Download presentation
Presentation is loading. Please wait.

2
NatPaCT works with Primary & Care Trusts
to help them learn & grow together, as connected and competent organisations and leaders of radical change to improve health & services for patients.

3
Chronic Eye Disease Management in Community Settings:
First Report of the Eye Care Services Steering Group

4
Bob Ricketts Head of Access Policy Development & Capacity Planning Department of Health

5
Head of Dental and Optical Commissioning Group
David Hewlett Head of Dental and Optical Commissioning Group

6
Minister of State Department of Health
Rosie Winterton MP Minister of State Department of Health

7
Blindness: Vision 2020 - The Global
Initiative for the Elimination of Avoidable Blindness disease prevention and control training of personnel strengthening of the existing eye care infrastructure use of appropriate and affordable technology mobilisation of resources

8
NHS PLAN Core Principles 3,4,8
The NHS will shape its services around the needs and preferences of individual patients, their families and their carers The NHS will respond to different needs of different populations The NHS will work together with others to ensure a seamless service for patients

9
“Fair for all and personal to you” John Reid 16 July 2003

10
Eye Care Services Steering Group
Set up by Ministers in December 2002 Worked on GMS, dentistry and pharmacy and ophthalmics now moving forward Growing need for eyecare services and major quality of life issues

11
Source ONS Source ONS Source ONS

12
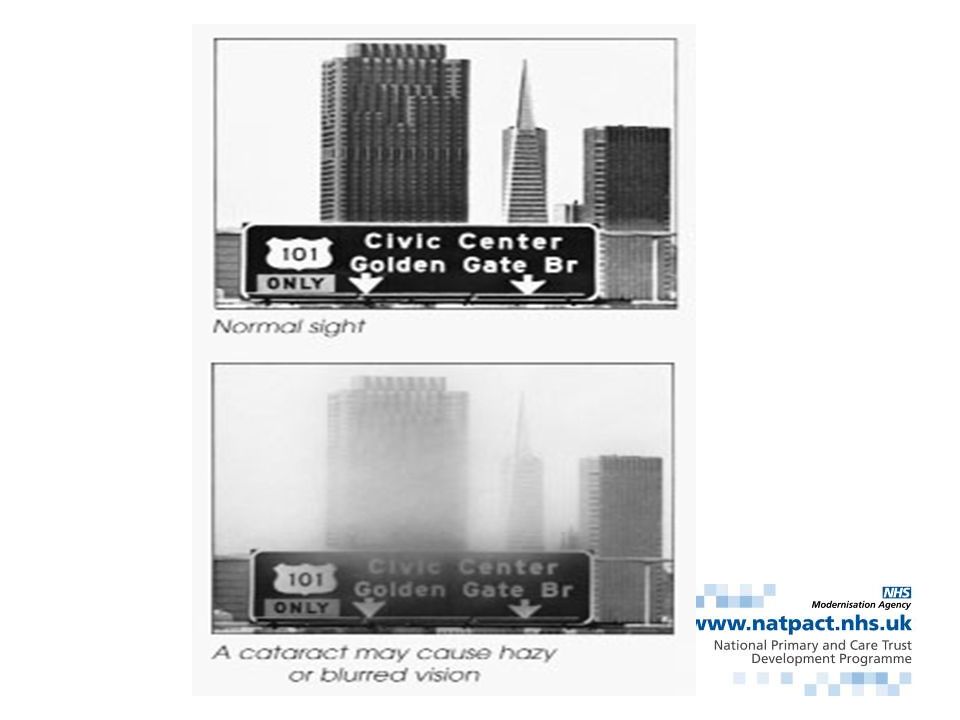
Half of over 65s have impaired vision in one or both eyes
Increase in elderly

13
Four Pathways Cataract Glaucoma
Age Related Macular Degeneration (ARMD) Low Vision Services Diabetic retinopathy being tackled separately as part of Diabetes NSF
 Low Vision Services. Diabetic retinopathy being tackled separately as part of Diabetes NSF.")
14
Design Principles Make best use of available resources
Have fewer steps for the user Make more effective use of professional resource Show a high standard of clinical care with good outcomes Improve access and deliver greater patient choice Evidence based

