Download presentation
Presentation is loading. Please wait.

1
Bayesian Clinical Trials
Scott M. Berry 1

2
Bayesian Statistics Reverend Thomas Bayes (1702-1761)
Essay towards solving a problem in the doctrine of chances (1764) This paper, on inverse probability, led to Bayes theorem, which led to Bayesian Statistics
 This paper, on inverse probability, led to Bayes theorem, which led to Bayesian Statistics.")
3
Bayes Theorem Bayesian inferences follow from Bayes theorem:
'(q| X) (q)*f (X | q) Assess prior ; subjective, include available evidence Construct model f for data Find posterior ' Both of these tasks are difficult.
 (q)*f (X | q) Assess prior ; subjective, include available evidence. Construct model f for data. Find posterior Both of these tasks are difficult.")
4
Simple Example Coin, P(HEADS) = p p = 0.25 or p =0.75, equally likely.
DATA: Flip coin twice, both heads. p ???

5
Bayes Theorem Posterior Probabilities Pr[ p = 0.75 | DATA] =
Pr[DATA | p=0.75] Pr[p=0.75] Pr[DATA | p=0.75] Pr[p=0.75] + Pr[DATA | p=0.25] Pr[p=0.25] (0.75)2 (0.5) = 0.90 (0.75)2 (0.5) + (0.25)2 (0.5) Posterior Probabilities Likelihood Prior Probabilities
![Bayes Theorem Posterior Probabilities Pr[ p = 0.75 | DATA] =](http://slideplayer.com/slide/709162/2/images/5/Bayes+Theorem+Posterior+Probabilities+Pr%5B+p+%3D+0.75+%7C+DATA%5D+%3D.jpg "Pr[DATA | p=0.75] Pr[p=0.75] Pr[DATA | p=0.75] Pr[p=0.75] + Pr[DATA | p=0.25] Pr[p=0.25] (0.75)2 (0.5) = (0.75)2 (0.5) + (0.25)2 (0.5) Posterior Probabilities. Likelihood. Prior Probabilities.")
6
Rare Disease Example Suppose 1 in 1000 people have a rare disease, X, for which there is a diagnostic test which is 99% effective. A random subject takes the test, which says “POSITIVE.” What is the probability they have X? (0.99) (0.001) = !!! (0.99) (0.001) + (0.01) (0.999)
 (0.001) = !!! (0.99) (0.001) + (0.01) (0.999)")
7
Bayesian Statistics A subjective probability axiomatic approach was developed with Bayes theorem as the “mathematical crank”--Savage, Lindley (1950’s) Very different than classical statistics: a collection of tools Before ?: A philosophical niche, calculation very hard. Early 1990’s: Computers and methods made calculation possible…and more!
 Very different than classical statistics: a collection of tools. Before : A philosophical niche, calculation very hard. Early 1990’s: Computers and methods made calculation possible…and more!")
8
Bayesian Approach Probabilities of unknowns: hypotheses, parameters, future data Hypothesis test: Probability of no treatment effect given data Interval estimation: Probability that parameter is in the interval Synthesis of evidence Tailored to decision making: Evaluate decisions (or designs), weigh outcomes by predictive probabilities
, weigh outcomes by predictive probabilities.")
9
Frequentist vs. Bayesian— Seven comparisons
1. Evidence used? 2. Probability, of what? 3. Condition on results? 4. Dependence on design? 5. Flexibility? 6. Predictive probability? 7. Decision making?

10
Consequence of Bayes rule: The Likelihood Principle
The likelihood function LX() = f( X | ) contains all the information in an experiment relevant for inferences about It is important to distinguish between “observed data” and data generally.
 = f( X | ) contains all the information in an experiment relevant for inferences about It is important to distinguish between observed data and data generally.")
11
Short version of LP: Take data at face value
But “data” can be deceptive Caveats . . . How identified? Why are they showing me this?

12
Example Data: 13 A's and 4 B's Parameter = = P(A wins)
Likelihood 13 (1–)4 Frequentist conclusion? Depends on design
4. Frequentist conclusion Depends on design.")
13
Frequentist hypothesis testing
P-value = Probability of observing data as or more extreme than results, assuming H0. P-V = P(tail of dist. | H0) Four designs: (1) Observe 17 results (2) Stop trial once both 4 A's and 4 B's (3) Interim analysis at 17, stop if or A's, else continue to n = 44 (4) Stop when "enough information"
 Four designs: (1) Observe 17 results. (2) Stop trial once both 4 A s and 4 B s. (3) Interim analysis at 17, stop if or A s, else continue to n = 44. (4) Stop when enough information")
14
Design (1): 17 results Binomial distribution with n = 17, = 0.5;
P-value = 0.049

15
Design (2): Stop when both 4 A’s and 4 B’s
Two-sided negative binomial with r = 4, = 0.5; P-value = 0.021

16
Design (3): Interim analysis at n=17, possible total is 44
Analyses at n = 17 & 44; 17 if 0-4 or 13-17; P = 0.085 Both shaded regions = 0.049 P(both) = 0.013; net = 2(0.049) – 0.013 = 0.085
 = 0.013; net = 2(0.049) – =")
17
Design (4): Scientist’s stopping rule: Stop when you know the answer
Cannot calculate P-value Strictly speaking, frequentist inferences are impossible

18
Bayesian Calculations
Data: 13 A's and 4 B's Parameter = = P(A wins) For ANY design with these results, the likelihood function is P(data | p) 13 (1–)4 Posterior probabilities & Bayesian conclusion same for any design
 For ANY design with these results, the likelihood function is. P(data | p) 13 (1–)4. Posterior probabilities & Bayesian conclusion same for any design.")
19
Likelihood function of

