Download presentation
Presentation is loading. Please wait.

1
Designing Safe and Effective Patient Handovers
Vineet Arora, MD, MA University of Chicago Julie Johnson, MSPH, PhD University of Chicago Quality Colloquium at Harvard August 21, 2008 10:45 – 12:45 pm

2
Objectives Determine which methods are most appropriate for exploring hand-offs in clinical settings Develop a standard process to optimize hand-offs using a process mapping methodology Create a checklist of critical patient and process information Design a strategy for dissemination and training Identify and overcome barriers to implementation Develop a plan to evaluate and monitor hand-off protocols

3
Agenda 10:45 – 10:50 Introduction and Overview of the Agenda
10:50 – 11:00 Participant Introductions and Expectations 11:00 – 11:10 Hand-off Theater 11:10 – 11:15 Audience Poll 11:15 – 11:30 What is known about Hand-offs in Medicine and other Industries 11:30 – 11:50 Small Group Exercise: Paper Tear 11:50 – 12:00 A Model for Developing a Standard Protocol 12:00 – 12:20 Small Group Exercise: Process Mapping 12:20 – 12:30 Completing the Hand-off Model 12:30 – 12:40 Research Presentation 12:40 – 12:45 Final Comments and Adjourn

4
Introductions Who are you? What do you do?
What are your expectations for today’s session?

5
What are the types of handoffs that come to mind when you think about handoffs?

6
“Hand-off Theater”

7
Role Play of a Intern “Sign-out”
Use the checklist for observations: Please record cultural, communication, and environmental barriers that interfere with successful patient hand-off practices in patient care

8
What Do You Look For? Barriers Observations/Thoughts Facilitators
Cultural (e.g., not prioritizing hand-offs, following proper procedures, unprofessional behavior, etc.) Communication (e.g., vague terms, incomplete information, lack of verification, etc.) Environmental (e.g., distractions and obstacles interfering with completing proper hand-off procedure) Other Facilitators What went well?
 Communication (e.g., vague terms, incomplete information, lack of verification, etc.) Environmental (e.g., distractions and obstacles interfering with completing proper hand-off procedure) Other. Facilitators. What went well")
9
Debriefing from the Role Play
What types of barriers to an effective hand-off did you observe? Environment Cultural Communication Any others?

10
Audience Poll: Current Practices in Transfer of Care in Your Institution
When there is a transfer of care, who is primarily responsible for the transfer?

11
Audience Poll: Current Practices in Transfer of Care in Your Institution
How many senders and receivers of information are present at the time of the hand-off?

12
Audience Poll: Current Practices in Transfer of Care in Your Institution
Is a verbal communication required at the time of a hand-off in your institution/program?

13
Audience Poll: Current Practices in Transfer of Care in Your Institution
If conducted, where does verbal communication take place? Face to face in a dedicated room On the phone “On the fly” (wherever/whenever the two parties can meet) At the patient’s bedside
 At the patient’s bedside.")
14
Audience Poll: Current Practices in Transfer of Care in Your Institution
Does your program/institution use a standard template for written information conveyed at the hand-off (“sign-out”)?
")
15
Audience Poll: Current Practices in Transfer of Care in Your Institution
Do you have formal training on how to perform hand-offs and transition patients for new personnel at your institution?

16
Background and Definitions

17
Exchange vs. Hand-off An exchange of information doesn't require that the other person understand what is being transmitted but simply conveys information information is often acquired and transmitted without testing for comprehension A hand-off implies transfer of information as well as professional responsibility Hand-offs with exchange elements that don’t test for comprehension put teams at risk

18
Lessons from Other Industries and Applications to Healthcare

19
Hand-off as a Form of Communication
“When you move from right to left, you lose richness, such as physical proximity and the conscious and subconscious clues. You also lose the ability to communicate through techniques other than words such as gestures and facial expressions. The ability to change vocal inflection and timing to emphasize what you mean is also lost…Finally, the ability to answer questions in real time, are important because questions provide insight into how well the information is being understood by the listener.” –Alistair Cockburn In thinking of the way we communicate, it is important to think about the mode of communication. I use the red arrows to highlight two ends of this spectrum that we use to communicate every day in healthcare: paper and face to face communication. And clearly they are very different and it is important to know how they differ. Esp in the context of signout. This passage from Allistair Cockburn, who is actually a software engineer and prominent author on this topic describes it best: When you move from right to left, you lose richness, such as physical proximity and the conscious and subconscious clues that such proximity provides. You also lose the ability to communicate through techniques other than words such as gestures and facial expressions. The ability to change vocal inflection and timing to emphasize what you mean is also lost…Finally, the ability to answer questions in real time, are important because questions provide insight into how well the information is being understood by the listener.

