Download presentation
Presentation is loading. Please wait.

1
Step into the void: Vestibular deficits in children with hearing loss
Genevieve DelRosario, MHS, PA-C University of Kansas Medical Center Kansas City, Kansas

3
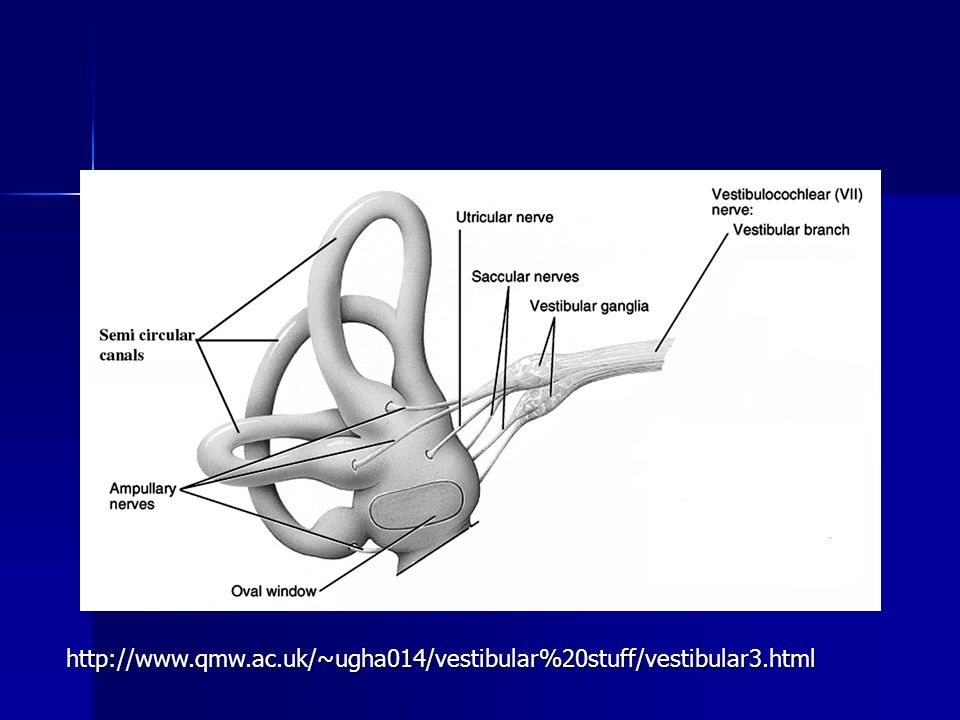
Objectives Review vestibular physiology and pathophysiology
Discuss the evaluation of a child’s vestibular status Be able to develop a plan for a child with vestibular dysfunction

4
Vestibular system: A “sixth sense”
Allows us to know where we are in space Orient selves with respect to gravity Unifying system that allows us to process information from other senses

5
Where does our sense of balance come from?
Eyes Sensors in joints, muscles, and feet Balance organs in the ears

6
Vestibular system Vestibular ocular system Vestibular spinal system
Responsible for visual stabilization Vestibular spinal system Maintains orientation of the body in space Contributes to the postural tone necessary for the acquisition of motor development milestones

7
Development of the vestibular system
Very old in evolutionary terms Emerges early in embryonic development Prior to vision and hearing Peak developmental time is 6-12 months Continues development through childhood

11
Prevalence of vestibular dysfunction*
20-70% of children with hearing loss Higher in profound HL vs. severe Continuum of severity Mild loss to vestibular areflexia * Angeli 2003.

12
What happens in deaf/HOH children?
Semicircular canals may be absent Hair cells may be damaged, absent, or reduced Nerve damage Enlarged vestibular aqueduct ???

13
Will a deaf child’s vestibular system get better?

14
……Maybe.

15
Better or worse? In general, balance improves as you age
Vestibular maturation continues through adolescence Vestibular deficits in deaf/HOH may worsen Small study showed progressive gross motor and balance difficulties1 Contradicted by other studies2 1. Rine et al Siegel et al 1991.