20
Posterior Distribution
Prior: < < 1 Posterior 1 * 13 (1–)4 = 1 * 13 (1–)4 / ∫ 1 * 13 (1–)4 d = {13!4!/18!} 13 (1–)4
4. = 1 * 13 (1–)4 / ∫ 1 * 13 (1–)4 d = {13!4!/18!} 13 (1–)4.")
21
Posterior density of for uniform prior: Beta(14,5)
")
22
Pr[ > 0.5 ]
![Pr[ > 0.5 ]](http://slideplayer.com/slide/709162/2/images/22/Pr%5B%EF%81%B0+%3E+0.5+%5D.jpg "Pr[ > 0.5 ]")
23
PREDICTIVE PROBABILITIES
Distribution of future data? P(next is an A) = ? Critical component of experimental design In monitoring trials
 = Critical component of experimental design. In monitoring trials.")
24
Laplace’s rule of succession
P(A wins next pair | data) = EP(A wins next pair | data, ) = E( | data) = mean of Beta(14, 5) = 14/19 Laplace uses Beta(1,1) prior
 = EP(A wins next pair | data, ) = E( | data) = mean of Beta(14, 5) = 14/19. Laplace uses Beta(1,1) prior.")
25
Updating w/next observation

26
Suppose 17 more observations
P(A wins x of 17 | data) = EP(A wins x | data, ) = Beta-Binomial Distribution
 = EP(A wins x | data, ) = Beta-Binomial Distribution.")
27
Predictive distribution
Predictive distribution of # of successes in next 17 tries: 88% probability of statistical significance Has more variability than any binomial

28
Best fitting binomial vs. predictive probabilities
Binomial, p=14/19 96% probability of statistical significance Predictive, p ~ beta(14,5) 88% probability of statistical significance
 88% probability. of statistical. significance.")
29
Possible Calculation Simulate a from the beta(14,5)
Simulate an x from binomial(17, ) Distribution of x’s is beta-binomial--the predictive distribution
 Distribution of x’s is beta-binomial--the predictive distribution.")
30
Posterior and Predictive…same?
Clinical Trial, 100 subjects. HA: > 0.25? FDA will approve if # success ≥ 33 [post > 0.95, beta(1,1)] See 99 subjects, 32 successes Pr[ > 0.25 | data ] = 0.955 Predictive prob trial success = 0.327
] See 99 subjects, 32 successes. Pr[ > 0.25 | data ] = Predictive prob trial success =")
31
Predictive Probabilities for Medical Device
Bayesian calculations FDA: Some patients have reached 2 years Some patients have only 1-yr follow-up

32
Continuous data; Patients w/both 12 and 24 months

33
Some patients with only 12-month data

34
Kernel density estimates

35
Small bandwidth (0.2)
")
36
Larger bandwidth (0.3)
")
37
Still larger bandwidth (0.4)
")
38
Very large bandwidth (0.5) (nearly bivariate normal)
 (nearly bivariate normal)")
39
Condition on 12-month value

40
Conditional distribution of 24-month value (0.2)
")
41
For largest bandwidth (0.5)
")
42
Multiple imputation: simulate full set of 24-month data

43
Simulate experimental patients and controls in this way— multiple imputation
Make inferences with full data (for example, equivalent improvement) Repeat simulations (≥10,000 times) Gives probability of future results– for example, of “equivalence”
 Repeat simulations (≥10,000 times) Gives probability of future results– for example, of equivalence")
44
Monitoring example: Baxter’s DCLHb
Diaspirin Cross-Linked Hemoglobin Blood substitute; emergency trauma Randomized controlled trial (1996+) Treatment: DCLHb Control: saline N = 850 (= 425x2) Endpoint: death
 Treatment: DCLHb. Control: saline. N = 850 (= 425x2) Endpoint: death.")
45
Waiver of informed consent
Data Monitoring Committee First DMC meeting: DCLHb Saline Dead 21 (43%) 8 (20%) Alive Total No formal interim analysis
 8 (20%) Alive Total No formal interim analysis.")
46
Bayesian predictive probability of future results (no stopping)
Probability of significant survival benefit for DCLHb after 850 patients: (PP=0.0097) DMC paused trial: Covariates? DMC stopped the trial
 DMC paused trial: Covariates DMC stopped the trial.")
47
Herceptin in Neoadjuvant BC
Endpoint: tumor response Balanced randomized, A & B Sample size planned: 164 Interim results after n = 34: Control: 4/16 = 25% (pCR) Herceptin: 12/18 = 67% (pCR) Not unexpected (prior?) Predictive prob of stat sig: 95% DMC stopped the trial ASCO and JCO—reactions …
 Herceptin: 12/18 = 67% (pCR) Not unexpected (prior ) Predictive prob of stat sig: 95% DMC stopped the trial. ASCO and JCO—reactions …")
48
Mixtures: Data: 13 A's and 4 B's Likelihood p13 (1–p)4
4")
49
Mixture Prior p ~ p0 I[p=p0] + (1-p0) Beta(a,b)
p p0 I0 p013(1-p0)4 + (1-p0) Kpa+13-1(1-p)b+4-1 p ~ p0 I0 + (1-p0) Beta(a+13,b+4 ) p0 p13(1-p)4 p0 = G(a)G(b)G(a+b+17) p0 p13(1-p)4 + (1-p0) G(a+13)G(b+4)G(a+b)
![Mixture Prior p ~ p0 I[p=p0] + (1-p0) Beta(a,b)](http://slideplayer.com/slide/709162/2/images/49/Mixture+Prior+p+%7E+p0+I%5Bp%3Dp0%5D+%2B+%281-p0%29+Beta%28a%2Cb%29.jpg "p p0 I0 p013(1-p0)4 + (1-p0) Kpa+13-1(1-p)b+4-1. p ~ p0 I0 + (1-p0) Beta(a+13,b+4 ) p0 p13(1-p)4. p0 = G(a)G(b)G(a+b+17) p0 p13(1-p)4 + (1-p0) G(a+13)G(b+4)G(a+b)")
50
Mixture Posterior p0=.5 Pr(p=0.5) = 0.246 P(p > 0.5) = 0.742
 = P(p > 0.5) = 0.742")
51
Crooked-Penny Example
Flip the coin 20 times. What is q for your coin? Everyone reports p for their coin. ^ A new estimate for q? Are others relevant for you?