15
Conclusions Primary care ophthalmic services need to be developed to meet demographic demand Partnerships with primary & secondary care, patients and carers essential Integrated IT needed but not prerequisite Voluntary agency and social services involvement important

16
Care Pathways Designed to Achieve:
Integrated eye care services Better use of skills in primary care Increased amount of care for all in accessible primary care settings Increased role for professional groups in primary care

17
Recommendations Cataract pathway to be implemented when waiting times reduced to 3 months £73million additional funding to achieve 3 month cataract waits by December 2004 Glaucoma pathway to be piloted initially ARMD and Low Vision to be taken forward within existing funds £4million for innovative projects and pilots GOS Regulations to be amended to allow direct referral by optometrists

18
Why are we here? Share our report with you Consider, if you agree with us, how we take it forward together

20
Director Association of Optometrists & Chair, Cataract Working Group
Elizabeth Frost Director Association of Optometrists & Chair, Cataract Working Group

22
Background Mainly elderly population
Many misconceptions about cataract surgery Changes in HES Action on Cataracts

23
Current Cataract Pathway
Patient reports sight problem to GP Patient goes to optometrist/OMP for sight test and optometrist/OMP refers patient to GP Patient goes to GP, referred to HES Patient seen at HES, cataract confirmed, decision to operate, and put on waiting list Patient attends HES for pre-op assessment Patient attends HES for day case surgery Patient attends HES for 24 hr check Patient attends HES for 6 week check, 2nd eye discussed Patient attends optometrist/OMP for sight test and new specs.

24
Proposed Cataract Pathway
Patient attends optometrist/OMP for sight test, cataract diagnosed and discussed, general risks & benefits of surgery explained, current medication listed, patient information given, and appointment made for HES, with choice of provider (copy of referral to GP for info) Patient attends HES to see ophthalmologist and for pre-op assessment Patient attends HES for day case surgery Patient attends HES/optometrist/OMP for 24/48 hr check OR is phoned by cataract nurse to check progress (agreed locally) Patient attends optometrist/OMP for final check and sight test, 2nd eye discussed.
 Patient attends HES to see ophthalmologist and for pre-op assessment. Patient attends HES for day case surgery. Patient attends HES/optometrist/OMP for 24/48 hr check OR is phoned by cataract nurse to check progress (agreed locally) Patient attends optometrist/OMP for final check and sight test, 2nd eye discussed.")
25
Proposed Cataract Pathway
Start Finish 1. Patient attends optometrist Sight test, cataract diagnosed and discussed General risks and benefits of surgery discussed Patient wishes to proceed, information given etc Patient offered choice of hospital and appointment agreed 4. Patient attends HES or Optometrist Final check Sight test Discharged or 2nd eye discussed and appointment arranged 2. Patient attends HES Outpatient appointment with ophthalmologist* pre-assessment (with nurse?) Date for surgery arranged/agreed (* details of medication etc received from optometrist, GP or patient as per local protocols ) 3. Patient attends HES Day case surgery undertaken
 Date for surgery arranged/agreed. (* details of medication etc. received from optometrist, GP or. patient as per local protocols ) 3. Patient attends HES. Day case surgery undertaken.")
26
Who should be referred? Not a ‘fast track’ service
Suitable for those who – have a cataract that is interfering with their daily living have been given basic information about cataract surgery, and risks / benefits want to have surgery

27
Evidence of Success Several services developed and audited
90%+ referrals proceeding to surgery cf 80% for traditional referrals Reduced time to surgery from 12 to 3 months Surgical outcomes meet RCO guidelines Reduced DNA rates Greater nurse involvement High patient satisfaction

28
Constraints to Success
Not funded centrally through GOS budget To be funded by existing PCT budgets Investment needed in equipment and staffing Needs mutual inter-professional trust and teamwork Lack of IT booking links will hamper

29
Key Recommendations for local action
Reduce number of steps in pathway Eliminate duplication Improve IT links – optometrist/OMP/HES Develop protocols for discharge from HES to optometrist/OMP with audit feedback Agree funding

31
Royal College of Ophthalmologists & Chair, Glaucoma Working Group
Stephen Vernon Royal College of Ophthalmologists & Chair, Glaucoma Working Group