20
Hand-offs in Other High-Risk Industries
Direct observations of hand-offs at NASA, 2 Canadian nuclear power plants, a railroad dispatch center, and an ambulance dispatch center STRATEGIES Standardize - use same order or template Update information Limit interruptions Face to face verbal update with interactive questioning Structure Read-back to ensure accuracy Now what can we say about communication at the time of Handoffs—here we have to turn to other industries…read slide… Not surprisignly, the main strategies described in this paper resonate with those that have worked in healthcare communication more generally TRANSITION TO JEFF… ********************************************** Human factors researchers noted the same thing as they conducted direct observations of handoffs at NASA Johnson Space center, 2 canadian nuclear power plants, a railroad dispatch center in the US, and an ambulance dispath center in Toronto. From these observations, they identified handoff strategies and face to face verbal update with interactive questioning was definitely a plus… Other things they noted Patterson, Roth, Woods, et al. Intl J Quality Health Care, 2004

21
Applications of Standard Language
“Read-back” Reduces errors in lab reporting “Read-backs” at your neighborhood Drive-Thru But the good news, is that communication can be improved, and that is one goal of today’s workshop. In fact, more structured communication, such as the use of a read-back, similar to your neighborhood drive-thru that confirms your order, reduces errors during telephone reporting of abnormal lab values. **** Barenfanger J, Sautter RL, Lang DL, Collins SM, Hacek DM, Peterson LR. Improving patient safety by repeating (read-back) telephone reports of critical information. Am J Clin Pathol. 2004;121(6):801-3. The recipients were asked to repeat the name of the patient, the test, and the result; the technologists noted this on the form. In addition, they noted the time necessary for the entire phone call and the extra time necessary to ask for the message to be repeated and for it to be repeated. Data $11.25/hour ($0.19/minute or $0.0032/second), the extra time to repeat the message costs the hospital from $0.11 to $0.16 per call ($0.07 per 13 seconds for a laboratory technologist’s time plus $0.04-$0.09 per 13 seconds for the recipient’s time). 29 errors detected during requested read-back of 822 lab results at Northwestern Memorial Hospital. All errors detected and corrected. Barenfanger, Sautter, Lang, et al. Am J Clin Pathol, 2004.
 telephone reports of critical information. Am J Clin Pathol. 2004;121(6): The recipients were asked to repeat the name of. the patient, the test, and the result; the technologists noted. this on the form. In addition, they noted the time necessary. for the entire phone call and the extra time necessary to ask. for the message to be repeated and for it to be repeated. Data. $11.25/hour ($0.19/minute or $0.0032/second), the extra. time to repeat the message costs the hospital from $0.11 to. $0.16 per call ($0.07 per 13 seconds for a laboratory technologist’s. time plus $0.04-$0.09 per 13 seconds for the. recipient’s time). 29 errors detected during requested read-back of 822 lab results at Northwestern Memorial Hospital. All errors detected and corrected. Barenfanger, Sautter, Lang, et al. Am J Clin Pathol,")
22
A Word of Caution on Technology
Computerized sign-out Brigham and Women’s Hospital (Petersen, et al. Jt Comm J Qual Improv, 1998) U Washington (Van Eaton, et al. J Am Coll Surg, 2005) IT solutions alone cannot substitute for a “successful communication act” Human vigilance still required Now lets turn to communication in healthcare…what do we know…first we know that it is indispensible. This is important particularly in the context of future IT solutions which are sometimes touted as the safer. **** Refs: Ash JS, Berg M, Coiera E. Some unintended consequences of information technology in health care: the nature of patient care information system-related errors. J Am Med Inform Assoc. 2004;11(2):121-4. Kilpatrick ES, Holding S. Use of computer terminals on wards to access emergency test results: a retrospective audit. BMJ. 2001;322(7294): The results from 1443/3228 (45%) of urgent requests from accident and emergency and 529/1836 (29%) from the admissions ward were never accessed via the ward terminal. Results from 794/3228 (25%) of accident and emergency requests and 413/1836 (22%) of admissions ward requests were seen within 1 hour of becoming available while a further 491/3228 (15%) and 341/1836 (19%) respectively were accessed between 1 and 3 hours. In up to 43/1443 (3%) of the accident and emergency test results that were never looked at the findings might have led to an immediate change in patient management. CONCLUSIONS: When used as the sole substitute for telephoning results, the provision of terminal access to laboratory results on wards can hinder rather than promote the communication of emergency blood results to healthcare staff. In an emergency room, replacing a phone call for critical lab values with electronic reporting with no verbal communication resulted in 45% (1443/3228) of urgent labs to go unchecked. Ash, Berg, Coiera. JAMIA, 2004; Kilpatrick, Holding, BMJ, 2001.
