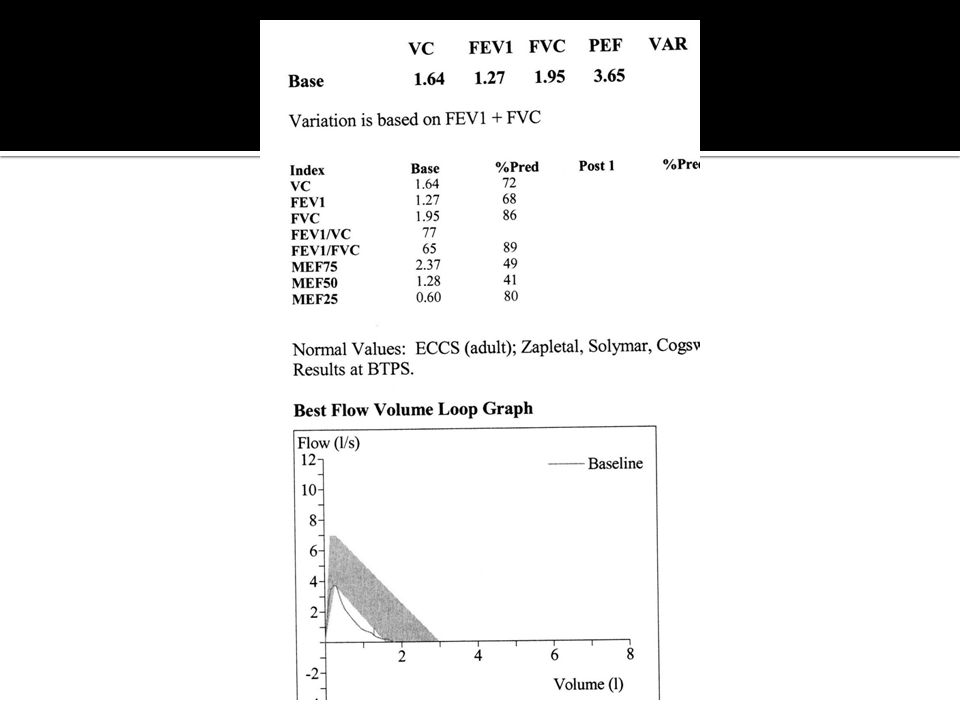
Looking at the printout

56
Normal Results FEV1 > 80% predicted FVC > 80% predicted

57
Obstruction FEV1 < 80% predicted FVC > 80% predicted
Ratio <70% Caution If ratio is low but FEV1 and FVC are normal there is still obstruction present

58
Obstructive Disorders
COPD Asthma Bronchiectasis Tumour Foreign Body

59
NICE 2010 Consider alternative diagnoses in:
Older people without typical symptoms of COPD where the FEV1/FVC is <0.7 Younger people with symptoms of COPD where the FEV1/FVC ration is ≥ 0.7

60
Restriction FEV1 <80% predicted FVC < 80% predicted
Ratio >70%

61
Restrictive Disorders
Kyphoscoliosis Muscular Dystrophy Problems Arthritis Pleural Problems Interstitial Lung Disease Obesity Drugs

62
Combined FEV1 <80% predicted FVC <80% predicted Ratio <70%

63
Combined Disorders Severe COPD Multiple Pathology e.g.
Kyphscoliosis and COPD Tumour and COPD

64
Severity of Obstruction
Based on % Predicted of FEV1 Good predictor of Prognosis Poor Predictor of Disability and Quality of Life Categories; BTS (1997) GOLD (2001) NICE (2004) NICE (2010)
 GOLD (2001) NICE (2004) NICE (2010)")
65
Severity of Obstruction
NICE Guideline (2004) ATS/ERS (2004) GOLD (2008) NICE Guideline (2010) Post-Bronchodilator FEV1/FVC FEV1 % Predicted Severity of Airflow Obstruction Post -Bronchodilator <0.7 ≥ 80% Mild Stage 1-Mild Stage 1-Mild* 50-79% Moderate Stage 2-Moderate 30-49% Severe Stage 3-Severe < 30% Very Severe Stage 4-Very Severe** *Symptoms should be present to diagnose COPD with mild airflow obstruction **or FEV1 <50% with respiratory failure
 ATS/ERS (2004) GOLD (2008) NICE Guideline (2010) Post-Bronchodilator FEV1/FVC. FEV1 % Predicted. Severity of Airflow Obstruction. Post -Bronchodilator. <0.7. ≥ 80% Mild. Stage 1-Mild. Stage 1-Mild* 50-79% Moderate. Stage 2-Moderate % Severe. Stage 3-Severe. < 30% Very Severe. Stage 4-Very Severe** *Symptoms should be present to diagnose COPD with mild airflow obstruction. **or FEV1 <50% with respiratory failure.")
66
Other Predictor of QOL and Prognosis
MRC score BODE Modified BODE AOD

