Download presentation
Presentation is loading. Please wait.

1
High reliability healthcare: how much choice can we afford?
David Mudd Head of Modernisation North West London SHA 4 August 2004

2
In this session you can see comparisons of reliability in healthcare and other industries; look at how to design for better reliability; look at the benefits and costs of high reliability organisations; think about how you can improve the reliability of your service

3
The basics Joined-up services - as seen by users Shared information
Choice – providers, settings, date and time Redesigned, streamlined services – fewer visits, no avoidable waits Better working lives for NHS staff

4
Higher expectations over time, the basics get taken for granted
then we expect high reliability examples – cars, TVs, food industry, civil aviation, nuclear industry

5
High reliability healthcare Don Berwick, Tom Nolan
Reliability = number or % of actions that achieve the intended results “Getting it right, every time”

6
Healthcare process reliabilities
Reliability Unreliability One in.…goes wrong Process/outcome 90% 10%/10-1 10 Beta-blockers to prevent MI 99% 1%/10-2 100 Polypharmacy in the elderly Medication harm Deaths in risky surgery 99.9% 0.1%/10-3 1,000 Neonatal mortality General Surgery deaths 99.99% 0.01%/10-4 10,000 Deaths in routine anaesthesia 99.999% 0.001%/10-5 100,000 Deaths from major radiotherapy machine failures

7
Reliability in healthcare and other industries (Amalberti; Espinosa & Nolan)
ED reading X-rays (97%) Blood transfusion ED reading X-rays - improved (99.7%) Anaesthesia ASA1 Fatal iatrogenic adverse events Cardiac surgery (Patient ASA 3-5) Civil aviation Medical risk (total) Railways - France Himalaya mountaineering Road safety Chemical industry (Europe) Nuclear power industry 10-2 10-3 10-5 10-6 10-4 Very unsafe Ultra-safe
 Blood transfusion. ED reading X-rays - improved (99.7%) Anaesthesia ASA1. Fatal iatrogenic adverse events. Cardiac surgery (Patient ASA 3-5) Civil aviation. Medical risk (total) Railways - France. Himalaya mountaineering. Road safety. Chemical industry (Europe) Nuclear power industry Very unsafe. Ultra-safe.")
8
Design for Reliability (Berwick & Nolan)
Level 1: Intent, vigilance and hard work Level 2: Design informed by reliability science and research in human factors Level 3: Design of high reliability organisations

9
Level 1: “Intent, vigilance, hard work”
Standardized protocols, feedback, training, checklists Guidelines easy; getting people to follow them is difficult But: good evidence exists that this will get you to (99%)
")
10
Group discussion (5 mins)
Recall an experience – in any setting – in which the request that you ‘try harder’, ‘be careful’, or ‘stay alert’ improved your performance. Why did that work? Identify a process in your workplace that relies on vigilance. What would you estimate its reliability to be?

11
Factors affecting human vigilance
Fatigue Environmental conditions Task design Psychological conditions Competing demands

12
Level 2: Design informed by reliability science and research in human factors
Redesign the system; don’t rely on checking Decision aids and reminders built into the system; automation;evidence as the default; redundancy; scheduling; connection to habits Can take you from (99%) to (99.9%)
 to 10-3 (99.9%)")
13
Three-level design of safe and reliable systems: Prevent – Identify - Mitigate (Norman)
Design the system to prevent failure Design the system to make failures visible if they do occur Design procedures to mitigate the harm caused if failures are not detected and intercepted

14
Physical design, human behaviour (Norman)
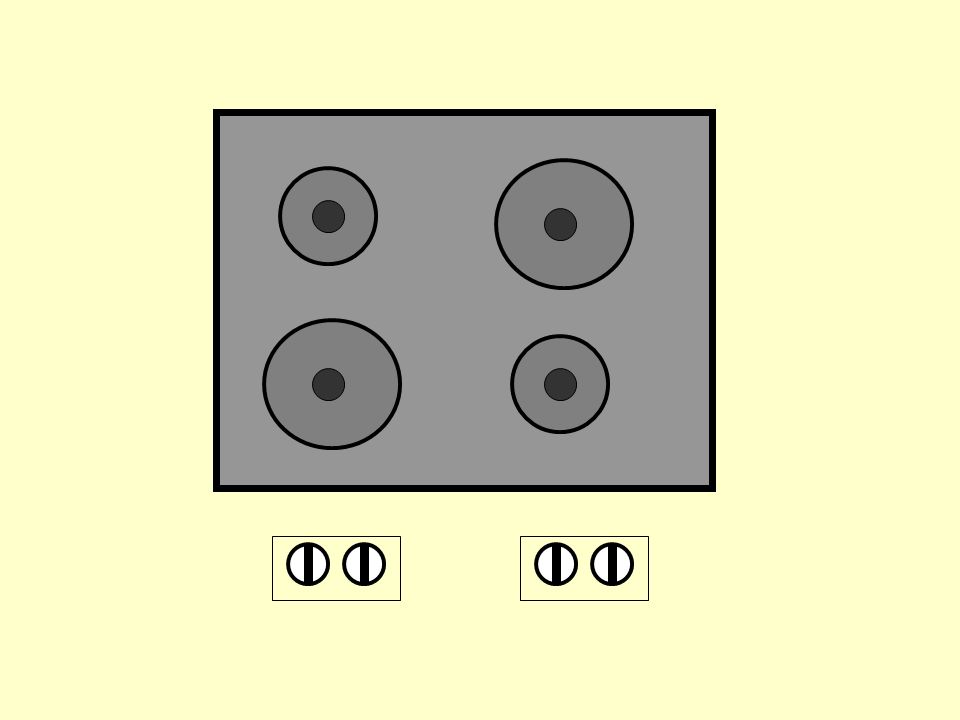
Constraints physical (eg square peg round hole) cultural (eg Red for Stop) Memory eg numbers, passwords, dates Mapping eg my cooker
 cultural (eg Red for Stop) Memory. eg numbers, passwords, dates. Mapping. eg my cooker.")
15
Natural mapping – my cooker (Norman)
")
19
Advantages of automation
Increased capacity and productivity Reduction of manual workload and fatigue Relief from routine operations Relief from small errors More precise handling of routine operations Economical utilisation of machines Damping of small differences

