Download presentation
Presentation is loading. Please wait.

1
Running Healthy: Protecting, Preserving and Restoring Cartilage
Matthew Busam, MD Cincinnati SportsMedicine Team Physician: Elder HS

2
“If you have a body, you’re an athlete.” -Bill Bowerman

3
Goals Review evidence concerning running and arthritis
Review supplements Review “cortisone” injections Review signs and symptoms of when we ask our patients to stop running and consider further evaluation Surgical advances in articular cartilage injuries

4
Benefits of running Physical Psychological Cardiovascular
Weight management Intellectual? – regular exercise can improve cognition (at least in mice) Maintenance of bone mineral density Protective effect for joints? Psychological
 Maintenance of bone mineral density. Protective effect for joints Psychological.")
5
Adverse effects Injuries 30% of “serious distance runners”
>25 miles per week will be injured in a given year 30% of these injuries involve the knee

6
Running & Arthritis Does running cause arthritis? NO!

7
But what about…? Anecdotal evidence for just about anything. No proven relationship implicating running with development or progression of osteoarthritis

8
Examples JAMA Mar 7;255(9): Lane NE, Bloch DA, Jones HH, Marshall WH Jr, Wood PD, Fries JF Long-distance running, bone density, and osteoarthritis. Running is associated with increased bone mineral but not, in this cross-sectional study, with clinical osteoarthritis

9
Evidence J Rheumatol Mar;20(3):461-8. Lane NE, Michel B, Bjorkengren A, Oehlert J, Shi H, Bloch DA, Fries JF. The risk of osteoarthritis with running and aging: a 5-year longitudinal study. Running did not accelerate the development of radiographic or clinical OA of the knees

10
Curr Opin Rheumatol. 1999 Sep;11(5):413-6.
Exercise and osteoarthritis. Lane NE, Buckwalter JA. Recreational jogging in individuals 60 or more years of age with normal knee and hip joints does not increase the risk for the development of osteoarthritis.

11
Who hurts more?

12
Arthritis Res Ther. 2005;7(6):R1263-70. Epub 2005 Sep 19.
Bruce B, Fries JF, Lubeck DP. Aerobic exercise and its impact on musculoskeletal pain in older adults: a 14 year prospective, longitudinal study. Compared runners, who averaged about 26 miles a week, to a matched set of controls, who averaged about two miles a week. "If running creates damage through accumulated trauma, then runners with about ten-fold the exposure to such trauma should have increased pain over time." The runners experienced "about 25 percent less musculoskeletal pain" than the controls.

13
Long-term study: Percent Pain Increase Age Female Runners:11.8% Female Control: 70.6% Male Runners: 17.6% Male Control: 41.4%

14
Imaging Data

15
Objective Findings Am J Sports Med. 2004 Jan-Feb;32(1):55-9.
Hohmann E, Wörtler K, Imhoff AB MR imaging of the hip and knee before and after marathon Results suggest that the high impact forces in long-distance running are well tolerated and subsequently do not demonstrate changes on MR images. Eur Radiol Oct;16(10): Epub 2006 Mar 10. Schueller-Weidekamm C, Schueller G, Uffmann M, Bader TR. Does marathon running cause acute lesions of the knee? Evaluation with magnetic resonance imaging. The evaluation of lesions of the knee with MRI shows that marathon running does not cause severe, acute lesions of cartilage, ligaments, or bone marrow of the knee in well-trained runners
: Epub 2006 Mar 10. Schueller-Weidekamm C, Schueller G, Uffmann M, Bader TR. Does marathon running cause acute lesions of the knee Evaluation with magnetic resonance imaging. The evaluation of lesions of the knee with MRI shows that marathon running does not cause severe, acute lesions of cartilage, ligaments, or bone marrow of the knee in well-trained runners.")
16
Objective Findings Am J Sports Med May;36(5): Epub 2008 Feb 20. Kessler MA, Glaser C, Tittel S, Reiser M, Imhoff AB. Recovery of the menisci and articular cartilage of runners after cessation of exercise: additional aspects of in vivo investigation based on 3-dimensional magnetic resonance imaging. Recovery period of 1 hour, articular structures returned to normal

17
Objective findings Skeletal Radiol Jul;37(7): Epub 2008 May 16. Krampla WW, Newrkla SP, Kroener AH, Hruby WF Changes on magnetic resonance tomography in the knee joints of marathon runners: a 10-year longitudinal study Loads experienced in marathon running do not cause permanent damage in the internal structures of the knee. A disposition for premature arthrosis was not registered in the population investigated.