67
Degree of breathlessness related to activities
MRC Dyspnoea Scale Grade Degree of breathlessness related to activities 1 Not troubled by breathlessness except on strenuous exercise 2 Short of breath when hurrying or walking up a slight hill 3 Walks slower than contemporaries on the level because of breathlessness, or has to stop for breath when walking at own pace 4 Stops for breath after walking about 100m or after a few minutes on the level 5 Too breathless to leave the house, or breathless when dressing or undressing

68
Bode Index

69
Bode Index

70
Annual FEV1? Used to detect sudden deterioration in lung function
Should precipitate action if deterioration marked. Normal deterioration in FEV1 thought to be 50ml/annum in none smoking individual

71
Asthma Or COPD ?

72
COPD Definition ‘….airflow obstruction is usually progressive, not fully reversible and does not change markedly over several months. The disease is predominantly caused by smoking.’ NICE 2004

73
Asthma Definition ‘….in susceptible individuals, inflammatory symptoms are usually associated with widespread but variable airflow obstruction and an increase in airway response to a variety of stimuli. Obstruction is often reversible, either spontaneously or with treatment.’ BTS and SIGN 2003

74
Post Bronchodilator Spirometry
QOF 12 (2009/10) states that a diagnosis of COPD should be confirmed by recording post bronchodilator spirometry Bronchodilator should be taken 15 minutes prior to spirometry being performed i.e. 4 puffs Salbutamol 100 MDI with AeroChamber Salbutamol 2.5mg nebuliser
 states that a diagnosis of COPD should be confirmed by recording post bronchodilator spirometry. Bronchodilator should be taken 15 minutes prior to spirometry being performed i.e. 4 puffs Salbutamol 100 MDI with AeroChamber. Salbutamol 2.5mg nebuliser.")
75
Post Bronchodilator Spirometry
Why? Post Bronchodilator recommended by GOLD and used in new trials e.g. UPLIFT Removes conflict with many guidelines Decrease work load in primary care Failure to use post bronchodilator over estimates COPD by 25% DOH 2009

76
Why Not Reversibility? Repeated FEV1 measurements can show small spontaneous fluctuations The results of a reversibility test performed on different occasions can be inconsistent and not reproducible Over-reliance on a single reversibility test may be misleading unless the change in FEV1 is greater than 400 ml The definition of the magnitude of a significant change is purely arbitrary Response to long-term therapy is not predicted by acute reversibility testing. NICE 2010

77
Present and progressive
Diagnosing COPD COPD Asthma Smoker or ex-smoker Nearly all Possibly Symptoms under the age 35 Rare Often Chronic Productive Cough Common Uncommon Breathlessness Present and progressive Variable Night time waking with breathlessness and or wheeze Significant diurnal or day to day variability of symptoms

78
20 pack years is considered a significant factor for developing COPD
Smoking History Cigarettes per Day x Years Smoked = 1 pack Year 20 e.g. 1 Pack Year = 20 cigarettes/day for 1 year or; 10 cigarettes/day for 2 years 40 cigarettes a day for 6 months 50g/2oz tobacco = 100 cigarettes Cigars – Café Crème = 3 cigarettes Hamlet = 5 cigarettes Corona = 8+ cigarettes 20 pack years is considered a significant factor for developing COPD

79
Present and progressive
Diagnosing COPD COPD Asthma Smoker or ex-smoker Nearly all Possibly Symptoms under the age 35 Rare Often Chronic Productive Cough Common Uncommon Breathlessness Present and progressive Variable Night time waking with breathlessness and or wheeze Significant diurnal or day to day variability of symptoms

80
Reversibility Useful if diagnosis is not clear Either;
Measure peak flows for 14 days morning and evening. Diurnal variation of greater than 20% indicates asthma Record pre and post bronchodilator spirometry

81
Repeat Spirometry after 15-30 minutes
Reversibility Repeat Spirometry following one of the following (Post); Salbutamol 100mcg MDI 4 puffs via spacer Salbutamol 2.5mg nebuliser Repeat Spirometry after minutes
; Salbutamol 100mcg MDI 4 puffs via spacer. Salbutamol 2.5mg nebuliser. Repeat Spirometry after minutes.")
82
Reversibility An FEV1 that increases by < 400mls is likely to have COPD An FEV1 that increases by > 400mls is likely to have asthma However if; FEV1 < 80% Ratio < 70% Post > 400mls Obstruction is not fully reversible