16
How does it feel?

17
How does it feel (adult perspective)?
Headache Feeling of ear fullness Imbalance to the point of being unable to walk Bouncing and blurring of vision (oscillopsia) Inability to tolerate head movement Difficulty walking in the dark Feel unsteady; actual unsteadiness while moving Lightheadedness Severe fatigue In severe cases, symptoms such as oscillopsia and problems with walking in the dark are not going to go away.
 Inability to tolerate head movement. Difficulty walking in the dark. Feel unsteady; actual unsteadiness while moving. Lightheadedness. Severe fatigue. In severe cases, symptoms such as oscillopsia and problems with walking in the dark are not going to go away.")
18
Oscillopia

19
Signs of poor vestibular function
Low muscle tone Delayed loss of primitive reflexes Delayed gross motor milestones Developmental delays Seizures Nystagmus Easy fatiguability Reflux

20
Signs of poor vestibular function
Low muscle tone Delay in holding head up “Snuggly” baby “Floppy baby” Arching of back

21
Signs of poor vestibular function
Delayed disappearance of newborn reflexes Moro ATNR: Asymmetric tonic next response Usually disappear by 6-7 months

22
Signs of poor vestibular function
Delayed motor milestones Average deaf child walks at 14 months Average child with Usher’s Type 1 walks at 20 mos Delays sitting, crawling, climbing steps, hopping… Speech delays

23
What do older children look like?
Clumsy Unable to walk on a balance beam Problems standing with feet together and eyes closed (Romberg test) Love spinning, merry-go-rounds, water activities
 Love spinning, merry-go-rounds, water activities.")
24
Weak VOR Challenges with reading
Gaze instability causes problems with acuity* Braswell & Rine 2006.

25
My deaf child is a late walker…does that mean she has vestibular problems?

26
No, but it’s a red flag! Consider also:
Vision problems Global developmental delay Autistic spectrum disorder Just taking her sweet time!

27
Tests of vestibular function
Eye tracking tests Positional/positioning tests Dix-Hallpike Supine Rotational tests Rotary chair testing is gold standard

28
Causes of poor vestibular function
Postnatal acquired cases Meningitis Labyrinthitis Some forms of syndromic deafness Labyrinthine dysplasia Ototoxicity

29
Conditions associated with CHL and poor balance
Usher’s Syndrome (Type 1) Waardenburg Syndrome Pendred syndrome ESPN mutation CHARGE Syndrome Brachio-oto-renal syndrome ….and more!
 Waardenburg Syndrome. Pendred syndrome. ESPN mutation. CHARGE Syndrome. Brachio-oto-renal syndrome. ….and more!")
30
Usher’s Syndrome Autosomal recessive syndrome
Hearing loss, vision loss, and variable vestibular dysfunction Visual loss is due to retinitis pigmentosa Three types

31
Usher’s syndrome Type 1 Type 2 Type 3 Born profoundly deaf
Vision loss typically noted by age 10 Absent vestibular function 3-6/100,000 individuals ~ 5% of deaf individuals Type 2 Moderate to severe hearing loss Vision loss typically begins after teen years Normal vestibular function Type 3 Born with normal hearing, varying rate of loss Night blindness during puberty Normal or near-normal vestibular function

32
Retinitis pigmentosa <> <>

33
Retinitis pigmentosa

34
Waardenburg Syndrome

35
Pendred Syndrome

36
CHARGE Syndrome Coloboma of the eye Heart defects
Atresia of the choanae Retardation of growth and/or development Genital and/or urinary abnormalities Ear abnormalities and deafness

37
Brachio-oto-renal syndrome
Autosomal dominant Malformation of ear cochlear hypoplasia enlargement of the cochlear and vestibular aqueducts hypoplasia of the lateral semicircular canal Hearing loss Malformations of kidney

38
ESPN Mutation Autosomal recessive mutation Mapped to chromosome 1p36.3

39
Environmental causes Aminoglycoside antibiotics Anti-neoplastics
Gentamicin, streptomycin, kanamycin, tobramycin, neomycin, amikacin, netilmicin, dihydrostreptomycin, and ribostamycin. Anti-neoplastics Cisplatin, carboplatin Environmental chemicals Butyl nitrite, mercury, carbon disulfide, styrene, carbon monoxide, tin, hexane, toluene, lead, trichloroethylene, manganese, xylene, mercury Loop diuretics Bumetanide, ethacrynic acid, furosemide, and torsemide. Aspirin and quinine products Infections

40
Vestibular effects of cochlear implantation
Rare cause of permanent damage Common cause of transient damage 20% in one series1 Anecdotal evidence for improvement Hearing with CI does not make a difference2 1: Vilbert et al Suarez et all 2007.

41
I think the child I am treating may have vestibular problems. Now what?

42
Evaluation CT of temporal bone Vestibular testing (if possible)
Physical, occupational, ? cognitive therapies Genetic appointment Strongly consider testing for Usher’s mutations Vision evaluation ?ERG

43
Therapeutic goals Enhance existing vestibular capabilities
Strengthen compensatory mechanisms

44
Compensatory mechanisms
Proprioceptive input Walking barefoot or soft soled shoes Visual input Other sensory systems

45
Therapies for children with poor vestibular systems
Swinging Rocking Bouncing/jumping Dancing Skipping Running Hopping Jumping rope Rough and tumble play

46
Other interventions May wear weighted vests, leg weights, etc
Consider orthopedic shoes OR soft soled shoes Offer sensory activities May need extra time to process information

47
Does treatment make a difference?
Motor development improved post treatment1 Therapy three times weekly for 12 weeks Visual and somatosensory function, balance training Significant improvement in motor development Insignificant improvement in posturography May improve gaze stability2 Preliminary study of two individuals 1. Rine et al Braswell and Rine 2006.

