Download presentation
Presentation is loading. Please wait.

1
Safe prescribing: How to avoid prescribing errors
Kevin Gibbs Clinical Pharmacy Manager United Bristol Healthcare Trust

2
Aims To provide an awareness of:
Common medication errors How to minimise these National and local resources available to you to aid in safer prescribing To give you some prescribing pointers to look out for in your clinical placements

3
By the end of the session you should be able to:
Define a medication error List the ‘Five Rights’ Identify common types of medication errors Begin to think about how to minimise errors by using your knowledge, skills and available resources

4
During your placements Think about:
What do I need to prescribe in a safe way? Patient information Co-morbid conditions Drug information Pharmacology Pharmacokinetics and pharmacodynamics Therapeutics Systems Policies, guidelines, prescribing aids etc

5
What is an error?

6
What is an error ? Doses omitted Wrong dose Unprescribed drug given
Wrong dosage form given Wrong route of administration Wrong rate of administration Wrong time of administration time of day in relation to food etc.... Using unstable/expired drug Wrong administration technique Incorrect reconstitution Extra dose given

7
Where do errors occur in the process of giving a drug?
Prescribing Dispensing Administration Counselling/communication

8
Adverse events in hospitals What is the size of the problem?
Adverse events per admission (%) 10% AE number / year in UK 850,000 Cost in additional hospital stay (£) £2 billion Cost of clinical negligence schemes/yr £400 million Medication errors = % of incidents 25% An organisation with a memory. Dept of Health 2001
 10% AE number / year in UK. 850,000. Cost in additional hospital stay (£) £2 billion. Cost of clinical negligence schemes/yr. £400 million. Medication errors = % of incidents. 25% An organisation with a memory. Dept of Health")
9
Reported incidences Difficult to estimate due to varying definitions - US/UK Prescribing errors 3-20 per 1000 prescriptions Medication errors 1 per patient per day Been estimated that drug errors account for 1/5 of all deaths due to adverse drug events

10
Outcomes Data collated by US National Co-ordinating council for Medication Error Reporting and Prevention Performance deficit 29.8% Communication problem 15.8% Knowledge deficit 14.2% Dose miscalculation 13% 5366 reports 68.2%- Serious patient outcomes 9.8% - fatal Improper dose Wrong drug Wrong route of administration Phillips, J etal. Am J Health Syst Pharm 2001;58:

11
Prescribing errors Process Error Rate Serious Errors
(Primary Care) Computer generated 7.9% Hand written 10.2% (Hospital) 1.5% 0.4% Dean B, Schachter M, Vincent C, Barber N. Quality and Safety in Healthcare 2002; 11: Shah SNH, Aslam M and Avery AJ. Pharm J. 2002; 267:
 Computer generated. 7.9% Hand written. 10.2% (Hospital) 1.5% 0.4% Dean B, Schachter M, Vincent C, Barber N. Quality and Safety in Healthcare 2002; 11: Shah SNH, Aslam M and Avery AJ. Pharm J. 2002; 267:")
13
Handwriting

14
Errors in medication history taking
Literature review 22 studies, 3755 patients Errors in medication histories In up to 67% of cases 10-61% had at least 1 omission error 54% of patients had at least 1 medication history error Clinically important errors in 11-59% Tam et at Canadian Medical Association Journal 2005;173(5):510-15
:")
15
Dispensing and adminn errors
Stage of process Error Rate Serious Errors Dispensing errors (P) 1% 0.18% Dispensing errors Undetected (H) 0.0002 Administration Oral Medicines (H) 3 – 8% Preparation and admin of parenteral medicines 13%- 49% UK references 1 – 12 from Building a safer NHS, Medication Safety
 1% 0.18% Dispensing errors. Undetected (H) Administration. Oral Medicines (H) 3 – 8% Preparation and admin of parenteral medicines. 13%- 49% UK references 1 – 12 from Building a safer NHS, Medication Safety.")
16
Similar packaging Same drug – different manufacturers

17
Similar packaging Same drug – several strengths
May be colour-coded but DO NOT rely on colour

18
Similar packaging Similar sounding names / similar spelling / same strength Ceftazidime – Cefotxime

19
Similar packaging If in a hurry – These look similar
Water for injection, Sodium Chloride injection So does Potassium 15% injection = Why there are NPSA/Trust policy on restricting this

