Download presentation
Presentation is loading. Please wait.

1
Texas Pandemic Influenza Preparedness
Cynthia Morgan, PhD, RN Pandemic Influenza Program Coordinator, Acting Anita Wheeler, BSN, RN School Nurse Consultant

2
Agenda Everything you wanted to know about pandemic influenza but couldn’t find anyone to ask What you can do to prepare your family What you can do to prepare your school What you can do to prepare your students & their families

3
Everything you wanted to know. . .
Definitions Examine reasons pandemics occur Look at the progress of Avian H5N1 Influenza Discuss why we are concerned Review current prevention efforts Consider the state of the science

4
Avian vs Pandemic Influenza
?

5
Epidemiology of Avian flu in humans
Avian (Bird) Flu is a disease of birds All Avian Flu viruses are endemic in waterfowl & do not harm them Wild birds mix with domestic chickens in back yard farms Domestic chicken flocks mix in live poultry markets People mix with sick or dead chickens People catch Avian Flu
 Flu is a disease of birds. All Avian Flu viruses are endemic in waterfowl & do not harm them. Wild birds mix with domestic chickens in back yard farms. Domestic chicken flocks mix in live poultry markets. People mix with sick or dead chickens. People catch Avian Flu.")
6
Seasonal vs Pandemic Flu
Annually Known virus Vaccine available (usually) High mortality young & old esp. w/ health problems Pandemic Irregular intervals Novel virus No or mismatched vaccine High mortality in year olds; mortality in young similar to seasonal flu
 High mortality young & old esp. w/ health problems. Pandemic. Irregular intervals. Novel virus. No or mismatched vaccine. High mortality in year olds; mortality in young similar to seasonal flu.")
7
Pandemics of the 20th Century
Year Name Strain Deaths 1918 Spanish H1N1 >50 million (US 675,000) 1957 Asian H2N2 1 – 2 million 1968 Hong Kong H3N2 700,000
 Asian. H2N2. 1 – 2 million Hong Kong. H3N2. 700,000.")
9
Composition of Seasonal Vaccines
2004 – 2005 A / New Caledonia / 99 / H1N1 A / Fugian / 02 / H3N2 2005 – 2006 A / California / 03 / H3N2 2006 – 2007 (recommended) A / Wisconsin / 05 / H3N2 Looking at the A viruses what observations can you make? The H&Ns are the same as for the Spanish Flu and the Hong Kong flu but they have different names. The H3N2s have different names each year.
 A / Wisconsin / 05 / H3N2. Looking at the A viruses what observations can you make The H&Ns are the same as for the Spanish Flu and the Hong Kong flu but they have different names. The H3N2s have different names each year.")
10
Pandemics of the 20th Century
Year Name Strain Deaths 1918 Spanish H1N1 >50 million (US 675,000) 1957 Asian H2N2 1 – 2 million 1968 Hong Kong H3N2 700,000 Going back – these are the same strains that cause pandemics in the past. What happened?
 Asian. H2N2. 1 – 2 million Hong Kong. H3N2. 700,000. Going back – these are the same strains that cause pandemics in the past. What happened")
11
Antigenic change Antigenic ‘drift’ occurs in HA and NA