52
Numbers of heads This is you

53
One-Sample Problem [q] ~ Beta(a,b) [X] ~ Binomial(n,q)
[q|X]~Beta(a+X,b+n-X) Mean = (a + X)/(a+b+n)
![One-Sample Problem [q] ~ Beta(a,b) [X] ~ Binomial(n,q)](http://slideplayer.com/slide/709162/2/images/53/One-Sample+Problem+%5Bq%5D+%7E+Beta%28a%2Cb%29+%5BX%5D+%7E+Binomial%28n%2Cq%29.jpg "[q|X]~Beta(a+X,b+n-X) Mean = (a + X)/(a+b+n)")
54
For uniform prior (a = b = 1)
Posterior: q ~ Beta(17, 5) Prior: q ~ Beta(1, 1) 0.77
 Prior: q ~ Beta(1, 1)")
55
For a = b = 10 Posterior: q ~ Beta(26, 14) Prior: q ~ Prior: q ~
0.65

56
Remember the other coins . . .
This is you

57
Learning about the prior
In your setting the other coins give you information about the prior…which helps!!!! The coins do not have to be the same or close, you learn the appropriate amount of borrowing.

58
HIERARCHICAL MODELING
Population: Sample: Inferential problems Sample from sample:

59
Selecting coins Population of coins—population of q’s:
Select two coins and toss each coin 10 times: one 9 heads, other 4 heads. Estimate q1, q2. Estimate distribution of q’s in population.

60
Generic example: Unit is lab or drug variation or lot or study
Unit s n s/n Total n = #observations s = #successes s/n = success proportion

61
If q1 = q2 = . . . = q9 = q (all 150 units exchangeable)
")
62
Assuming equal q’s, 95% CI for q: (0.63, 0.77)
But 7 of 9 estimates lie outside this interval. Combined analysis unsatisfactory. Nine different analyses even worse: nine individual CIs?

63
Suppose ni independent observations on unit i
Suppose each unit has its own q, with q1, , q9 having distribution G. Observe x's, not q's. Xi ~ binomial(ni, qi). Likelihood is product of likelihoods of qi
. Likelihood is product of likelihoods of qi.")
64
Bayesian view: G unknown = G has probability distribution
Prior distribution reflects heterogeneity vs homogeneity. Assume G is Beta(a,b), a > 0, b > 0 with a and b unknown. Study heterogeneity: little if a+b is large lots if a+b is small
, a > 0, b > 0 with a and b unknown. Study heterogeneity: little if a+b is large. lots if a+b is small.")
65
Beta(a,b) for a, b = 1, 2, 3, 4:
 for a, b = 1, 2, 3, 4:")
66
Suppose uniform prior for a & b on integers 1, . . ., 10

67
Posterior probabilities for a & b

68
Calculating posterior distribution of G
Direct in this example Can be more complicated, and require: Gibbs sampling (BUGS) Other Markov chain Monte Carlo
 Other Markov chain Monte Carlo.")
69
Posterior mean of G (also predictive density for q)
")
70
Contrast with likelihood assuming all p’s equal

71
Bayesian questions: P(q > 1/2) = ????
P(next unit in study i is success) = ? How to weigh results in unit i? How to weigh results in unit j? P(unit in 10th study is success) = ? How to weigh results in study i?
 = How to weigh results in unit i How to weigh results in unit j P(unit in 10th study is success) = How to weigh results in study i")
72
Bayes estimates Unit x n x/n Bayes 1 20 20 1.00 0.90 2 4 10 0.40 0.53
Total (0.71)
")
73
Bayes estimates are regressed or shrunk toward overall mean
Unadjusted estimates

74
Baseball Example 446 players in 2000 with > 100 at bats Jose Vidro

75
X ~ Binomial(606, qJV) (hits) qJV ~ Beta(a,b) How good was Jose Vidro?
(200 hits in 606 at bats, 0.330) X ~ Binomial(606, qJV) (hits) qJV ~ Beta(a,b)
 X ~ Binomial(606, qJV) (hits) qJV ~ Beta(a,b)")
76
Empirical Bayes: aEB = bEB=258.9 (mean = 0.269; var = ) [q|X] ~ Beta( , ) (approx) Posterior mean = 0.308 Posterior st. dev. = 0.015
![Empirical Bayes: aEB = 95.5 bEB= (mean = 0.269; var = ) [q|X] ~ Beta( , ) (approx)](http://slideplayer.com/slide/709162/2/images/76/Empirical+Bayes%3A+aEB+%3D+95.5+bEB%3D+%28mean+%3D+0.269%3B+var+%3D+%29+%5Bq%7CX%5D+%7E+Beta%28+%2C+%29+%28approx%29.jpg "Posterior mean = Posterior st. dev. =")
77
Science, Feb 6, 2004, pp 784-6

78
Efficacy of Pravastatin + Aspirin: Meta-Analyses
ohrms/dockets/ac/02/slides/ 3829s2_03_Bristol-Meyers-meta-analysis.ppt Efficacy of Pravastatin + Aspirin: Meta-Analyses [For statistical analysis, S.M. Berry et al., Journal of the American Statistical Association, 2004]

79
Meta-Analysis of these Pravastatin Secondary Prevention Trials
Number of Subjects* % on Aspirin Primary Endpoint LIPID 9014 82.7 CHD mortality CARE 4159 83.7 CHD death & non-fatal MI REGRESS 885 54.4 Atherosclerotic progression (& events) PLAC I 408 67.5 Atherosclerotic progression (& events) PLAC II 151 42.7 Atherosclerotic progression (& events) Totals 14,617 80.4 *99.7% of pravastatin-treated subjects received 40mg dose
 PLAC I Atherosclerotic progression (& events) PLAC II Atherosclerotic progression (& events) Totals. 14, *99.7% of pravastatin-treated subjects received 40mg dose.")
80
Trial Commonalities Similar entry criteria
Patient populations with clinically evident CHD Same dose of pravastatin (40mg) Randomized comparison against placebo All trials with durations of 2 years Pre-specified endpoints Covariates recorded Common meta-analysis data management
 Randomized comparison against placebo. All trials with durations of 2 years. Pre-specified endpoints. Covariates recorded. Common meta-analysis data management.")
81
Patient Group Comparisons
Randomized Groups Pravastatin Placebo Aspirin Users Prava+ASA Prava alone Placebo+ASA Placebo alone Randomized Comparison Aspirin Non-Users Observational Comparison