32
Chronic Glaucoma gives tunnel vision
10 years

34
Testing for glaucoma

35
UK population by age Age range

36
BMES PREVALENCE OF POAG
< >80 Age Group

37
Estimated numbers of glaucomas in UK by age (1000s)
")
38
Current Glaucoma Pathway (Hospital Based Care)
Single screening opportunity by community optometrists with no standardised protocols Diagnosis and continued care for life of all glaucoma (and many suspects) within Hospital Eye Service by ophthalmologists
 within Hospital Eye Service by ophthalmologists.")
39
Proposed Pathway (Community Based Care)
Community optometrists work to nationally agreed screening protocols which permit refinement of tests prior to referral Glaucoma suspects and stable glaucoma patients managed in the community by COs and OMPs with interaction of community and HES teams where appropriate

40
The 5 Care Pathways Care Pathway 1 Ocular Hypertension Care Pathway 2
Glaucoma without other eye disease Care Pathway 3 Glaucoma suspect on discs and/or fields Care Pathway 4 Glaucoma in presence of other significant eye disease Care Pathway 5 Refinement of community optometric referrals

41
Proposed Glaucoma Pathway
Start 1. Patient attends community optometrist (CO) Sight test, IOP over 21 (applanation tonometry) and/or visual field defect and/or excavated discs Patient/optometrist makes appointment with optometrist with special interest in glaucoma (OSI) or OMP 4. OSI/OMP manages patient in community setting Regular reviews set in place OSI/OMP relay data to hospital if significant progression for HES review if needed 2. Patient attends OSI or OMP Full history and assessment carried out according to protocol Decision taken as to whether patient has ocular hypertension (OSI/OMP reviews) or can be discharged (return to CO) or has glaucoma (treat or refer to HES) Patient advised, given information etc and further appropriate appointments made if needed 3. OSI/OMP relays data to HES HES reviews data, advises OSI/OMP regarding management and sets up review at HES if needed
 Sight test, IOP over 21 (applanation tonometry) and/or visual field defect and/or excavated discs. Patient/optometrist makes appointment with optometrist with special interest in glaucoma (OSI) or OMP. 4. OSI/OMP manages patient in community setting. Regular reviews set in place. OSI/OMP relay data to hospital if significant progression for HES review if needed. 2. Patient attends OSI or OMP. Full history and assessment carried out according to protocol. Decision taken as to whether patient has ocular hypertension (OSI/OMP reviews) or can be discharged (return to CO) or has glaucoma (treat or refer to HES) Patient advised, given information etc and further appropriate appointments made if needed. 3. OSI/OMP relays data to HES. HES reviews data, advises OSI/OMP regarding management and sets up review at HES if needed.")
42
Evidence Base Only 33% of suspect glaucoma referrals found to have glaucoma by HES Optometrists with additional training can assist in glaucoma management freeing up ophthalmologist and hospital time Refinement of referrals for suspect glaucoma by specially trained optometrists reduces HES referrals

43
Constraints to Achievement
Funding issues - increased revenue costs Training requirements Legal issues for prescribing rights Information Technology issues Communication Record keeping Audit

44
Key Recommendations for Local Action
Community optometrists conform to College guidelines for referral of glaucoma suspects HES services utilise optometrists to assist in glaucoma care within the HES Community refinement of optometric referrals established utilising OMPs and optometrists with a special interest in glaucoma Community care of “straightforward” glaucoma cases by OMPs and optometrists with a special interest in glaucoma

46
President College of Optometrists & Chair, ARMD Working Group
Frank Munro President College of Optometrists & Chair, ARMD Working Group

47
OBJECTIVES Map out the current care pathway
Identify inhibitors & barriers to change Identify areas for improvement Develop proposals for a new integrated care pathway for patients with ARMD

48
WHAT IS AGE RELATED MACULAR DEGENERATION(ARMD)?
Acquired condition - > over 60 years ‘Wet’ & ‘Dry’ forms Affects central vision Almost 1 million in England Commonest cause of irremediable visual loss Accounts for 14% blind & partially sighted registrations ( 50% for those > 65yrs) Limited credible treatment options
 Limited credible treatment options.")
49
ASSOCIATION BETWEEN VISUAL IMPAIRMENT &…..
Increased mortality Increased morbidity / falls / fractures Increased road accidents Increased anxiety & depression Poorer self care & independence Greater need for community & institutional resources Social isolation - quality of life Loss of income