Associated with seasonal epidemics Continual development of new strains secondary to genetic mutations Antigenic ‘shift’ occurs in HA and NA Associated with pandemics Appearance of novel influenza A viruses bearing new HA or both HA & NA Here is an analogy. Dogs come in various broad classes (Saint Bernards, Collies, Dachshunds, etc.) that are very different from each other. They are all dogs, but they don’t look much alike. These are the H1, H2, etc. and N1, N2, etc. classes of glycoproteins. Within each breed there are also smaller variations: some variation in size, hair color, pattern, etc. These are the strains of virus within each H–N subtype combination. If the only dog you know is a black Saint Bernard with a rough coat you may be a bit confused when confronted with a red Saint Bernard with a smooth coat, and if you encounter a chihuahua you may not even recognize the animal before you is a dog. Similarly your immune system may be slow and ineffective in recognizing different strains of the same viral subtype and not even ‘see’ a different subtype at all. Our immune systems have no experience with the H5 subtype of influenza A virus, which is one of the main reasons public health officials are so concerned: one of our main defense systems, the immune system, may be ineffective until it learns to recognize this subtype, and the learning only takes place after infection. In the case of previous infections with the same subtype, even if the strain is different, there may some recognition and the response, while delayed, may still have some effectiveness. But with the H5 subtype, the virus will reproduce unhindered for much longer and your immune system may not have enough time to make antibodies at all.
 that are very different from each other. They are all dogs, but they don’t look much alike. These are the H1, H2, etc. and N1, N2, etc. classes of glycoproteins. Within each breed there are also smaller variations: some variation in size, hair color, pattern, etc. These are the strains of virus within each H–N subtype combination. If the only dog you know is a black Saint Bernard with a rough coat you may be a bit confused when confronted with a red Saint Bernard with a smooth coat, and if you encounter a chihuahua you may not even recognize the animal before you is a dog. Similarly your immune system may be slow and ineffective in recognizing different strains of the same viral subtype and not even ‘see’ a different subtype at all. Our immune systems have no experience with the H5 subtype of influenza A virus, which is one of the main reasons public health officials are so concerned: one of our main defense systems, the immune system, may be ineffective until it learns to recognize this subtype, and the learning only takes place after infection. In the case of previous infections with the same subtype, even if the strain is different, there may some recognition and the response, while delayed, may still have some effectiveness. But with the H5 subtype, the virus will reproduce unhindered for much longer and your immune system may not have enough time to make antibodies at all.")
12
Mechanisms of Antigenic Shift
Reassortment in humans Direct Infection Non-human virus Human virus Since the H5N1 and the 1918 H1N1 (found last year) investigations we have learned that a reassortment event that could create a pandemic strain could directly occur in humans potentially increasing the likelihood of a pandemic. Recent research on the 1918 Spanish Flu virus seems to have done this. Indirect Infection Reassorted virus
 investigations we have learned that a reassortment event that could create a pandemic strain could directly occur in humans potentially increasing the likelihood of a pandemic. Recent research on the 1918 Spanish Flu virus seems to have done this. Indirect Infection. Reassorted. virus.")
18
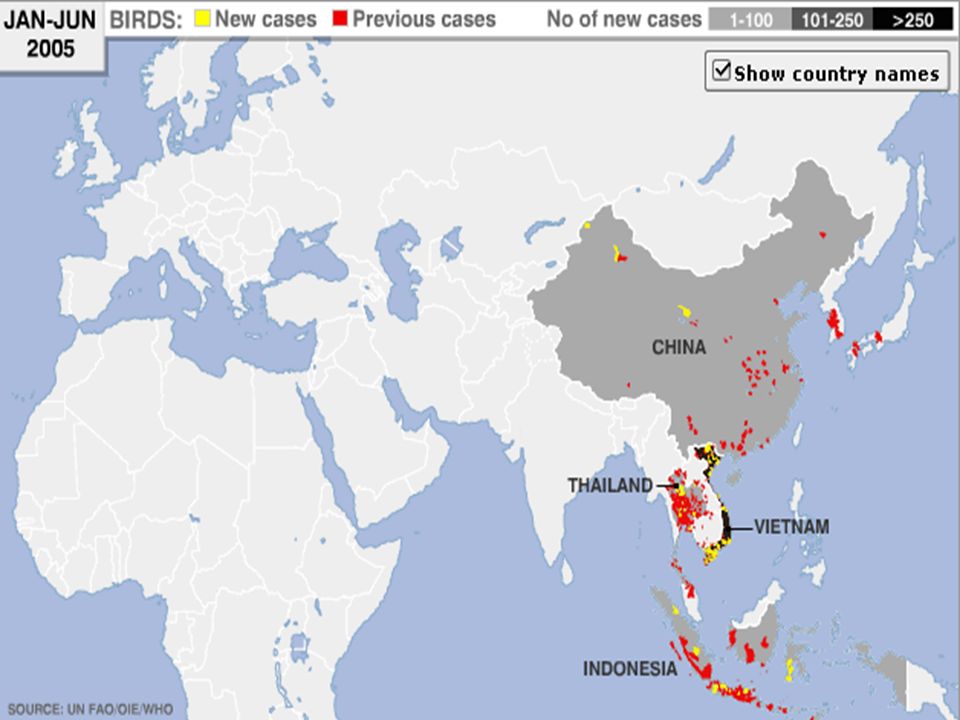
Countries with H5N1 Influenza in animals & humans
Countries with H5N1 influenza in humans 51 18 11 10 5 2 1 2 2003 2004 2005 2006 Through June 15, 2006