 U Washington. (Van Eaton, et al. J Am Coll Surg, 2005) IT solutions alone cannot substitute for a successful communication act Human vigilance still required. Now lets turn to communication in healthcare…what do we know…first we know that it is indispensible. This is important particularly in the context of future IT solutions which are sometimes touted as the safer. **** Refs: Ash JS, Berg M, Coiera E. Some unintended consequences of information technology in health care: the nature of patient care information system-related errors. J Am Med Inform Assoc. 2004;11(2): Kilpatrick ES, Holding S. Use of computer terminals on wards to access emergency test results: a retrospective audit. BMJ. 2001;322(7294): The results from 1443/3228 (45%) of urgent requests from accident and emergency and 529/1836 (29%) from the admissions ward were never accessed via the ward terminal. Results from 794/3228 (25%) of accident and emergency requests and 413/1836 (22%) of admissions ward requests were seen within 1 hour of becoming available while a further 491/3228 (15%) and 341/1836 (19%) respectively were accessed between 1 and 3 hours. In up to 43/1443 (3%) of the accident and emergency test results that were never looked at the findings might have led to an immediate change in patient management. CONCLUSIONS: When used as the sole substitute for telephoning results, the provision of terminal access to laboratory results on wards can hinder rather than promote the communication of emergency blood results to healthcare staff. In an emergency room, replacing a phone call for critical lab values with electronic reporting with no verbal communication resulted in 45% (1443/3228) of urgent labs to go unchecked. Ash, Berg, Coiera. JAMIA, 2004; Kilpatrick, Holding, BMJ,")
23
In both aviation and medicine, people depend on technology as the solution…

25
Newer technology doesn’t eliminate error

27
Nor does even newer technology

29
Continued Focus on Hand-offs
July 2003– ACGME set limits for resident duty hours Reduce sleep deprivation and improve patient safety Unintended consequence is increase in number of hand-offs (discontinuity) Safety of hand-off? Error-prone and variable A vulnerable “gap” in patient care In July of 2003, the ACGME set limits on resident duty hours. One reason for these limits was to relieve sleep deprivation in medical trainees. In addition to the limit of 80 hours per week, there was also a maximum of 30 consecutive hours per call shift, otherwise known as the “24+6 rule”. While the ACGME and others, especially in light of recent studies, have been debating the optimal length of a call period, we are ignoring another potential way of relieving fatigue. Naps are a proven method to relieve fatigue in other industries requiring long shifts. In residency programs, naps can be provided by using nigh float (NF) systems. In fact, this type of system was used by internal medicine residency programs prior to the duty hours to provide residents with some rest so they could continue to provide care for patients throughout the next day.
 Safety of hand-off Error-prone and variable. A vulnerable gap in patient care. In July of 2003, the ACGME set limits on resident duty hours. One reason for these limits was to relieve sleep deprivation in medical trainees. In addition to the limit of 80 hours per week, there was also a maximum of 30 consecutive hours per call shift, otherwise known as the 24+6 rule . While the ACGME and others, especially in light of recent studies, have been debating the optimal length of a call period, we are ignoring another potential way of relieving fatigue. Naps are a proven method to relieve fatigue in other industries requiring long shifts. In residency programs, naps can be provided by using nigh float (NF) systems. In fact, this type of system was used by internal medicine residency programs prior to the duty hours to provide residents with some rest so they could continue to provide care for patients throughout the next day.")
30
ACGME Core Competencies
Patient Care Medical Knowledge Professionalism Communication Systems Based Practice Practice Based Learning and Improvement