20
Disadvantages of automation
Seen as dehumanising – lower job satisfaction Low alertness of human operators Systems are fault intolerant – may lead to larger errors Silent failures Lower proficiency of human operators Over-reliance – complacency, uncritical acceptance of results False alarms

21
Computers are incredibly fast, accurate and stupid; humans are incredibly slow, inaccurate and brilliant; together they are powerful beyond imagination Albert Einstein

22
What’s the contribution of IM&T in healthcare?
Shared electronic record – one set of data, available to all Protocol-driven care as the default – standardising on best practice Decision aids Scheduling Making errors visible and retrievable Letting every player see the whole system

24
Level 3: Design of high reliability organisations: “ultra-safe” (Weick; Amalberti)
Accepting limits on discretionary actions (eg pilots told when it’s safe to take off/land) max safety up to 10-2 Abandoning autonomy (eg drive on the left) max safety up to 10-3 Moving from ‘craftsmanship’ to ‘equivalent actor’ (eg anaesthetics v surgery) max safety up to 10-4 Sharing the residual risk – how the system deals with failure (eg KAL 007) max safety up to 10-5 Managing the invisibility of risk (“we’ve never seen one of these before” max safety up to 10-6
 max safety up to Abandoning autonomy (eg drive on the left) max safety up to Moving from ‘craftsmanship’ to ‘equivalent actor’ (eg anaesthetics v surgery) max safety up to Sharing the residual risk – how the system deals with failure (eg KAL 007) max safety up to Managing the invisibility of risk ( we’ve never seen one of these before max safety up to")
25
Some outcomes of focus for a high reliability healthcare organisation (Berwick)
No needless deaths No needless pain No feelings of helplessness No unnecessary waiting No waste

26
Constraints Constraints on patient choice
Constraints on professional autonomy Constraints on the factors which distinguish healthcare organisations (competitive advantage)
")
27
Challenges Buy-in from clinicians and patients
Protocol-driven care as the default – standardising on best practice Sharing information – with whom? Decision aids or decision-taking? Scheduling – are we ready for it? Making errors visible and retrievable – aligning the incentives and penalties

28
Summary Reliability in healthcare is a long way behind other safety-critical industries We can improve reliability by better design equipment and systems, and by standardisation Beyond this, improvement comes with reduced choice – standardisation/doing it by the book Clinicians need to work with standardisation, but be prepared to respond with autonomy Sophisticated design of human interactions and working relationships

29
Table discussion Think about the clinical service you provide/manage:
What changes must you make to get to 10-4 performance? What implications does this have for how you select and train your staff?

30
References/further reading
The Design of Everyday Things. Donald A Norman; MIT Press; 1998 Handbook of Human Factors and Ergonomics. G Salvendy (ed); John Wiley, New York; 1997 Managing the Unexpected. Weick and Sutcliffe; Josey Bass; 2001 System changes to improve patient safety. Nolan TW. BrMedJ 2000;320: (18 March) Reducing errors made by emergency physicians in interpreting radiographs: longitudinal study. Espinosa JA, Nolan TW. BrMedJ 2000; 320: (18 March) The quality of care delivered to adults in the United States. McGlynn EA, Asch SM, et al. N Engl J Med, 348(26); June 2003 Revisitjng safety and human factors paradigms to meet the safety challenges of ultra complex and safe systems. Amalberti R, In Challenges and pitfalls of safety interventions, Willpert B & Fahlbruch B. Elsevier, North Holland Wiener EL, Nagel DC, ed. Human Factors in Aviation. New York: Academic Press, 1988. Various presentations & papers by Rene Amalberti on the Internet (via Google)
; John Wiley, New York; Managing the Unexpected. Weick and Sutcliffe; Josey Bass; System changes to improve patient safety. Nolan TW. BrMedJ 2000;320: (18 March) Reducing errors made by emergency physicians in interpreting radiographs: longitudinal study. Espinosa JA, Nolan TW. BrMedJ 2000; 320: (18 March) The quality of care delivered to adults in the United States. McGlynn EA, Asch SM, et al. N Engl J Med, 348(26); June Revisitjng safety and human factors paradigms to meet the safety challenges of ultra complex and safe systems. Amalberti R, In Challenges and pitfalls of safety interventions, Willpert B & Fahlbruch B. Elsevier, North Holland. Wiener EL, Nagel DC, ed. Human Factors in Aviation. New York: Academic Press, Various presentations & papers by Rene Amalberti on the Internet (via Google)")
Similar presentations



 Reporting systems are vital in providing a core of sound, representative information on which to base analysis.>")








 was developed by Johns Hopkins University, funded by the Department of Health.>")