19
Bird and Human Cases H5N1 June 13, 2006 Bird Cases Human Cases

20
Risk factors: Handling sick or dead birds Exposure to feces of sick or dead birds Inhaling dust contaminated with feces Risk locations areas of overlap Open backyard chicken flocks Green East Atlantic flyway overlapping in Canada w/ Atlantic American & Open air bird markets Mississippi American Dead birds in the wild Blue East Asian overlapping with the Pacific Americas & Mississippi Americas Prevention is the key Increased surveillance in wild birds – migratory overlap This will provide early warning for us Bans on imported birds – England’s case was an imported parrot Indoor facilities for chicken production Excellent surveillance and control in chicken production facilities Vaccination – French and Dutch have program approved to vaccinate free-range chickens and backyard chickens and for producers in 3 areas deemed high risk

21
The H5N1 Flu Threat to Humans
A new virus to which humans have no immunity - Yes The virus causes significant human illness or death - Yes The virus spreads easily from person-to-person – NO The Avian Flu (H5N1) virus has 2 out of 3 of these today…
 virus has 2 out of 3 of these today…")
22
Why the Concern with H5N1? 1918 (H1N1) flu and H5N1 avian flu are the only “kissing cousins” among the 169 known avian flu viruses.
 flu and H5N1 avian flu are the only kissing cousins among the 169 known avian flu viruses.")
23
1918 Influenza Pandemic 20-40 million persons died worldwide, possibly more Death rate 25 times higher than previous epidemics ,000 deaths in the U.S.: Ten times as many Americans died of flu than died in WW I The epidemic preferentially affected and killed younger, healthy persons The epidemic was so severe that the average life span in the U.S. was depressed by 10 years

24
MOST FATAL EVENT IN THE LAST 300 YRS
U.S. LIFE EXPECTANCY AT BIRTH

25
1918 H5N1 Incident rate (0-75) 15 55 Young through middle age are most likely to become infected; elderly less likely. Remember the to 55 year olds

26
Case fatality rate comparison (0-75)
U-shaped is seasonal flu case fatality rate W is pandemic; pattern is being seen with H5N1 Middle age has healthiest immune system. Over reacts to the highly virulent virus, Over reaction called cytokine storm. People die of Adult Respiratory Distress Syndrome. This was also seen with SARS. 15 55

27
Case fatality rate comparison

28
Cytokine Storm Has been suggested as an explanation for the devastating nature of the 1918 flu Is an over reactive immune response that causes multiple organ system failure Evidence indicates H5N1 deaths are caused by this Chemokines and cytokines are the "messengers of the immune system" and are critical in coordinating and regulating the immune response. Altering this balance is likely to lead to an uncontrolled inflammatory response in the lung and probably explains, at least in part, the severe lung inflammation associated with avian flu virus H5N1. One of the many possible effects of cytokines is to summon other immune cells to the site of microbial attack and to activate those cells so that they, too, elaborate cytokines which in turn summon still more cells. This is a positive feedback loop and is ordinarily damped down by other cytokines signalling still other cells to elaborate still more cytokines that put the brakes on the process. Ordinarily this works well. But most regulatory mechanisms can get out of kilter and this can happen in a variety of different ways. The cytokines do not turn off, immune cells become overstimulated and run amok. Occurs in people with excellent immune systems.

29
50% of workforce over 1 year
Worst Case Scenario Patient Severe (1918-like) National Texas Number sick 150M 11.5M Outpatient 75M (50%) 5.75M Hospitalized 16.5M (11%) 1,265,000 ICU Care 2.5M (15%) 199,750 Ventilator 1.25M (50%) 94,780 Death 3.225M (2.15%) 247,250 Absenteeism 50% of workforce over 1 year
 National. Texas. Number sick. 150M. 11.5M. Outpatient. 75M (50%) 5.75M. Hospitalized. 16.5M (11%) 1,265,000. ICU Care. 2.5M (15%) 199,750. Ventilator. 1.25M (50%) 94,780. Death M (2.15%) 247,250. Absenteeism. 50% of workforce over 1 year.")
30
Pandemic wave mortality

31
In 1957 it took 4-6 months for the pandemic to spread to the US
In 1957 it took 4-6 months for the pandemic to spread to the US. It will take significantly less time with travel as it is today.