82
Is Pravastatin+Aspirin More Effective than Pravastatin Alone?
Aspirin studies were conducted before statins were widely used Placebo-controlled trial with aspirin is not feasible Investigation of pravastatin database to explore this question

83
Is the Combination More Effective than Pravastatin Alone?
Unadjusted event rates in LIPID and CARE suggest pravastatin + aspirin is more effective than pravastatin alone

84
Event Rates for Primary Endpoints in LIPID and CARE
Pravastatin-treated Subjects Only Trial: Primary Endpoint: LIPID CHD Death CARE CHD Death or Non-fatal MI Aspirin Users 5.8% 8.8% Observational Comparison 14.8% 9.3% Aspirin Non-Users

85
Accounting for Baseline Risk Factors
Age Gender Previous MI Smoking status Baseline LDL-C, HDL-C, TG Baseline DBP & SBP Additional analyses also included revascularization, diabetes and obesity

86
Meta-Analysis Endpoints Considered
Fatal or non-fatal MI Ischemic stroke Composite: CHD death, non-fatal MI, CABG, PTCA or ischemic stroke

87
H(t) = l0(t)exp(Zb + fS + gT)
Meta-Analysis Models Model 1: Multivariate Cox proportional hazards model Patients combined across trials; trial effect is a fixed covariate H(t) = l0(t)exp(Zb + fS + gT) Covariates Baseline Hazards constant Study effects Treatment Effects
 = l0(t)exp(Zb + fS + gT) Covariates. Baseline Hazards. constant. Study. effects. Treatment Effects.")
88
Relative Risk Reduction Cox Proportional Hazards – All Trials
Prava+ASA vs ASA alone Prava+ASA vs Prava alone Fatal or Non-Fatal MI 0.400 0.800 1.000 0.600 Relative Risk (95% CI) RRR 31% 0.69 26% 0.74 Prava+ASA vs ASA alone Prava+ASA vs Prava alone 29% 0.71 31% 0.69 Ischemic Stroke 0.400 0.800 1.000 0.600 0.400 0.800 1.000 0.600 CHD Death, Non-Fatal MI, CABG, PTCA, or Ischemic Stroke Prava+ASA vs ASA alone Prava+ASA vs Prava alone 24% 0.76 13% 0.87 RRR = Relative Risk Reduction
 RRR. 31% % Prava+ASA vs ASA alone. Prava+ASA vs Prava alone. 29% % Ischemic Stroke CHD Death, Non-Fatal MI, CABG, PTCA, or Ischemic Stroke. Prava+ASA vs ASA alone. Prava+ASA vs Prava alone. 24% % RRR = Relative Risk Reduction.")
89
H(t) = l0(t)exp(Zb + fS + gT)
Meta-Analysis Models Model 2: Same as Model 1 except Allows trial heterogeneity: Bayesian hierarchical (random effects) model of trial effect H(t) = l0(t)exp(Zb + fS + gT) Covariates Baseline Hazards piecewise-constant Study effects Hierarchical Treatment Effects
 model of trial effect. H(t) = l0(t)exp(Zb + fS + gT) Covariates. Baseline Hazards. piecewise-constant. Study. effects. Hierarchical. Treatment Effects.")
90
Model 2 – Hierarchical, Random Effects
Fatal or Non-Fatal MI 0.000 0.025 0.050 0.075 0.100 1 2 3 4 5 Placebo Prava alone ASA alone Prava+ASA Cumulative Proportion of Events Year

91
Model 2 – Hierarchical, Random Effects
Ischemic Stroke Only 0.000 0.005 0.010 0.015 0.020 0.025 1 2 3 4 5 Prava alone Placebo ASA alone Prava+ASA Cumulative Proportion of Events Year

92
Model 2 – Hierarchical, Random Effects
CHD Death, Non-Fatal MI, CABG, PTCA, or Ischemic Stroke 0.00 0.05 0.10 0.15 0.20 0.25 1 2 3 4 5 Year Prava alone Placebo Prava+ASA ASA alone Cumulative Proportion of Events

93
Combination is More Effective than Either Agent Alone
Pravastatin + aspirin provides benefit for all three endpoints: 24% - 34% RRR compared with aspirin 13% - 31% RRR compared with pravastatin This benefit was similar in Models 1 and 2 This benefit was consistent in both LIPID and CARE trials

94
Model 2: Fatal or Non-Fatal MI
Cumulative Proportion of Events 0.000 0.025 0.050 0.075 0.100 Year 1 2 3 4 5 Prava+ASA ASA alone Prava alone Placebo 0.000 0.005 0.010 0.015 0.025 Year 1 2 3 4 5 0.020 Hazard Prava+ASA ASA alone Prava alone Placebo

95
H(t) = lT0(t)exp(Zb + fS)
Meta-Analysis Models Model 3: Same as Model 2 except Treatment hazard ratios vary over time H(t) = lT0(t)exp(Zb + fS) Baseline Hazards piecewise-constant Within treatment Covariates Study Effects Hierarchical
 = lT0(t)exp(Zb + fS) Baseline Hazards. piecewise-constant. Within treatment. Covariates. Study. Effects. Hierarchical.")
96
Model 3: Fatal or Non-Fatal MI
Cumulative Proportion of Events 0.000 0.025 0.050 0.075 0.100 Year 1 2 3 4 5 Prava+ASA ASA alone Prava alone Placebo 0.000 0.005 0.010 0.015 0.030 Year 5 Separate Analyses: One per Year 1 2 3 4 5 0.020 Hazard 0.025 Prava+ASA ASA alone Prava alone Placebo

97
Probability of synergy between pravastatin & aspirin
Endpoint Model 2 Model 3 All events 0.983 0.985 Cardiac events 0.945 0.947 Any MI 0.911 0.923 Stroke 0.924 0.906 Death 0.997