50
DEMOGRAPHICS AMD 1998 approximately 8.3
By 2020 A 25% increase in the over 65 population is expected Incidence of ARMD expected to rise by 31% AMD 1998 approximately 8.3 on people over the age of 65 in England and Wales 4.3 million have impaired vision AMD is the leading cause in over 65s

51
AMD: A Growing Problem Burden recognised by government
NSF for Older People Vision impairment is an intrinsic risk factor for falls NICE: Recent guidance on PDT for wet-AMD NICE to review new treatments in 2005 In meeting future demand, service will have to respond to increasing patient numbers and delivering new therapies

52
Current Services There are many good points about today’s services:
Access to angiography in most (if not all) eye departments Access to Argon laser in all eye departments Great awareness of AMD in general optical services Prompt access for suspected wet AMD in most secondary care sites In some centres access to LVA, LV1, social services advice is almost one stop
 eye departments. Access to Argon laser in all eye departments. Great awareness of AMD in general optical services. Prompt access for suspected wet AMD in most secondary care sites. In some centres access to LVA, LV1, social services advice is almost one stop.")
53
Current ARMD Pathway Patient reports visual problem
GP refers patient to HES OR Patient is referred to an optometrist ARMD is diagnosed Patient is referred to HES via GP Fluorescein angiography carried out Any credible treatment option considered Patient managed by HES or by Low Vision Service Patient registered Referred for Social Service & Rehabilitation support

54
Problems with Current Services
Can be a lack of collaboration / communication between healthcare and social service providers Lack of timely diagnosis and ease of access to treatments / social services for patients with AMD

55
What do patients want from future services?
Rapid and precise diagnosis in primary care Access to medical retina specialists advice Rapid access to treatment when appropriate Access to LVA services to make best use of remaining sight Understand risk factors Improved communication between: Clinicians and patients Different service providers Further research

56
Need to Manage AMD Differently
Improve collaboration / communication between healthcare and social service providers Ensure timely diagnosis and ease of access to treatments / social services for patients with AMD

57
The ‘NEW’ AMD Pathway SELF REFERRAL
REFERRED BY ANOTHER CLINICIAN OR CARER OTHER SOURCE PATIENT PRESENTS WITH VISUAL PROBLEM AND IS EXAMINED BY COMMUNITY OPTOMETRIST IN TRIAGE CAPACITY – DIFFERENTIAL DIAGNOSIS SYMPTOMS SUGGESTIVE OF ARMD NOT ARMD APPROPRIATE CARE AS INDICATED ‘DRY’ (NON-NEOVASCULAR) ARMD ‘WET’ (NEOVASCULAR) OR SUSPECTED ‘WET’ ARMD OPTICAL / OPHTHALMIC LOW VISION SERVICES COUNSELLING SOCIAL SERVICE SUPPORT REHABILITATION BD8/LV1 AS REQUIRED DIRECT REFERRAL TO HES FOR FLUORESCEIN AGIOGRAPHY AND FURTHER INVESTIGATION UNTREATABLE ACCESS TO TREATMENT TREATABLE
 ARMD. ‘WET’ (NEOVASCULAR) OR SUSPECTED ‘WET’ ARMD. OPTICAL / OPHTHALMIC. LOW VISION SERVICES. COUNSELLING. SOCIAL SERVICE SUPPORT. REHABILITATION. BD8/LV1 AS REQUIRED. DIRECT REFERRAL TO HES FOR FLUORESCEIN AGIOGRAPHY AND. FURTHER INVESTIGATION. UNTREATABLE. ACCESS TO TREATMENT. TREATABLE.")
58
Summary of Evidence 2/3rds with vision impairment are over 65 years of age ARMD commonest cause of irremediable serious visual loss in people over 65 years of age Macular degeneration - 14% of new partial sight & blind registrations for working population (aged 16-64) Exponential increase in ARMD over the age of 75 Demographic shifts in population - increase of approximately 30% over next 20 years Reductions in contrast sensitivity, depth perception and peripheral vision linked with risk of falls or hip fracture Visual impairment important risk factor for hip fracture and falls
 Exponential increase in ARMD over the age of 75. Demographic shifts in population - increase of approximately 30% over next 20 years. Reductions in contrast sensitivity, depth perception and peripheral vision linked with risk of falls or hip fracture. Visual impairment important risk factor for hip fracture and falls.")
59
Inhibitors and Barriers
Adequate Funding – fees, IT etc Human resources / recruitment Patient / Practitioner Communication Competitive behaviour Lack of Inter Professional Collaboration Lack of patient understanding Lack of trust Poor understanding / recognition of the role of other professionals