18
Causes of knee pain in runners
Anterior knee pain Lateral pressure syndrome Patella instability Extensor mechanism tendinopathy Others Meniscus Focal chondral defects OA Bursitis Stress fracture ITB Popliteal tenosynovitis Ligamentous instability

19
Treatment: Where to intervene
Training programs Anatomy, biomechanics Shoes, orthotics Muscles: weakness, imbalance Physical therapy Medication Surgery Rehab

20
Where to Start? The best way to protect the knees of runners is with regular stretching and strengthening exercises…in addition to running!

21
Quads and Hamstrings Patellofemoral pain Anterior knee pain
“Runners Knee”

22
Runners are tough, but weak!
Running does not produce strength It produces endurance Weakness leads to imbalance pain and injury

23
Closed chain quad rehab

24
Iliotibial Band Streching/Strengthening

25
Stretching

26
Strengthen

27
Shoes Am J Sports Med Dec;34(12): Butler RJ, Davis IS, Hamill J. Interaction of arch type and footwear on running mechanics. Running footwear recommendations should be based on an individual's running mechanics. If not available, footwear recommendations can be based arch type.

28
Shoes Midsoles wear out before outsoles
If outsole is worn, midsole is likely worse! Mileage estimates are really just guesses, but usually 300 miles is time for new footwear Unless pt is a very efficient, lightweight runner

29
Running through Injury
Yes, No, and Maybe Yes for shin splints No for stress fractures No when swelling is present

30
Return from Injury

31
Graduated return to sport program
Prolonged process Start slow Gradually increase time and distance Then focus on speed

32
What about regrowing cartilage?

33
Supplements “Patented ingredients help support, ease, and rebuild joints….” “Soothe away joint pain and watch as your skin regains a nourished, youthful appearance….” “It’s like oil for your joints—it helps promote full range of motion and flexibility.” “New Miracle Relief Formula eliminates even the worst pain...almost instantly!”

34
What is a Supplement? U.S. Food and Drug Administration (FDA)
dietary supplements: subcategory of “food,” providing manufacturers with greater leeway and less oversight than products in the pharmaceutical category Asterisk syndrome: product is advertised to promote and maintain “joint strength,* joint flexibility,* joint lubrication,* range of motion,* production of lubricating fluid,* and renewal of cartilage and connective tissue.*” “*These statements have not been evaluated by the Food and Drug Administration. This product is not intended to diagnose, treat, cure, or prevent any disease.”

35
Glucosamine “highly significant efficacy” for all outcomes, including joint space narrowing and Western Ontario MacMaster University Osteoarthritis Index (WOMAC). Structural and Symptomatic Efficacy of Glucosamine and Chondroitin in Knee Osteoarthritis A Comprehensive Meta-analysis Florent Richy, MSc; Olivier Bruyere, MSc; Olivier Ethgen, MSc; Michel Cucherat, MSc, PhD; Yves Henrotin, MSc, PhD; Jean-Yves Reginster, MD, PhD Arch Intern Med. 2003;163:
. Structural and Symptomatic Efficacy of Glucosamine and Chondroitin in Knee Osteoarthritis A Comprehensive Meta-analysis. Florent Richy, MSc; Olivier Bruyere, MSc; Olivier Ethgen, MSc; Michel Cucherat, MSc, PhD; Yves Henrotin, MSc, PhD; Jean-Yves Reginster, MD, PhD. Arch Intern Med. 2003;163:")
36
Glucosamine & Chondroitin
GA stimulates production of collagen and its precursors. It may also have an antiinflammatory role. CS inhibits enzymes that break down cartilage. It also adds to the pool of molecules that form collagen. The combination of these compounds is considered to enhance cartilage protection.