31
The Role of the Hand-off: Communication and Patient Safety
Transfer of information (content) Different modalities (process) Written Verbal Variable, error-prone Few trainees receive formal education The Joint Commission National Patient Safety Goal (effective Jan 1, 2006) “Requires hospitals to implement a standardized approach to hand-off communications and provide an opportunity for staff to ask and respond to questions about a patient's care” Who signed out today—where? Describe it? Noisy, pager going off, others in the room?
 Different modalities (process) Written. Verbal. Variable, error-prone. Few trainees receive formal education. The Joint Commission National Patient Safety Goal (effective Jan 1, 2006) Requires hospitals to implement a standardized approach to hand-off communications and provide an opportunity for staff to ask and respond to questions about a patient s care Who signed out today—where Describe it Noisy, pager going off, others in the room")
32
How Do We Do At Sharing Information?
Verbal handoffs Interruptions lead to diversion of attention, forgetfulness, and error (Coiera, BMJ 1998) Written handoffs Inconsistent Missing code status, allergies, age, sex (Lee, JGIM 1996)
 Written handoffs. Inconsistent. Missing code status, allergies, age, sex (Lee, JGIM 1996)")
34
A Brief Example of the Difficulties in Communicating
The Purpose of This Exercise To make the distinction between hearing (the biological process of assimilating sound waves) and listening (adding our interpretations of what is being said) To demonstrate the importance of effective communication skills and listening skills to thinking and acting systematically adapted from the Systems Thinking Playbook, Meadows and Sweeney, 1995
 and listening (adding our interpretations of what is being said) To demonstrate the importance of effective communication skills and listening skills to thinking and acting systematically. adapted from the Systems Thinking Playbook, Meadows and Sweeney,")
35
Instructions for Part 1 of the exercise
Everyone take 1 sheet of colored paper There is no talking Close your eyes and do exactly what I tell you to do Our goal is to produce identical patterns with the pieces of paper Fold your paper in half and tear off the bottom right corner of the paper. (Pause and allow the group to try this.) Fold the paper in half again and tear off the upper right hand corner. (Pause) Fold the paper in half again and tear off the lower left hand corner. (Pause) Open your eyes, unfold your paper and hold it out for everyone to see.
 Fold the paper in half again and tear off the upper right hand corner. (Pause) Fold the paper in half again and tear off the lower left hand corner. (Pause) Open your eyes, unfold your paper and hold it out for everyone to see.")
36
Instructions for Part 2 of the exercise
Form groups of 3 or 4 at your table Pick 1 person to be the communicator and the rest will be the listeners Listeners close their eyes Communicators go through at least 3 steps, each step involving a fold and a tear Switch roles and repeat the exercise with your same group but with someone else as the communicator. This time the listeners are allowed to talk, but still have their eyes closed

37
What happened? How would you describe your listening skills?
For those who were communicators, how effective were your skills? Were there any differences in the 3 attempts?

38
How Can We Improve Hand-offs?
Developing a Standard Hand-off Protocol

39
A Model For Developing a Standard Protocol
Principles underlying the model The hand-off protocol will need to be discipline specific Standardization is key for both process and content PROCESS Create a process map CONTENT Create a standard check-list IMPLEMENTATION Leadership and resident buy-in MONITORING Ensure the protocol is in place and identify and resolve barriers

40
Understanding Hand-offs as a Process
“The first step is to draw a flow diagram. Then everyone understands what his job is. If people do not see the process, they cannot improve it.” W.E. Deming, 1993