32
Animal intervention

33
Society during a pandemic
Healthcare system Work School Travel Supplies Services Worst case scenario – anarchy. We are expecting less. HCDS Overwhelmed. Enough beds for 15% of those who become ill Sick needing professional care in alternate buildings No elective surgeries Flu clinics in tents to limit exposure in hospitals Work Business contingency planning – ID critical tasks, cross train, telecommuting Schools close because staff and kids ill before health offiicial closes them Parents stay home not only because they are sick, but kids at home, and possibly need to care for sick family member Supplies and services Food in short supply as staff in stores, distributors, manufactures ill Critical services – limited; garbage pick-up rare, power outages, critical system maintenance issues Banks may be closed. Limited law enforcement

34
Prevention & Containment – Nonpharmaceutical
Public Health population focused measures Personal protective measures Business contingency planning Care of sick at home In actuality this is probably all we’ll really have during the first wave.

36
Potential Community Measures to Decrease Transmission
Travel advisories/limit travel to affected areas Screening travelers from affected areas* Limit large public gatherings; close schools Encourage telecommuting Limit availability of public transportation Hand hygiene, respiratory hygiene/cough etiquette Quarantine of exposed persons* Education to allow early identification and isolation of cases* * Note: Some measures may be most useful early in outbreak and with strains that are not efficiently transmitted

37
Evidence for use of masks
Limited evidence available on benefits of masks in preventing healthcare or community influenza transmission Use prudent at least in healthcare settings SARS studies have shown clear benefit mask use in healthcare setting Short incubation period Difficult to trace source of outbreak since cases usually occur during community outbreaks Unknown if type of mask may make a difference (N-95 versus surgical, etc.) Did not appear to be helpful in , but quality of masks and adherence to use questionable
 Did not appear to be helpful in , but quality of masks and adherence to use questionable.")
38
Influenza Antiviral Drug Questions
How much supply will there be? Will feds or state have control over distribution decisions? How should it be used? Who should get it? How can it be delivered? Where does the $$ come from? Antivirals are marginally useful even if available: For treatment – must be started w/I 48 hour of beginning of symptoms Will then reduce length of illness by a few days and possibly reduce chances of secondary infections For prophylaxis after exposure – must be able to know when you have been exposed. Difficult since a person is contageous 1=2 days before symptoms. Tamiflu and Relenza can only be used post exposure not long term One strain is showing some resistance to antivirals all ready

39
12/07?? 50 million courses Texas: M people. The federal goal is to have enough stockpiled to treat 25% of the population and have 4 post-exposure prophy courses for critical service providers. SNS share of 50 M courses = 3.3 M courses which are totally paid for by the feds. TX option on 31M federal contract 75/25 split = 2.3M courses = $32.5M Total of 5.6M courses leaves us 150,000 short of treatment for 25% of the population – none for prophylaxis of health care personnel or critical service providers even though CDC calls for 4 post-exposure courses This works assuming: you know when you are exposed and it happens only 4 times during a pandemic that lasts 1 year with 3 waves totaling 180 days. To prophylax the 4 suggested times would require purchase on state contract price of $40 = $47M for a grand total of ~80M We need to let CDC know by 7/1/06 how much of our allotment we want to reserve for purchase Issues: Do we want to purchase; where will the $$ come from; priorities (science and ethics) Just this month CDC announced AVs in their control will be used for illness only. We are seeking clarification for the state option purchase Where do the dollars come from? General revenue after legislative budged approval.
 Just this month CDC announced AVs in their control will be used for illness only. We are seeking clarification for the state option purchase. Where do the dollars come from General revenue after legislative budged approval.")
40
Influenza Antiviral Drug Questions
How much supply will there be? Will feds or state have control over distribution decisions? Where do the $$ come from? How should it be used? Who should get it? How can it be delivered? Next 4 are intertwined Expert panel 5/18 – scientists, flu experts, ethicists, lawyers, faith community, consumer advocates – 3 separate groups hand divided to be balanced representation – similar conclusions: highest priorities should be: outbreak control for early containment which is a treatment/prophy mix, and critical service providers. If we have no health care providers, no police or fire protection, and utilities or no food Sick patients should be treated by the usual private sector routine; public sector should be concerned about outbreak control, prophy for target groups, and tx for safety net populations Should we buy it and how much? Depends on the second and third bullets