37
Glucosamine Another study reported on 1,583 patients with symptomatic knee osteoarthritis who were randomly assigned to take glucosamine, chondroitin, a combination of glucosamine and chondroitin, celecoxib, or placebo over 24 weeks. Overall rate of response to glucosamine, chondroitin, and the combination were not found to be significantly better than placebo, although patients with moderate to severe pain at baseline were observed to respond significantly better with the combination. N Engl J Med Feb 23;354(8):
:")
38
Glucosamine: Side effects
Primary side effects: mild gastrointestinal complaints such as constipation, diarrhea, cramping, gas, heartburn, and nausea. Glucosamine sulfate has been associated with drowsiness and headache. The effects of glucosamine on nursing or pregnant women have not been well-studied. Glucosamine may increase blood sugar levels. Although studies of glucosamine on patients with diabetes are inconclusive, it is believed that higher doses may prompt the pancreas to produce less insulin, so caution is advised. Because glucosamine is often made from shellfish and the source of the product is not required to be on the label, individuals who are allergic to seafood are advised to exercise caution as well

39
Chondroitin Study participants have generally reported a decrease in pain and increases in joint movement when taking chondroitin, although it is not uncommon for participants to take chondroitin in combination with aspirin or other conventional arthritis treatments, so the true extent of the efficacy of chondroitin remain unclear. Some studies seem to show that chondroitin must be taken for up to 4 months before benefits are realized. A recent 24-week trial of 279 patients found no significant difference between chondroitin and placebo as far as the study’s primary efficacy criteria (pain on daily activities and Lequesne’s index) were concerned
 were concerned.")
40
Chondroitin Primary side effects: uncommon and include hair loss and minor gastrointestinal complaints. The effects of chondroitin on nursing or pregnant women have not been well-studied. Chondroitin can decrease the blood’s ability to clot, and it is not advisable to take it concurrently with aspirin, antiplatelet, or anticoagulant drugs. Chondroitin products are also sometimes combined with manganese, which may assist in cartilage production, but is toxic in large doses. The U.S. National Academy of Sciences has set the adult tolerable upper limit for manganese at 11 mg/day; patients should be advised not to exceed that level.

41
MSM Methylsulfonylmethane (MSM)
Treatment for a variety of conditions from osteoarthritis to stress and snoring. Few clinical trials examine the supplement’s efficacy for osteoarthritis. Evidence for this is spotty at best

42
Omega-3 Shark Cartilage
Little clinical evidence exists to support assertions that omega-3s are effective against arthritis. Shark Cartilage No proof that taking a shark cartilage supplement provides benefits. No studies have been conducted to determine whether shark cartilage has any serious or long-term side effects

43
Supplements Overall Of the commonly available supplements, glucosamine, chondroitin, or a combination of the two appear to have the greatest efficacy based on clinical trials, but a number of researchers remain guarded even when recommending those products If less than 120 lbs: GA 1000mg + CS 800mg (1 tab twice a day) Between : GA 1500mg + CS 1200mg (2 tabs in morning and 1 tab in afternoon) If greater than 200: GA 2000mg + CS 1600mg (2 tabs twice a day)
 Between : GA 1500mg + CS 1200mg (2 tabs in morning and 1 tab in afternoon) If greater than 200: GA 2000mg + CS 1600mg (2 tabs twice a day)")
44
Injections Clinical data supports the uses of intra-articular corticosteroids, even in repeated use (up to every 3 months for up to 2 years) particularly for patients with knee OA.
 particularly for patients with knee OA.")
45
Injections (My philosophy)
As an anti-inflammatory When pt has effusion When OA is known Not given to “return to sport” As an adjunct to PT Decrease acute symptoms to allow proper participation in physical therapy Not more than 3 per year.