98
Conclusion of Hazard Analysis over Time
Benefit of pravastatin+aspirin over aspirin was present in each year of the 5-year duration of the trials Benefit of pravastatin+aspirin over pravastatin was present in each year of the 5-year duration of the trials Benefits estimated from Model 1 (and confidence intervals) confirmed by more general models and fewer assumptions
 confirmed by more general models and fewer assumptions.")
99
Hierarchical modeling in design
Using historical information Combining results from multiple concurrent trials (or many centers)
")
100
Hierarchical modeling & dose-response
Example: drug Z (rozuvastatin) vs drug A (atorvastatin) (Berry et al., 2002, American Heart Journal)
 vs drug A (atorvastatin) (Berry et al., 2002, American Heart Journal)")
101
Studies involving drugs A and Z*, with %change from baseline.
Study n Dose Mean SD Y – 45 20 – – Placebo – – 16 20 – 12 80 – – – – – Placebo – Placebo 18 10 – – – 51 20 – 61 40 – 10 80 –

102
Study n Dose Mean SD Y – –37.6 NA 0.624 Placebo – – 11 10 – 10 20 – 11 40 – 11 80 – – –46 NA 0.54 Placebo 15 10 – 13 80 – 14 1* – * – 16 5* – 17 10* – 17 20* – 18 40* – Placebo 15 40* – 31 80* –

103
Dose-response model Yij = exp{as + at + bt log(d)} + eij s for study
t for drug d for dose i for observation (1, , 43) j for patient within study/dose eij is N(0, s2) Priors don’t matter much, except . . .
 j for patient within study/dose. eij is N(0, s2) Priors don’t matter much, except")
104
Prior for as ~ N(0, t2) t2 is important
t2 large means studies heterogeneous—little borrowing t2 small means studies homogeneous—much borrowing Prior of t2 is IG(10, 10) Prior mean and sd are 0.10 & 0.017
 Prior mean and sd are 0.10 &")
105
Likelihood Calculations of posterior & predictive distributions by MCMC

106
Posterior means and SDs
Parameter Mean StDev aP – aA – aZ – bA – bZ – s t

107
Posterior means and SDs
Par. Mean StDev Par. Mean StDev a a10 – a2 – a a a12 – a4 – a13 – a5 – a a6 – a a a16 – a a17 – a9 –

108
Model fit

109
Interval estimates for pop. mean: model (line) vs standard (box)
 vs standard (box)")
110
Study/dose-specific interval estimates: model (line) vs standard (box)
 vs standard (box)")
111
Posterior dist’n of reduction (95% intervals)
Drug A Drug Z

112
Posterior dist’n of mean diff, A – Z

113
Really neat . . . Using predictive probabilities for designing future studies Contour plots

114
Observed %Y for future study with nA=nZ=20 dA=dZ=10

115
Observed %Y for future study with nA=nZ=100 dA=dZ=10

116
Observed %Y for future study with nA=nZ=20 dA=10, dZ=5

117
Observed %Y for future study with nA=nZ=100 dA=10, dZ=5

118
STELLAR trial results (each n≈160)
Predicted atorva -36% Predicted rosuva -41% -46% -50% -52% -54% -58%

119
Posterior dist’n of reduction (95% intervals)
Recall: Drug A Drug Z

120
Adaptive Phase II: Finding the “Best” Dose
Scott M. Berry

121
Standard Parallel Group Design
Equal sample sizes at each of k doses. Doses 7

122
True dose-response curve (unknown)
Doses 7

123
Observe responses (with error) at chosen doses
7

124
Dose at which 95% max effect
Response True ED95 Doses 8

125
Uncertainty about ED95 Response ? Doses 7

126
Increase number of doses
Solution: Increase number of doses Response True ED95 Doses 8

127
But, enormous sample size, and . . . wasted dose assignments—always!
Response True ED95 Doses 8

128
Solutions Lots of doses (continuum?) Adaptive Allocation
Model dose response Define what you are looking for Stop when you find what you are looking for… Yogi Berra-ism: If you don’t know where you are going, how do you know when you get there?

129
Dose Finding Trial Real example (all details hidden, but flavor is the same) “Delayed” Dichotomous Response (random waiting time) Combine multiple efficacy + safety in the dose finding decision Use utility approach for combining various goals Multiple statistical goals Adaptive stopping rules

130
Adaptive Approach

131
Statistical Model The statistical model captures all the uncertainty in the process. Capture data, quantities of interest, and forecast future data Be “flexible,” (non-monotone?) but capture prior information on model behavior. Invisible in the process
 but capture prior information on model behavior. Invisible in the process.")
132
Empirical Data Observe Yij for subject i, outcome j
Yij = 1 if event, 0 otherwise j = 1 is type #1 efficacy response j = 2 is type #2 efficacy response j = 3 is minor safety event j = 4 is major safety event