20
Summary: Common error types
Wrong patient Contra-indicated medicine Allergy, medical condition, drug-drug interaction Wrong drug / ingredient Wrong dose / frequency Wrong formulation Wrong route of administration Wrong quantity

21
Incorrect IV administration calculations or pump rates
Poor handwriting on Rx Incorrect IV administration calculations or pump rates Poor record keeping/checking double doses wrong patient Paediatric doses Poor administration technique

22
Complicated prescriptions Calculations Verbal orders
Lack of knowledge about drugs Mistakes in identifying drugs names packaging misreading

23
National & local examples
Discharged on warfarin loading dose 10mg od Not referred for dose adjustment to clinic 14days of 10mg od INR 12.3 Admitted with frank haemorrhage Weight-related dose for tinzaparin – 80kg estd Patient was 51kg, risk of haemorrhage Rx: Ranitidine 50mg Given via epidural line rather than central line

24
Discharged on warfarin loading dose 10mg od
Not referred for dose adjustment to clinic 14days of 10mg od INR 12.3 Admitted with frank haemorrhage Weight-related dose for tinzaparin – 80kg estd Patient was 51kg, risk of haemorrhage Rx: Ranitidine 50mg Given via epidural line rather than central line

25
CABG patient, standard therapy
Thyroxine missed on admission, discovered day 10 Galantamine re-started after a gap, Rx; 8ml qds Should have been 12mg (2ml) bd prescriber confused over liquid strength Rx: Co-amoxiclav Penicillin-alllergic Did not realise this is a penicillin anaphylaxis
 bd. prescriber confused over liquid strength. Rx: Co-amoxiclav. Penicillin-alllergic. Did not realise this is a penicillin. anaphylaxis.")
26
Anaesthetist adjusted rate of fentanyl syringe pump in Theatre
New pump. Increased rate x 1000 Respiratory arrest - death Rx: morphine 0.4ml 4ml given 30% sodium chloride used instead of 0.9% to dilute an epidural Severe pain

27
Respiratory arrest. Syringes made up in advance and not labelled
In Theatre: Sodium chloride flush for a central line switched with fentanyl Respiratory arrest. Syringes made up in advance and not labelled IV line flushed with sodium chloride 0.9% Was in fact Potassium 15% → death Ampoules look similar in design

28
Case study 1 – "Cambridge" Rx Methotrexate 17.5mg once a week
New Rx 10mg once a day 10mg daily dispensed by locum pharmacist Rx error noticed by 2nd GP, but the computer record was not altered +5/7 patient admitted to ENT ward

29
Drug chart written for 100mg daily
+1/7 Nurse d/w patient – back to 10mg od +1/7 Pharmacist queries and asks nurse to ask Dr to check dose GP records confirm 10mg od +2/7 blood tests re-checked } Haem +5/7 patient dies

30
Case study 2 – “Nottingham”
Rx Intrathecal methotrexate under GA in theatre by Oncology Reg & intravenous vincristine on ward by specialist nurse "Outlied" on non-specialist ward Both drugs delivered to theatre from ward Given food pre-op – op postponed

31
Orignal SpR off-duty now
Cover SpR unable to leave ward, anaesthetist to admin intrathecal drug Aneasthetist had given I/Thecal drugs before but had never given chemotherapy Methotrexate given intravenously Vincristine given intrathecally Patient died

32
Improving medication safety
Department of Health. Jan 2004

33
Improving medication safety: Main areas of medication error
Anaesthetic practice Anticoagulants Cytotoxic drugs Intravenous infusions Methotrexate Opiate analgesics Potassium chloride

34
Causes → Solutions Lack of knowledge of the drug – 31%
Wrong dose, choice, drug. Interaction Allergy checking “rule” violations – 10% Incl. communication problems “Slip” or memory loss – 9% Drug information Eg: Interactions Resources available Patient condition Renal / liver function Guidelines, formulary Leape et al. JAMA 1995;274:35-43

35
Avoiding errors Patient knowledge Have a therapeutic goal
Is prescribing the right answer? Have you included the patient in this decision? Knowledge about the drug Monitor for effects and adverse effects Use your resources Good communication