46
Focal Chondral Defects
OCD Osteochondritis dissicens Osteochondral defect

47
FCD: Treatment Is it symptomatic?
Don’t make an asymptomatic finding a symptomatic problem Don’t be surprised! Treatment and rehab is very different

48
Chondral repair

49
Options Observation Chondroplasty Microfracture OATS (AOT)
ACI (Carticel) Osteochondral allograft Meniscus transplants Ligament reconstruction Correction of alignment Osteotomy
 Osteochondral allograft. Meniscus transplants. Ligament reconstruction. Correction of alignment. Osteotomy.")
50
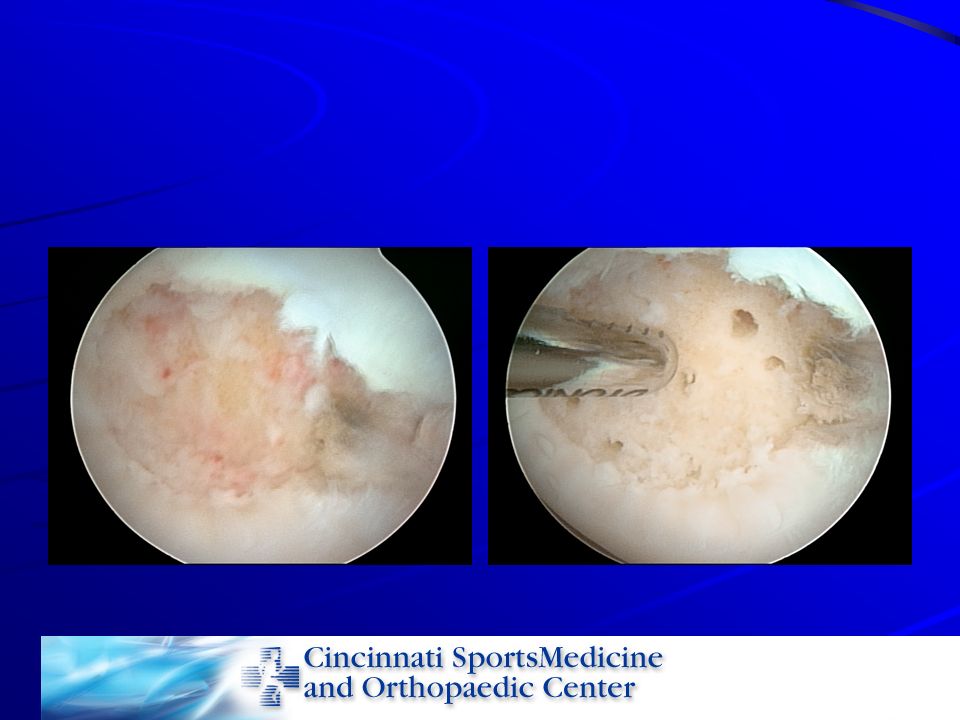
Microfracture Marrow stimulation technique
Body will produce repair tissue for a chondral defect if undifferentiated mesenchymal cells are accessed. Marrow cells, blood, platelets organize into the defect Differentiate into fibroblasts which produce a fibrocartilage “healing” of the defect