41
Overview of Process Mapping
A process map or flowchart is a picture of the sequence of steps in a process Useful for Planning a project Describing a process Documenting a standard way for doing a job Building consensus about the process (correct misunderstandings about the process) Detailed process maps are especially helpful to standardize and improve processes For use as an improvement tool, it is important to map the current process, not the desired process
 Detailed process maps are especially helpful to standardize and improve processes. For use as an improvement tool, it is important to map the current process, not the desired process.")
42
Process Mapping Ovals are beginnings and endings
Boxes are steps or activities Diamonds are questions Arrows show sequence and chronology

43
Process Mapping Can be “high-level” to get an overview of the process
Admitted? Patient arrives in ER Assessed in ER No Discharged Yes Diagnosed And Treated Sent to floor

44
Process Mapping Can also be very detailed and “drilled down” to show the details and roles Detailed process maps are especially helpful to standardize and improve processes For use as an improvement tool, it is important to map the current process, not the desired process

45
A Sample Hand-off Process (Internal Medicine)
")
46
Analyzing Process Maps
What is the goal of the process? Does the process work as it should? Are there obvious redundancies or complexities? How different is the current process from the ideal process?

47
Advanced Process Mapping: Identifying Barriers

48
Small Group Exercise Working in small groups, create a process map of an “ideal” hand-off process Identify the type of hand-off Set clear boundaries (where does the process begin and end) Identify key steps and decision points
 Identify key steps and decision points.")
49
Process Mapping Demonstration

50
Debriefing

51
Completing the Hand-Off Protocol
PROCESS Create a process map CONTENT Create a standard check-list IMPLEMENTATION Leadership and resident buy-in MONITORING Ensure the protocol is in place and identify and resolve barriers

52
Determine the Standard Content: ANTICipate
Develop a checklist Have disciplines customize to their needs Can be used to evaluate the quality of hand-offs

53
Beware technical, cultural, and environmental differences
A “one-size fits all” approach does not allow for customization. Environment Although 4 programs had a designated hand-off location, 3 conducted hand-offs wherever convenient Culture One resident describes being a “slave to ‘The List’ [sign-out sheet]” and “information overload” In a different program, only acutely ill patients are on the sign-out Technical While all disciplines hand-off “administrative data” (i.e. name, MRN, room number, etc.), major differences in specific categories Surgical fields: Pre-op consent, post-op checks, etc. Pediatrics: Custodial issues (DCFS, parents, etc.) Common use of some language: “If/Then” for contingency planning
, major differences in specific categories. Surgical fields: Pre-op consent, post-op checks, etc. Pediatrics: Custodial issues (DCFS, parents, etc.) Common use of some language: If/Then for contingency planning.")
54
Discipline-specific fields
Psychiatry check-list Routine fields Admin data Therapeutics To-do If/then Discipline-specific fields Housing Court/legal issues Special instructions etc.

55
Research on Transitions of Care
Resident to resident transitions Inpatient to outpatient transitions

56
University of Chicago Experience with Resident Hand-offs
Internal Medicine Department Study Development and Implementation of Standard Protocols

57
Critical Incident Study of IM Hand-offs
To characterize communication failures during hand-offs and solicit suggestions for improvement Question designed to elicit information about adverse events and near misses Was there anything bad that happened or almost happened last night because the (VERBAL/WRITTEN) sign-out wasn't as good as it could have been? Question designed to elicit information about ideas for improvement Regardless of whether anything went wrong or almost went wrong, and thinking about what should be included in a sign-out, is there anything about the (VERBAL/WRITTEN) sign-out that you received that you think should have been better? Arora, Johnson, et al. Quality and Safety in Healthcare, 2005.
 sign-out wasn t as good as it could have been Question designed to elicit information about ideas for improvement. Regardless of whether anything went wrong or almost went wrong, and thinking about what should be included in a sign-out, is there anything about the (VERBAL/WRITTEN) sign-out that you received that you think should have been better Arora, Johnson, et al. Quality and Safety in Healthcare,")
58
Taxonomy of Sign-out Quality
POOR SIGN-OUT Omissions in Content Medications or Therapies Tests or Consults Medical Problems Active Anticipated Baseline status Code status Rationale of primary team Failure-Prone Processes Lack of Face-to-Face Communication Double Sign-out (“Night Float”) Illegible or Unclear Handwriting EFFECTIVE SIGN-OUT Written Sign-out Patient Content Code status Anticipated problems Active Problems Baseline Exam Pending Test or Consults Overall Features Legible Relevant Accurate Up-to-date Verbal Sign-out Face to Face Anticipate Pertinent Thorough
 Illegible or Unclear Handwriting. EFFECTIVE SIGN-OUT. Written Sign-out. Patient Content. Code status. Anticipated problems. Active Problems. Baseline Exam. Pending Test or Consults. Overall Features. Legible. Relevant. Accurate. Up-to-date. Verbal Sign-out. Face to Face. Anticipate. Pertinent. Thorough.")
59
Development and Implementation of a Standard Protocol
To date, 8 residency programs have participated. Analysis of these protocols demonstrates that the hand-off process is highly variable and discipline-specific. Process and content analysis of protocols yields several themes.