36
Taking a good medication history
How reliable is your source – does it have enough detail? Patient, patient’s repeat prescription, own drugs, GP admission letter, on-call service Drug details dose, frequency, formulation (eg modified release), start date, indication Include: Prescribed drugs, ‘OTC’ drugs, complementary medicines, vitamins, ? ‘Recreational drugs’ Allergies including severity Compliance Therapeutic failures
, start date, indication. Include: Prescribed drugs, ‘OTC’ drugs, complementary medicines, vitamins, ‘Recreational drugs’ Allergies including severity. Compliance. Therapeutic failures.")
37
Factors affecting a drugs pharmacodynamics or pharmacokinetics
Children The elderly Renal impairment Hepatic impairment Prescribing in pregnancy or breast feeding Drug interactions More later….. Further references: Clinical Pharmacology textbook – use course recommendation Basic Clinical Pharmacokinetics. 4th edn. ME Winter. Covers Drug-specific kinetics eg Digoxin, gentamicin

38
Drug dosing in renal impairment
Based on estimation of renal function using creatinine clearance Cockcroft-Gault equation Crcl = F x (140-age)x wt in kg S.Cr in micromol/L Where F = 1.23 for males, 1.04 for females Or use an on-line calculator such as
x wt in kg. S.Cr in micromol/L. Where F = 1.23 for males, 1.04 for females. Or use an on-line calculator such as.")
39
Drug-drug interactions drug-food interactions
Resources BNF Appendix 1 Pharmacy Medicines Information Departments Have specialists texts and other resources to help mOre in a leter talk

40
Resources available to you
Summary of Product Characteristics for each medicine - eMC Pharmacy Medicines Information On-line National Electronic prescribing Other medical and non-medical prescribers

41
Pharmacy Avaliable for help and advice Ward Pharmacist
Local Medicines Information department Regional medicines Information Mainly Community sector enquiries Out-of-hours: On-call or resident pharmacist