41
Influenza Vaccine Questions
When will it be available? How much will there be? How effective will it be? Who will own it? How should it be delivered? Who should get it? Who will pay for it? What about vaccine – that’s a better alternative When will it be available and how effective will it be we’ll discuss in a minute Who will own it? While it is in short supply my guess is the feds and/or states. I don’t beiieve it will be in the private sector until there is plenty. Who will pay for it? So far the public has through taxes. Once doses are available I suspect it will be government owned. Whether or not you will be charged, I have not heard anything. When it is plentiful, it will revert to private sector control as seasonal vaccine is today. How should it be delivered ties in with who should get it. CDC has a recommended priority list that states will consider and may possibly alter to reflect needs. If a pandemic occurs before vaccine is available and while the vaccine is in short supply, it will be given to priority groups in settings easily accessible, e.g hospitals for staff with direct patient contact; fire stations for EMS, etc. When we’re ready for the general public, we will potentially do mass clinics. Unlike antivirals which are all ready circulating in the private domain, vaccines won't be.

42
Current method 1950’s technology Depends on eggs and chicks
Shortages often due to problems here Requires 4-6 months for vaccine production *One current vaccine in trials now uses traditional technology. At a minimum and that’s beginning production after ~2 months to prepare the virus – total 6-8 months to begin production. It will take longer to produce enough to reach risk groups.

43
Pandemic wave mortality

44
New method Cell cultures Less room More dependable
Requires 4-6 weeks for vaccine production Cell culture – a new way to grow the old method. No eggs and sacrificing embryos Reduces time for start of production from 6-8 mos to 4-6 weeks Vical also uses cell culture technology However, cell culture technology is complex and potentially longer than egg-based 6-8 mos. DNA DNA technique breaks down the virus allowing scientists to pick and choose components to be used as antigens whereas traditional methods use the whole virus either live engineered to be less virulent or severe or an inactivated virus. The antigens the human immune system responds to are the surface antigens – the H and N – that mutate almost annually. DNA technology allows for introduction of specific components, in this case the M2 protein which is internal and which rarely mutates. Vical, a pharmaceutical research lab in San Diego received 2.6M from the government on 6/6/06 to assist in completing its animal trials soon and begin phase 1 human trials of its DNA vaccine in collaboration with Sts Judes Hosp. Is testing a DNA vaccine based on both the HA and NA surface proteins which mutate easily & M2 protein and another internal protein which are “conserved” proteins that do not mutate significantly over time. What does this mean? That an H5N1 vaccine made from the strain currently transmissible from birds to humans using the NA & M2 proteins would be effective against H5N1 that mutates to be easily transmissible between humans. What else? It means that a super vaccine could be produced to provide long acting immunity to all current human strains. Animal studies show some unintended cross protection to seasonal strains even with this H5N1 strain only. Bacterial fermentation DNA of interest is inserted into E.coli bacteria. Bacteria are allowed to grow and replicate in a fermentation vat. As the bacteria replicate, the DNA is copied. The genes of interest are removed and combined with an agent that increases the ability of the vaccine to elicit an immune response. Extremely easy Produce large quantities quickly = estimated significantly less than the 6 months targeted and in sufficient quantity for the population in short order. The exciting thing is that this will be moving to clinical trials shortly

45
Vaccine Consumption I’ve identified mismatch of produced vaccine with circulating virus as the first issue and time for production as the second. The third is that 70% of vaccine production in Europe; 90% of use in US. Some experts predict that the only vaccine that will be available to a region during a pandemic is what is produced in that region. During a pandemic when travel is restricted and countries are panicking, what are the chances that those who produce will get vaccine to those who purchase? The federal government has been pumping $$$ into the effort – I mentioned Sanofi pasteur in Pennsylvania just opening – we built the plant with tax $$. May 2006 – over $!B in a new emergency funding was divided between 5 vaccine companies to build, do research in vaccine methods, and produce vaccine in the US> Source: WHO Global Influenza Program