60
1. Understand and attempt to reduce the variation in the process
All disciplines “required” a verbal hand-off BUT due to competing demands (OR, clinic, etc.), this verbal communication sometimes did not occur Educate residents on this important priority Individual-level variation also present “Some residents are better at making themselves available and touching base with you [during the hand-off] than others...”
, this verbal communication sometimes did not occur. Educate residents on this important priority. Individual-level variation also present. Some residents are better at making themselves available and touching base with you [during the hand-off] than others...")
61
2. Hand-off = Transfer of information + professional responsibility
Transfers were at times separated in time and space In one program, departing residents forward their pager to the on-call resident after they provide a verbal hand-off. In another program, the on-call resident transfers a virtual pager to their own pager at a designated time which often occurs well before they receive a verbal hand-off.

62
Neurology Hand-Off Transfer of professional responsibility
Verbal hand-off

63
3. Need to ensure “closed-loop” hand-off communication
In two cases, patient tasks were divided and assigned to other team members To facilitate early departure of a post-call resident (to meet resident duty hour restrictions) BUT results of these tasks were not formally communicated to anyone Residents ensured “closed-loop” communication by building required follow-up on these tasks into the process
 BUT results of these tasks were not formally communicated to anyone. Residents ensured closed-loop communication by building required follow-up on these tasks into the process.")
64
Pediatric Resident Post-Call Hand-Off
“closed-loop” communication

65
4. Keep the focus on patient care: Clear roles and back-up behavior
Anesthesia resident to PACU RN Interdisciplinary hand-off with challenging complex fast-paced environment Clear delineation of responsibility to ensure patient care Anesthesia resident to call out for a bed Unit clerk to respond with bed # PACU RN to hook up monitors Equally important back-up behaviors Can empower participants to focus on the patient care “If nursing delay >30 sec, then resident to hook up monitors and call for RN”

66
Anesthesia Resident to PACU Nurse Hand-Off
Clear delineation of roles/responsibility Back-up Behavior

67
Future work We are still in the early stages of our work
Continue our research Mechanisms of human failures during sign-outs, Human factors and ergonomic issues that impede the sign-out process Perceived risks associated with shift changes by different classes of providers and administrators Understanding shared work better Ultimately, the goal is to identify and implement interventions that can reduce the risks associated with transitions in care

68
Inpatient to Outpatient Transitions of Care at University of Chicago
Our aim was to improve the quality, safety, and continuity of patient care during the transition from inpatient to ambulatory care by developing a model of effective communication between inpatient and ambulatory physicians. Specifically, we: Assessed current methods of communication Developed a model for effective inpatient physician – primary care physician communication. Designed an intervention to evaluate the model for effective inpatient physician – primary care physician communication

69
Methods Focus Groups were conducted with
Hospitalists Primary Care Physicians Internal Medicine residents Patients The focus groups were used to generate the process maps

71
Methods Observations were used to verify and enhance the process

72
Interviews Interviews were conducted with key stakeholders to determine barriers and facilitators to an effective handover process