133
Efficacy Endpoints j(d) ~ N(j, 2) Let d be the dose
Pj(d) probability of event j, dose d. j(d) ~ N(j, 2) G(1,1) N(1,1) N(–2,1) IG(2,2)
 probability of event j, dose d. j(d) ~ N(j, 2) G(1,1) N(1,1) N(–2,1) IG(2,2)")
134
Safety Endpoint Let di be the dose for subject i
Pj(d) probability of safety j, dose d. N(-2,1) G(1,1) N(1,1)
 probability of safety j, dose d. N(-2,1) G(1,1) N(1,1)")
135
Utility Function Multiple Factors: Utility is critical: Defines ED?
Monetary Profile (value on market) FDA Success Safety Factors Utility is critical: Defines ED?
 FDA Success. Safety Factors. Utility is critical: Defines ED")
136
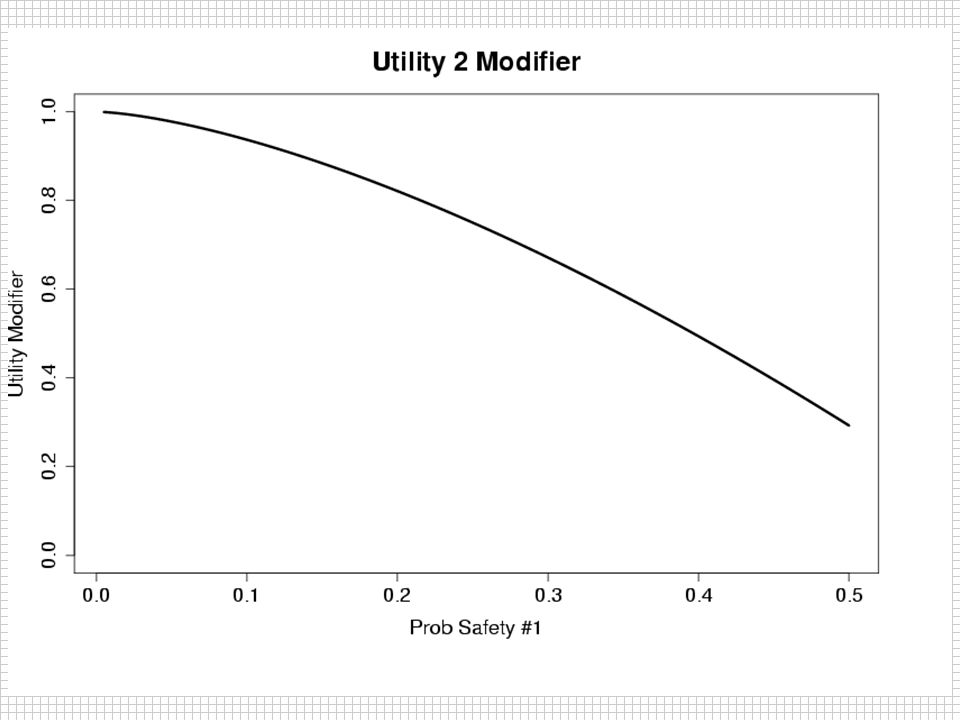
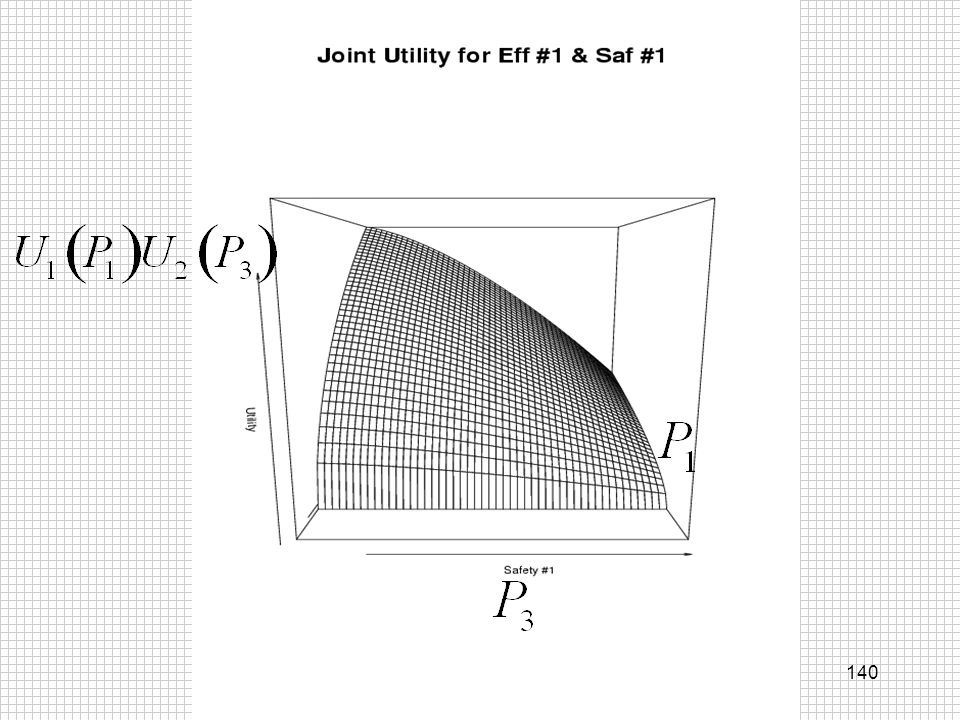
U(d)=U1(P1)U2(P3)*U3(P0,P2)*U4(P4)
Utility Function U(d)=U1(P1)U2(P3)*U3(P0,P2)*U4(P4) Monetary FDA Approval Extra Safety P0 is prob efficacy 2 success for d=0
=U1(P1)U2(P3)*U3(P0,P2)*U4(P4) Monetary. FDA Approval. Extra Safety. P0 is prob efficacy 2 success for d=0.")
137
Monetary Utility

141
U3: FDA Success “DSMB?”

142
Statistical + Utility Output
E[U(d)] E[j(d)], V[j(d)] E[Pj(d)], V[Pj(d)] Pr[dj max U] Pr[P2(d) > P0] Pr[ P2 >> P0 | 250/per arm) each d >> means statistical significance will be achieved
] E[j(d)], V[j(d)] E[Pj(d)], V[Pj(d)] Pr[dj max U] Pr[P2(d) > P0] Pr[ P2 >> P0 | 250/per arm) each d. >> means statistical significance will be achieved.")
143
Allocator Goals of Phase II study? Find best dose?
Learn about best dose? Learn about whole curve? Learn the minimum effective dose? Allocator and decisions need to reflect this (if not through the utility function) Calculation can be an important issue!
 Calculation can be an important issue!")
144
Allocator d* is the max utility dose, d** second best Find best dose?
Learn about best dose? d* is the max utility dose, d** second best Find the V* for each dose ==> allocation probs

145
Allocator V*(d≠0) = V*(d=0) =
 = V*(d=0) =")
146
Allocator “Drop” any rd<0.05 Renormalize

147
Decisions Shut down allocator wj if stop!!!!
Find best dose? Learn about best dose? Shut down allocator wj if stop!!!! Stop trial when both wj = 0 If Pr(P2(d*) >> P0) < 0.10 stop for futility If found, stop: Pr(d = d*) > C1 If found, stop: Pr(P2(d*) >> P0)>C2
 >> P0) < 0.10 stop for futility. If found, stop: Pr(d = d*) > C1. If found, stop: Pr(P2(d*) >> P0)>C2.")
148
More Decisions? Ultimate: EU(dosing) > EU(stopping)?
Wait until significance? Goal of this study? Roll in to phase III: set up to do this Utility and why? are critical and should be done--easy to ignore and say it is too hard.