46
Vaccine Production Capacity
Green in the US is a new Sanofi Pasteur plant in Pennsylvania that opened last year. The administration aiming to have 600 million flu vaccine doses available within six months of a pandemic, two for every American. To meet this target, the US Health and Human Services Department (HHS) is looking to diversify the production of influenza vaccines by using cell-based vaccine manufacturing, and also to have more of such manufacturing take place in American territory. Toward this end, last week, the govmt funded 6 companies to open production facilities in he US.
 is looking to diversify the production of influenza vaccines by using cell-based vaccine manufacturing, and also to have more of such manufacturing take place in American territory. Toward this end, last week, the govmt funded 6 companies to open production facilities in he US.")
47
Texas Plan Challenges In Health Systems Response
Assuring essential workers are prophylaxed and/or vaccinated Surge Capacity Emergency Systems for Advance Registration of Volunteer Health Professionals Program (ESAR-VHP) Availability of PPE Disaster Mental Health Dead bodies ESSENTIAL WORKERS In a coordinated manner (many independent entities- example major metro areas developing their own plans independently ESAR-VHP Redundancy is not helpful here – e.g., nurses on multiple volunteer lists such and American Red Cross, TX Ready Nurse, etc. Personal Protective Equipment Cost Disaster Mental Health Funding Available staff (surge capacity) SURGE CAPACITY # hospital beds vs # staffed beds Health care worker availability
 Availability of PPE. Disaster Mental Health. Dead bodies. ESSENTIAL WORKERS. In a coordinated manner (many independent entities- example major metro areas developing their own plans independently. ESAR-VHP. Redundancy is not helpful here – e.g., nurses on multiple volunteer lists such and American Red Cross, TX Ready Nurse, etc. Personal Protective Equipment. Cost. Disaster Mental Health. Funding. Available staff (surge capacity) SURGE CAPACITY. # hospital beds vs # staffed beds. Health care worker availability.")
48
Texas Plan Challenges In Communication
Risk Communication Pre-event message preparation for the public Educating decision makers Communication technology Interoperability RISK COMMUNICATION What messages are developed at the federal – state – local levels and attempting to eliminate mixed messages How to start preparing the public without eliciting panic and fear Consider what you might do to educate through the PTA or take-home messages for the kids. Your school nurse should be a resource for you. PRE-EVENT MESSAGE PREP Providing shelf-kits with messages prepared in advance costs $ Communication technology Keeping up with new technology and staff training Redundant systems Interoperability Systems interacting with systems w/o special effort on the part of the consumer Mixing software Educating decision makers If you have identified any issues relating to PI and school which need school board or legislative approval, get it taken care of early.

49
How can you prepare? Visit the DSHS website at: www.dshs/state/tx/us
Follow the Pandemic Influenza link to the state’s plan. Appendix F “Personal Protective Strategies

50
How can you prepare? Get seasonal flu vaccine Stay informed
Stockpile supplies, food, & some $$ Talk to MD and RPh about extra routine meds Don’t forget pets Have a family plan Know your business’ continuity plan

51
Websites http://www.pandemicflu.gov http://www.cidrap.umn.edu/cidrap/
Center for Infectious Disease Research and Policy, (Univ. of Minnesotta) Avian Flu and Pandemic Flu
 Avian Flu and Pandemic Flu.")
52
Planning Takes Partnerships

53
Considerations in School Planning
▶THE ROLES OF SCHOOLS IN THE COMMUNITY ▶ COMMUNICATING/COORDINATING WITH PUBLIC HEALTH/GOVERNMENT OFFICIALS ▶ UPDATING SCHOOL CRISIS PLANS ▶ LEARNING ABOUT PREVENTING INFECTIONS ▶ EDUCATING PARENTS, KIDS, STAFF ▶ INFORMING/COUNTERING DISINFORMATION ▶ MAINTAINING THE LEARNING ENVIRONMENT

54
Local Planning Is Critical
Planning must be broad/interactive/cross-cutting/coordinated: city government, civil agencies health departments, community centers, medical providers, businesses, schools, private/voluntary/faith based organizations

55
Resources to Assist in Crisis Planning

56
Federal and State Resources Focus on Local Planning

57
Mitigation and Prevention Activities
►Liaison with state/local health officials ►Clear Roles/responsibilities of staff ►Roles of school nurses ►Assign key roles ►Review health needs of students ►Improve health activities

58
Pandemic Preparedness
►Update crisis plans ►Educate staff, students & parents ►Account for Procedures ►Delegate Crisis Communication/Authority

59
Local School Considerations
►Maintain operations & the learning environment ►Triage/isolate students and staff ►Use good health practices: handwashing, disinfect, etc. ►Address misinformation ►Plan for school closure ►Disseminate community information ► Utilize schools as clinics, hospitals, morgues, vaccination sites or vaccine storage sites

60
School Houses were turned into temporary hospitals during the 1918 Influenza Pandemic

61
Pandemic Recovery Period
► Allocate time for recovery ► Involve kids & parents ► Counsel ► Debrief ► Plan anniversaries ► Facility remediation

62
School Specific Websites
63
Questions?

Similar presentations