73
Barrier Representative quote(s) (Hospitalists) Representative quote(s) (PCPs) Unable to correctly identify the PCP But also some notes, we don’t recognize their names so its difficult to know if that’s really a primary care doctor and not some sort of ancillary person—[Resident] The other issue is do they really know who the PCP is? They may see [in the electronic system] like a note from X, but then one from Y, one from Z, and how do they know who’s really the PCP? Finding PCP contact info It’s a little harder to get a hold of the [community-based] physicians so I end up resorting to Googling – [Resident] Sometimes we get a text page, voic , from the [General Medicine] team or they call the nurse…sometimes smoke signals- - Unaware or variable preference of PCP’s You know, this [PCP] wants you to get a hold of him ….but maybe some of them [other PCPs] would say, oh, but the [patient] is in the hospital and you know there’s ten people taking care of them, maybe I don’t need to be called until the next morning - - [Resident] I think there’s a culture of… negative feedback if the team contacts the PCP. PCP says oh fine, but never shows up, that’s a learned behavior, they’re going to be less likely to contact. Contacting PCP not a priority I’m usually busy with multiple admissions so I don’t spend too much time contacting the [primary care] providers right away - - [Resident] With 13 admissions or however many --the priority is taking care of the acute illness and continuity of care falls to number 37 on the list of priorities Fear of losing control I mean there are certain attendings, like some sub-specialists, I mean they want you to call them right away if its like, they have a cough… - - [Resident] I get the sense that people don’t call because they’re worried that you’re going to intrude or do something that prolongs the hospitalization Forgetting or too busy to contact PCP I know in the hospital I’ve just gotten better about [contacting PCP’s] from the beginning of my second year as a resident. Like I didn’t always do it right off the bat so I think that there is a learning curve - - I wonder how big of a component that being super-busy especially when they are under the pressure to leave the hospital by noon, the day that it would make the most sense to contact

74
Putting it All Together
The research informs the improvement work

76
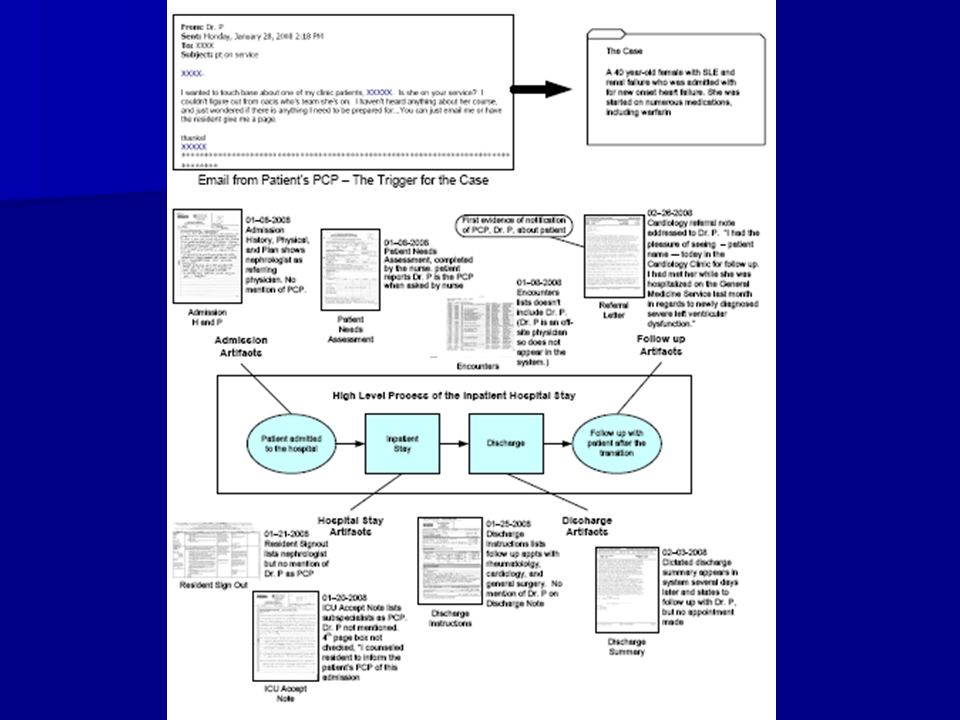
Artifact Analysis The study of any notes or materials used in the daily workflow of patient care may serve as a powerful supplement to the self-report data Provides further evidence of the effectiveness of the handover

78
Concluding Comments

Similar presentations



















” for each unit where.>")