60
Key recommendations for local action
Community optometrists encouraged to comply with College of Optometrists guidelines when examining older people Direct referral to the HES by optometrists should be introduced Care networks involving all carers established to ensure comprehensive care for all patients within an integrated structure Best possible patient care to be the clear focus of all involved

62
Elizabeth Bates Co- Director, Greater Manchester Children’s Network
& Chair Low Vision Services Working Group

63
Aim of Pathway “A growing number of the most vulnerable people in this country experience a quality of life that is significantly, but unnecessarily, diminished for the want of basic, relatively inexpensive health care” (RNIB 1999)
")
64
Key Issues Vast majority of people with low vision are over 70
Most people with low vision retain some sight Sight can be maximised by: prompt advice and counselling early assessment provision of appropriate low vision aids (LVAs) and training in their use Effective low vision services can reduce admissions to residential care
 and training in their use. Effective low vision services can reduce admissions to residential care.")
65
Current Low Vision Pathway
Fragmented Wide variation re access & quality Referral from optometrist (often via GP) to HES Uni-disciplinary Lack of information, signposting & awareness Long waiting times Initiation of LV services ONLY after ophthalmological assessment
 to HES. Uni-disciplinary. Lack of information, signposting & awareness. Long waiting times. Initiation of LV services ONLY after ophthalmological assessment.")
66
Proposed Low Vision Pathway(1)
Emphasis on low vision services not provision of low vision aids Led by Primary or Social Care Partnership Approach Providing Services which promote: Awareness Timeliness Accessible

67
Proposed Low Vision Pathway(2)
Establishment of a key worker model Registration not a pre-requisite Medical assessment not a pre-requisite Services enable re-access and re-assessment Better utilisation of relevant health & social care professionals

68
Proposed Low Vision Pathway
Start 4. Service enables re-access 1. Patient referred to Low Vision Service (LVS) Referral may be from secondary care, GP, social worker, rehabilitation officer, community nurse, OT etc or may be self referral Patient may have an LVI, RVI or CVI All patients are contacted by LVS within 10 working days 3. Patient has follow up visits as needed Visits may take place in the patient’s home or elsewhere Visit will be by appropriate member of the LV team 2. Patient attends LVS Service is seamless across health, social care and the voluntary sector A full sight test forms part of assessment Patient is given information on eye condition, entitlements etc as well as local services Counselling and advice on employment or education is available Spectacles, LV aids, advice (esp. lighting, contrast and size) and home adaptations are discussed and made available as appropriate Referral to other areas of health and social care as needed, including certification
 Referral may be from secondary care, GP, social worker, rehabilitation officer, community nurse, OT etc or may be self referral. Patient may have an LVI, RVI or CVI. All patients are contacted by LVS within 10 working days. 3. Patient has follow up visits as needed. Visits may take place in the patient’s home or elsewhere. Visit will be by appropriate member of the LV team. 2. Patient attends LVS. Service is seamless across health, social care and the voluntary sector. A full sight test forms part of assessment. Patient is given information on eye condition, entitlements etc as well as local services. Counselling and advice on employment or education is available. Spectacles, LV aids, advice (esp. lighting, contrast and size) and home adaptations are discussed and made available as appropriate. Referral to other areas of health and social care as needed, including certification.")
69
Recommendations Local Action National Action
Develop local partnership arrangements with designated lead officer/organisation Integrate LV assessment into the Single Assessment process for older people Move to provision of LV aids via a “loans” service Consider opportunities offered under the new GMS contract for LV screening National Action Develop national eligibility criteria & core standards Review existing funding streams Understand workforce implications Develop generic training programme Audit existing services