42
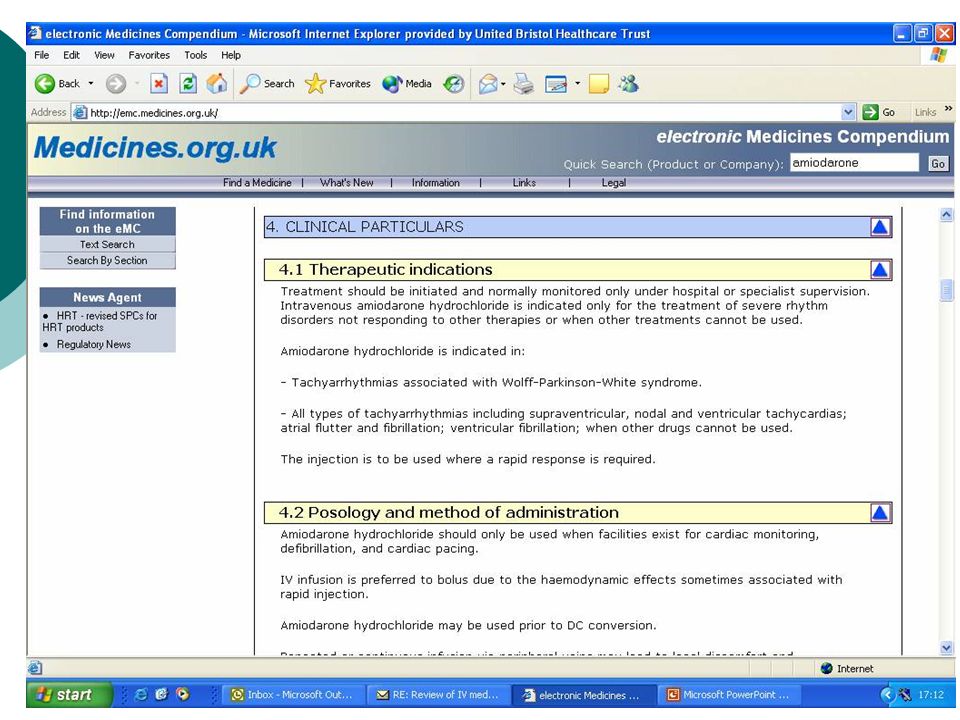
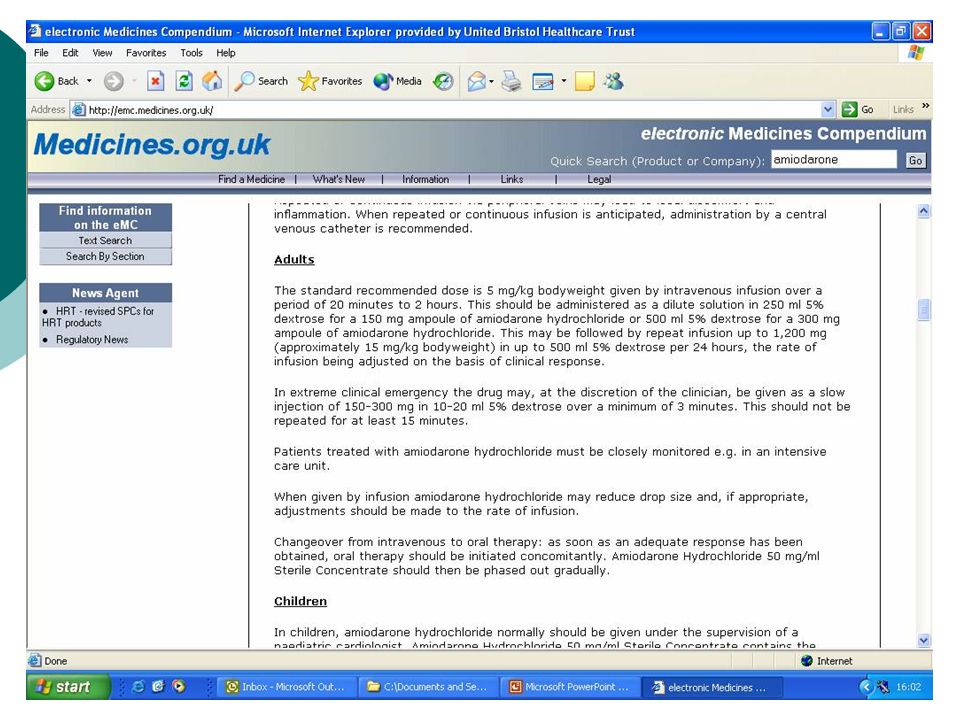
Electronic Medicines Compendium (eMC)
The eMC provides up-to-date information on licensed UK medicines Summary of Product Characteristics (SPCs) Patient Information Leaflets (PILs). SPCs are legal & technical documents with information to help guide on the best way to use a medicine.
 Patient Information Leaflets (PILs). SPCs are legal & technical documents with information to help guide on the best way to use a medicine.")
48
In summary

49
Prescribing responsibilities
Drug Dose Route Rate of administration Duration of treatment Checking patient allergies & sensitivities

50
Providing a prescription that is:
Legible Legal Signed Giving all information to allow safe administration

51
Hints Clear and unambiguous Approved name No abbreviations
Care with IVs Care with units Legal Is it weight/BSA- related dosing. Is weight accurate?

52
Rewrite charts regularly
Clear decimal points 0.5ml not .5ml Rewrite charts regularly Take time, eg to read labels Avoid abbreviations od / bd / tds / qds Not 250mg3

53
Take particular care if:
Impaired renal function Hepatic dysfunction Children The elderly Drug is unknown to you Very new drug

54
Remember the “Five Rights”
the right patient the right drug the right time the right dose the right route

55
If in doubt …….. Ask

56
Further reading & resources
Naylor, R. Medication Errors. Radcliffe Press. ISBN Department of Health. (2004). Building a safer NHS. Improving medication safety. National Patient Safety Agency Website:
. Building a safer NHS. Improving medication safety. CONTENT_ID= &chk=PH2sST. National Patient Safety Agency. Website:")
57
National Prescribing Centre
Website: Institute for Safe Medication Practices (ISMP) (American) Website: National Electronic Library for Medicines Website: Aronson & Richards. Oxford Handbook of Practical Drug Therapy. ISBN
 (American) Website: National Electronic Library for Medicines. Website: Aronson & Richards. Oxford Handbook of Practical Drug Therapy. ISBN")
Similar presentations






 Reporting systems are vital in providing a core of sound, representative information on which to base analysis.>")














 All paediatric wards have a visit.>")