149
Simulations Subject level simulation
Simulate 2/day first 70 days, then 4/day Delayed observation exponential with mean 10 days Allocate + Decision every week First 140 subjects 20/arm

150
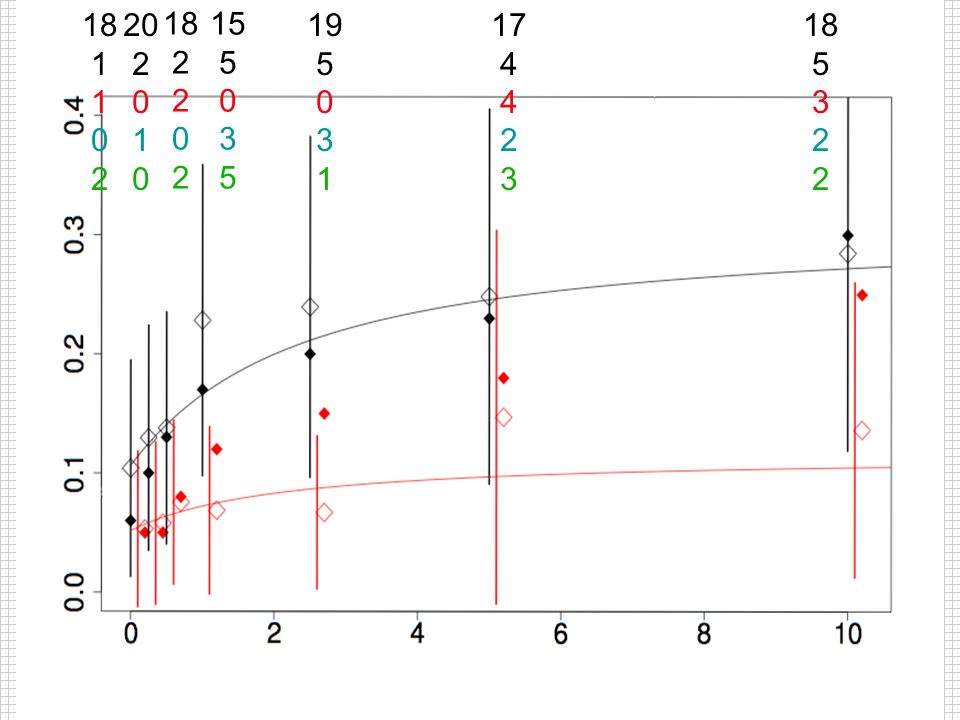
Scenario #1 Stopping Rules: C1 = 0.80, C2 = 0.90 Dose P1 P2 P3 P4 UTIL
0.06 0.05 0.25 0.10 0.5 0.13 0.08 0.07 0.063 1 0.17 0.12 0.323 2.5 0.20 0.15 0.09 0.457 5 0.23 0.18 0.532 10 0.30 0.11 0.656 MAX Stopping Rules: C1 = 0.80, C2 = 0.90

151
18 1 2 20 2 1 18 2 15 5 3 19 5 3 1 17 4 2 3 18 5 3 2
152
Dose Probabilities .25 .5 1 2.5 5 10 .18 .33 .27 .29 .67 P(max) .01
.25 .5 1 2.5 5 10 P(>>Pbo) .18 .33 .27 .29 .67 P(max) .01 .04 .06 .52 P(2nd) .03 .10 .13 .35 .32 Alloc .02 .46
 P(max) P(2nd) Alloc")
153
20 1 3 20 2 1 18 2 19 5 1 4 19 5 3 25 7 8 2 24 7 5 2

154
Dose Probabilities .25 .5 1 2.5 5 10 .12 .38 .36 .92 .91 P(max) .00
.25 .5 1 2.5 5 10 P(>>Pbo) .12 .38 .36 .92 .91 P(max) .00 .02 .04 .41 .53 P(2nd) .03 .06 .07 .47 .37 Alloc .09 .34 .51
 P(max) P(2nd) Alloc")
155
21 2 1 20 2 1 19 3 2 1 20 5 1 4 21 5 3 4 29 7 9 2 11 31 11 6 3 17

156
Dose Probabilities .25 .5 1 2.5 5 10 .13 .39 .38 .26 .97 .85 P(max)
.25 .5 1 2.5 5 10 P(>>Pbo) .13 .39 .38 .26 .97 .85 P(max) .00 .02 .03 .01 .55 P(2nd) .10 .05 .46 .35 Alloc .11
 P(max) P(2nd) Alloc")
157
23 2 1 4 20 2 1 20 4 2 21 5 1 4 25 5 1 4 36 7 10 3 45 12 10 3 16

158
Dose Probabilities .25 .5 1 2.5 5 10 .16 .41 .38 .48 .93 P(max) .00
.25 .5 1 2.5 5 10 P(>>Pbo) .16 .41 .38 .48 .93 P(max) .00 .02 .03 .04 .26 .65 P(2nd) .05 .07 .10 .49 .29 Alloc .08 .11 .18 .35 .28
 P(max) P(2nd) Alloc")
159
26 2 1 20 2 1 20 4 2 25 5 1 4 6 26 6 2 4 5 44 7 13 3 12 52 13 10 4 15

160
Dose Probabilities .25 .5 1 2.5 5 10 .16 .40 .31 .41 .98 .89 P(max)
.25 .5 1 2.5 5 10 P(>>Pbo) .16 .40 .31 .41 .98 .89 P(max) .00 .02 .03 .06 .27 .63 P(2nd) .12 .48 .28 Alloc .10 .04 .13 .26 .30
 P(max) P(2nd) Alloc")
161
26 2 1 6 20 2 1 21 4 2 3 26 6 1 4 5 33 7 3 4 5 52 8 13 4 10 61 18 15 4 12