83
Reversibility (Example)
Billy FEV l FEV1 56% of predicted Ratio 40% Given Salbutamol 2.5mg nebuliser and spirometry repeated after 30 minutes POST FEV l FEV1 91% of predicted Ratio 71%

84
Case Studies

85
Case Study One Clive 47 years old
Smoked 30 cigarettes a day since he was 15 years old Painter and decorator Repeated chest infections every year Finding it difficult to climb ladders and walk up steep hills Chronic Productive Cough

86
References SPIROMETRY IN PRACTICE
A PRACTICAL GUIDE TO USING SPIROMETRY IN PRIMARY CARE 2ND Edition BTS 2005 GENERAL CONSIDERATIONS FOR LUNG FUNCTION TESTING ATS/ERS TASK FORCE: STANDARDISATION OF LUNG FUNCTION TESTING European Respiratory Journal 2005 STANDARDISATION OF SPIROMETRY

88
Case Study Two Carol 69 years old
Has smoked 10 a day since the age of 21 Retired cleaner Frequent chest infections Frequent hospital admissions Oxygen at home House bound 10 metre exercise tolerance None productive cough

90
Case Study Three Sarah 56 years old
Unemployed. Varied previous employment 3 recent admissions to hospital with breathlessness Normally walks to shops with no problems Breathing problems for the last 3 years Smoked 20 a day since the age of 18 Currently sleeping on the sofa as can’t make it up stairs Hospital measured spirometry on her last admission. Fev litres or 22% of predicted Normally none productive cough currently coughing up green sputum

92
Case Study Four Sam 35 years old Teacher
20 pack year history of smoking Breathless in the last 6 months Breathless on exertion and has to stop if walking fast None productive cough

94
Case Study Five Marjory
75 year old retired chef Never smoked 4 hospital admissions in the last year with breathlessness Home oxygen and nebulisers Breathless since being a baby with repeated infections Often walks to shops half a mile away, but when unwell unable to leave flat No cough

96
Case Study Six Suzanne 50 years old 30 pack year history of smoking
Never worked Recent frequent chest infections Occasional productive cough No exertional breathlessness Only breathless with chest infections

98
Case Study Seven Colin 85 years old Retired office worker
80 pack year history of smoking but gave up 6 months ago Regular rambler but finds himself increasingly breathless on hills 2 chest infections since giving up smoking No cough unless he has a chest infection

100
Case Study Eight Paul 56 years old 25 pack year history of smoking
Works in dusty warehouses Breathless for last 3 years 2 recent A&E admissions but discharged as panic attacks Maximum inhaled bronchodilator therapy for COPD Breathless around the house Breathlessness starts when he is coughing but not sure of trigger for coughing None productive cough Lots of stress at home at present During summer was playing 18 holes of golf

102
Case Study Nine Molly 75 years old
50 pack year history of smoking and still smokes 10 a day Retired office worker None productive cough Walks everywhere and plays bowls when well Breathless at rest and unable to leave the house when unwell Frequent exacerbations though can never bring anything up Audible wheeze at rest when unwell

104
Case Study Ten Bridget 77 years old
35 pack year history of smoking but ex smoker for 10 years Retired shop worker Breathless for the last 30 years since an acute episode of pulmonary Sarcoidosis (Inflammatory Lung Disease) which left lung scarring Breathlessness has got progressively worse in the last 5 years Long Term Oxygen and nebulisers Breathless at rest even when well Productive cough at all times
 which left lung scarring. Breathlessness has got progressively worse in the last 5 years. Long Term Oxygen and nebulisers. Breathless at rest even when well. Productive cough at all times.")
106
Case Study Eleven Eileen
72 years old None smoker Worked in wool mills as spinner for 5 years then a teacher Breathless for last 15 years Chronic Productive Cough Frequent exacerbations No hospital admissions 5 metre exercise tolerance Long term Oxygen and nebulisers Plays cards 7 times a week and goes to the gym on a Friday

108
Case Study Twelve Mohammed
62 years old Breathless for last year Breathless on exertion Exercise tolerance 200 metres None smoker Works in a shop No chest infections None productive cough

Similar presentations













>")




 Airway.>")

 2008.>")



 M A Med Ed (Keele)>")


 By Chris Callan 23 April 2008.>")



 Diagnosis and management of chronic asthma in line with current BTS guidelines (Dr Lowery) 3 x Case.>")