51
Microfracture Correct and incorrect methods Correct:
Debride defect, leaving a sharp shouldered edge.

53
Microfracture

54
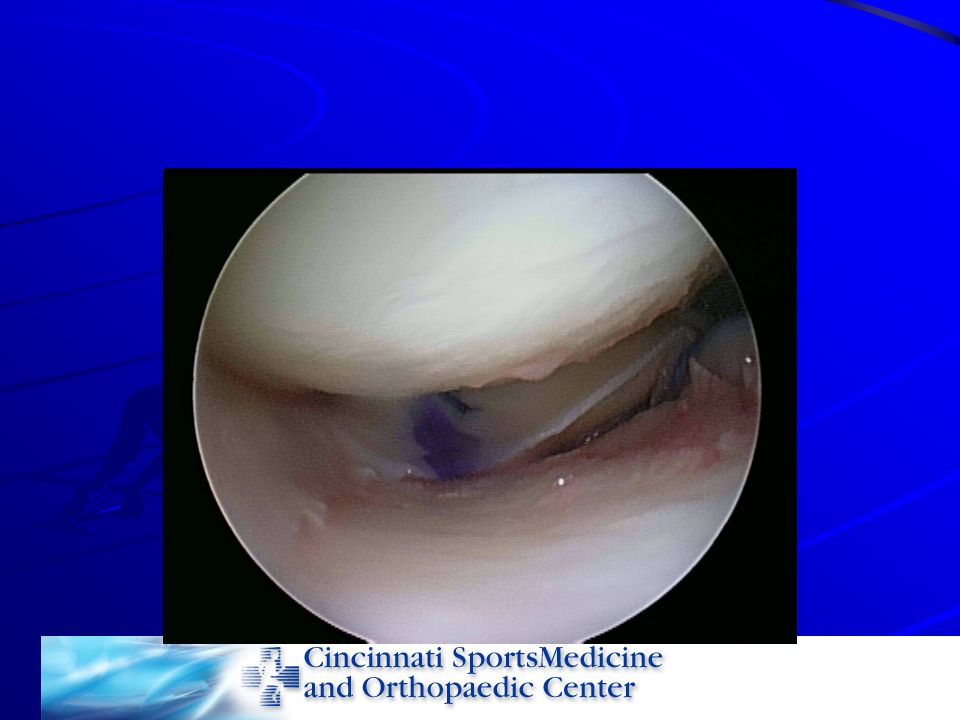
Microfracture is not “poking some holes in the cartilage”
“the same rehab as a menisectomy”

55
Rehab TTWB for 6-8 weeks (modified based on lesion location)
CPM at home for 6-8 weeks After 6-8 weeks begin active ROM and progress to full WB Cutting, twisting, pivoting 6 months

56
Success and cautions Return to impact sports Maybe not

57
Data HSS: 2006. Steadman: 2003 66% G-E results 44% returned to sports
57% of those at same level Steadman: 2003 76% of NFL players returned to play next season

58
Steadman: 2003 11.3 year f/u Pts 45 and younger with no meniscal or ligamentous pathology Showed improvement in function and had less pain.

59
Contraindications Malalignment Ligamentous instability
Unshouldered lesions Lesions > 10 mm deep Tibial lesions – less predictable results

60
ACI Autologous chondrocyte implantation 2 stage procedure
Scope, biopsy Culture cells Reimplant cells under patch (periosteum)
")
61
Pre-implant

62
Post implant

63
Rehab Protected WB CPM No running or impact loading until 12 months
High level sports at 16 months if pain free

64
Hypertrophy Reported with need for reoperation in up to 36% of patients… Reduced with non-periosteal covers collagen

65
After delamination

66
ACI as a second line Rx Unfortunately marrow stimulation techniques increase failure rate from ACI by up to 3X! Might not be best to mx then plan ACI if no better

67
OATS/ AOT

68
Osteochondral autograft transfer
Moves cartilage and its supporting bone Successful provided defect is not too large Limited by size Supply of cartilage

69
OCA Transplantation of allograft (cadaveric) cartilage and supporting bone. Successful in many series Concerns Disease Mismatch Non-healing

70
Osteochdral allograft

71
Technique

72
Final

73
Allograft meniscus transplantation
Role of intact meniscus is unquestioned Does an allograft function like a native meniscus? Disease Mismatch Non-healing Is it simply an “interposition arthroplasty”?

74
Meniscus Transplant

76
Return to sports? MFX, ACI, OATS, OCA:
Durable enough to allow long-term cutting, pivoting, impact sports? Studies are limited If these heal and incorporate, can attempt return to play if symptom free Would not typically advise return to distance running. For ACI, sports participation meant better long-term results.

77
Durability MAT and OCA have not been shown to have long-term superiority to prosthetic replacements. These are often “bridge” procedures that allow younger patients to avoid metallic arthroplasty and thus avoid revision.

78
The Future Resorbable matrix scaffolds
Off-label in US if used for focal defects Good results have been reported at short-term f/u

79
The Future MACI Cartilage “slurry” Equine cartilage
Matrix-induced ACI Culture chondrocytes implanted in collogen matrix prior to implantation No periosteal flap needed Cartilage “slurry” Equine cartilage Genetic alterations

80
The Future Don’t be the last or first to do something! Thanks

Similar presentations