71
Benefits, Next Steps, Commissioning Options

72
Benefits for patients Better care: access speed convenience

73
Benefits for the NHS shorter waiting times better use of skills
better value for money

74
Review of General Ophthalmic Services
Department reviewing General Ophthalmic Services Currently a central budget for limited service - need to consider if that supports modernisation proposals

75
Next Steps Local commissioning and planning across sectors to deliver integrated service Pathways a resource to inform planning and provide ideas for development Flexibilities in current system allow for progress now

76
Commissioning Options
PCTs can already purchase services in primary or secondary care PCTs can joint fund with social services to deliver integrated service

79
Delivering Effective Patient Choice in Cataract Surgery
Ann Wagner Programme Director West Yorkshire Patient Choice

80
Delivering Effective Patient Choice in Cataract Surgery
Choice and wider system reform context West Yorkshire Patient Choice Cataract Pilot Opportunities and Challenges

81
What is Choice all about?
Dept of Health policy to deliver more choice and certainty to patients Starting with choice of elective care, choice will eventually be rolled out to all service areas Starting with choice of when and where, choice will be expanded to include choice of what and who Needs to be seen in context of wider system reform agenda linked to financial flows – payment by results, agenda for change, booking, e booking and NPFIT and plurality and diversity agenda. A key enabler for choice is booking and e booking

82
Choice Targets From end April 2004, patients waiting over 6 months to be offered choice of at least one alternative provider From January 2005, all cataract patients to be offered a choice of at least two providers at point of referral From April 2005, heart surgery patients to be offered choice of hospital at point cardiologist refers them to a cardiothoracic surgeon From December 2005, all patients requiring elective care to be offered choice at point of referral of 4 or 5 alternatives

84
West Yorkshire Patient Choice Cataract Pilot
Community of Interest: 15 PCTs 5 Acute Trusts 4 LOCs Host PCT with DTC capacity and capability Clinical Engagement Supportive SHA Financial support of DoH

85
West Yorkshire Patient Choice Cataract Pilot
Aim: to improve the patient experience by: Giving patients much greater influence over treatment Reduce waiting times Increase activity Improve service delivery Challenge ways of working Focus: day case cataract surgery at Westwood Park DTC

87
West Yorkshire Patient Choice Cataract Pilot
Choice Objectives: Targeting long waiters Choice in secondary care Choice in primary care To support West Yorkshire Health Community in delivering choice for all

88
West Yorkshire Patient Choice Cataract Pilot
Developing clinical and patient pathways Process mapped existing pathways and practice Benchmarked against best and recommended practice Considered options and where to put choice for greatest benefit Agreed way forward including supporting common information, referral forms, Optom fees and clinical audit

89
Where do we offer Choice and Booking?
3 mth max 3 mth max Optometrist Outpatient waiting list Inpatient/ Daycase Treatment Assessment Post Op Assessment Choice Booking Optometrist Sight Check Who offers Choice? Who makes the booking?

90
West Yorkshire Patient Choice Cataract Pilot
Opportunities: Improve the patient experience Strengthen community of interest Explore single site capacity expansion Test out national tariff Develop more effective pathway Take a proactive, patient centred approach to evaluation and peer review Pilot choice

91
West Yorkshire Patient Choice Cataract Pilot
Challenges: Corporate buy in Optometrists fees Putting choice into the pathway Loss of control Conflicting policies/ competing priorities Referral thresholds and discharge protocols Data and patient tracking Transport Not reinventing the wheel

92
“And should there be a sudden loss of consciousness during this meeting oxygen masks will drop from the ceiling”

94
Contact Details Ann Wagner Programme Director
West Yorkshire Patient Choice Tel: , E mail :

Similar presentations













 Dr Martin Connor Associate Director (Health Reform) Greater Manchester Strategic Health.>")










 has been commissioned by Ipswich and East Suffolk CCG to establish and run.>")





 And Surrey County Council.>")