162
Dose Probabilities .25 .5 1 2.5 5 10 .13 .36 .32 .65 .96 P(max) .00
.25 .5 1 2.5 5 10 P(>>Pbo) .13 .36 .32 .65 .96 P(max) .00 .01 .09 .08 .81 P(2nd) .05 .23 .52 .15 Alloc
 P(max) P(2nd) Alloc.")
163
Trial Ends P(10-Dose max Util dose) = 0.907
P(10-Dose >> Pbo 250/arm) = 0.949 280 subjects: 32, 20, 24, 31, 38, 62, 73 per arm
 = subjects: 32, 20, 24, 31, 38, 62, 73 per arm.")
164
Operating Characteristics
Pbo 0.25 0.5 1 2.5 5 10 SS 39 21 25 37 63 89 110 Pmax --- 0.00 0.04 0.96 66 0.01 0.06 0.93

165
Operating Characteristics
Adaptive Constant P(Success) 0.936 0.810 P(Cap) 0.064 0.190 P(Futility) 0.000 Mean SS 384 459 SD SS 186 224 Mean TDose 1754 1263 Max TDose 4818 2370
 P(Cap) P(Futility) Mean SS SD SS Mean TDose Max TDose")
166
Scenario #2 Stopping Rules: C1 = 0.80, C2 = 0.90 Dose P1 P2 P3 P4 UTIL
0.06 0.05 0.25 0.10 0.5 0.13 0.08 0.07 0.063 1 0.17 0.12 0.323 2.5 0.20 0.15 0.452 5 0.23 0.18 0.502 10 0.40 0.302 Stopping Rules: C1 = 0.80, C2 = 0.90

167
Operating Characteristics
Pbo 0.25 0.5 1 2.5 5 10 SS 71 27 41 81 137 172 164 Pmax --- 0.00 0.03 0.22 0.60 0.16 100 0.20 0.44 0.33

168
Operating Characteristics
Adaptive Constant P(Success) 0.314 0.266 P(Cap) 0.686 0.734 P(Futility) 0.000 Mean SS 694 702 SD SS 193 190 Mean TDose 2954 1937 Max TDose 4489
 P(Cap) P(Futility) Mean SS SD SS Mean TDose Max TDose")
169
Simulation #3 Stopping Rules: C1 = 0.80, C2 = 0.90 Dose P1 P2 P3 P4
UTIL 0.06 0.05 0.1 0.10 0.5 0.13 0.08 0.07 0.063 1 0.30 0.25 0.11 0.656 2.5 0.17 0.12 0.323 5 0.20 0.15 0.09 0.457 10 0.23 0.18 0.532 Stopping Rules: C1 = 0.80, C2 = 0.90

170
Operating Characteristics
Pbo 0.25 0.5 1 2.5 5 10 SS 53 23 28 119 52 76 102 Pmax --- 0.00 0.92 0.01 0.07 87 0.83 0.02 0.15

171
Operating Characteristics
Adaptive Constant P(Success) 0.906 0.596 P(Cap) 0.092 0.404 P(Futility) 0.002 0.000 Mean SS 453 606 SD SS 187 205 Mean TDose 1663 1662 Max TDose 3771
 P(Cap) P(Futility) Mean SS SD SS Mean TDose Max TDose")
172
Scenario #4 Stopping Rules: C1 = 0.80, C2 = 0.90 Dose P1 P2 P3 P4 UTIL
0.06 0.05 0.25 0.5 1 2.5 0.20 0.10 0.573 5 10 Stopping Rules: C1 = 0.80, C2 = 0.90

173
Operating Characteristics
Pbo 0.25 0.5 1 2.5 5 10 SS 53 21 22 23 150 160 163 Pmax --- 0.00 0.27 0.32 0.40 92 0.28 0.33

174
Operating Characteristics
Adaptive Constant P(Success) 0.514 0.408 P(Cap) 0.486 0.592 P(Futility) 0.000 Mean SS 591 647 SD SS 239 220 Mean TDose 2840 1780 Max TDose 4815
 P(Cap) P(Futility) Mean SS SD SS Mean TDose Max TDose")
175
Scenario #5 Stopping Rules: C1 = 0.80, C2 = 0.90 Dose P1 P2 P3 P4 UTIL
0.06 0.05 0.1 0.07 0.5 0.08 1 0.09 2.5 5 0.10 10 0.11 Stopping Rules: C1 = 0.80, C2 = 0.90

176
Operating Characteristics
Pbo 0.25 0.5 1 2.5 5 10 SS 92 91 75 66 76 83 90 Pmax --- 0.45 0.04 0.07 0.10 0.13 0.21 84 0.44 0.08 0.12 0.15 0.17

177
Operating Characteristics
Adaptive Constant P(Success) 0.004 0.006 P(Cap) 0.484 0.544 P(Futility) 0.512 0.450 Mean SS 574 589 SD SS 250 258 Mean TDose 1637 1615 Max TDose 3223.5
 P(Cap) P(Futility) Mean SS SD SS Mean TDose Max TDose")
178
Scenario #6 Stopping Rules: C1 = 0.80, C2 = 0.90 Dose P1 P2 P3 P4 UTIL
0.06 0.05 0.1 0.5 1 2.5 5 Stopping Rules: C1 = 0.80, C2 = 0.90

179
Operating Characteristics
Pbo 0.25 0.5 1 2.5 5 10 SS 66 77 51 34 38 41 43 Pmax --- 0.90 0.01 0.02 0.03 56 0.86 0.05

180
Operating Characteristics
Adaptive Constant P(Success) 0.000 P(Cap) 0.122 0.190 P(Futility) 0.878 0.810 Mean SS 350 395 SD SS 215 241 Mean TDose 811 1086 Max TDose 2404
 P(Cap) P(Futility) Mean SS SD SS Mean TDose Max TDose")
181
Bells & Whistles Interest in Quantiles Minimum Effective Dose
“Significance,” control type I error Seamless phase II --> III Partial Interim Information “Biomarkers” of endpoint Continuous (& Poisson) Continuum of doses (IV)--little additional n!!!
 Continuum of doses (IV)--little additional n!!!")
182
Conclusions Approach, not answers or details!
Shorter, smaller, stronger! Better for company, FDA, Science, PATIENTS Why study?--adaptive can help multiple needs. Adaptive Stopping Bid Step!

Similar presentations