48
Treatment challenges Lack of data Different causes of balance problems
Especially true for infants and toddlers Different causes of balance problems

49
Cautions with poor vestibular function
Where visual and proprioceptive information is unreliable Eg, swimming in the dark Problems with depth perception Tunnel vision can cause problems Worse in unfamiliar places

50
Implications for future research
Vestibular hypofunction in infancy and early childhood poorly understood Need for research on both function and treatment

51
Implications for families
Share vestibular information with parents Encourage physical activity Continue to screen older children Balance Retinitis pigmentosa

52
Helpful resources What’s going on in there: How the brain and mind develop in the first five years of life. Lise Eliot, PhD. 1999 The out of sync child has fun. Carol Stock Kranowitz & TJ Wylie Vestibular disorders organization

54
Genevieve DelRosario gdelrosario@kumc
Genevieve DelRosario Department of Pediatrics University of Kansas Medical Center 3901 Rainbow Blvd Kansas City, KS (913)
")
55
Angeli S. Value of vestibular testing in young children with sensorineural hearing loss. Arch Otolaryngol Head Neck Surg. 2003;129: Braswell J, Rine RM. Evidence that vestibular hypofunction affects reading acuity in children. Int J Pediatr Otorhinolaryngol Nov; 70(11): Braswell, J, Rine RM. Preliminary evidence of improved gaze stability following exercise in two children with vestibular hypofunction. Int J Pediatr Otorhinolaryngol Nov;70(11): Epub 2006 Oct 4 Eliot, L. What’s going on in there: How the brain and mind develop in the first five years of life. Bantam Books, 1999. Rine RM, Braswell J, Fisher D, Joyce K, Kalar K, Shaffer M. Improvement of motor development and postural control following intervention in children with sensorineural hearing loss and vestibular impairment. Int J Pediatr Otorhinolaryngol Sep;68(9): Rine RM, Cornwall G, Gan K, LoCascio C, OHare T, Robinson E, Rice M. Evidence of progressive delay of motor development in children with sensorineural hearing loss and concurrent vestibular dysfunction. Perceptual and Motor Skills. 90(3 Pt 2): , 2000 June. Siegel JC, Marchetti M, Tecklin JS. Age-related balance changes in hearing-impaired children. Phys Ther Mar;71(3):183-9 Suarez H, Angeli S, Suarez A, Rosales B, Carrera X, Alonso R. Balance sensory ogranization in children with profound hearing loss and cochlear implants. Int J Pediatr Otorhinolaryngol Feb 1; [Epub ahead of print] Vibert D, Hausler R, Kompis M, Visher M. Vestibular function in patients with cochlear implantation. Acta Otolaryngol Suppl. 2001; 545:
: Braswell, J, Rine RM. Preliminary evidence of improved gaze stability following exercise in two children with vestibular hypofunction. Int J Pediatr Otorhinolaryngol Nov;70(11): Epub 2006 Oct Eliot, L. What’s going on in there: How the brain and mind develop in the first five years of life. Bantam Books, Rine RM, Braswell J, Fisher D, Joyce K, Kalar K, Shaffer M. Improvement of motor development and postural control following intervention in children with sensorineural hearing loss and vestibular impairment. Int J Pediatr Otorhinolaryngol Sep;68(9): Rine RM, Cornwall G, Gan K, LoCascio C, OHare T, Robinson E, Rice M. Evidence of progressive delay of motor development in children with sensorineural hearing loss and concurrent vestibular dysfunction. Perceptual and Motor Skills. 90(3 Pt 2): , 2000 June. Siegel JC, Marchetti M, Tecklin JS. Age-related balance changes in hearing-impaired children. Phys Ther Mar;71(3): Suarez H, Angeli S, Suarez A, Rosales B, Carrera X, Alonso R. Balance sensory ogranization in children with profound hearing loss and cochlear implants. Int J Pediatr Otorhinolaryngol Feb 1; [Epub ahead of print] Vibert D, Hausler R, Kompis M, Visher M. Vestibular function in patients with cochlear implantation. Acta Otolaryngol Suppl. 2001; 545:")
Similar presentations