Download presentation
Presentation is loading. Please wait.

1
CANCER SCREENING 2008: Updates and Evidence
Leah Karliner, MD, MCR Assistant Professor of Medicine Division of General Internal Medicine UCSF

2
OUTLINE Evaluating Screening Tests: general principles
Colon cancer screening: which test is best? Prostate cancer screening: to screen or not to screen? Ovarian cancer: to screen high risk?

3
PRINCIPLES OF SCREENING
Disease has high prevalence Disease has serious consequences Detectable preclinical phase Treatment for presymptomatic disease is more effective than after symptoms develop Positive impact on clinical health outcomes: early detection reduces cancer mortality

4
EFFECTIVENESS OF TEST Tests should be simple, inexpensive and acceptable with a high sensitivity and specificity Number of false positives is acceptably low

5
EFFECTIVENESS OF TEST Questions to be answered when evaluating/comparing tests: Who will be tested? What tests will it supplement or replace? Is the new test safer? Is the new test less costly? Is the test more specific (excluding cases of non-disease)? Is the new test more sensitive (detecting more cases of disease)? Is wide-spread use of the test feasible in practice?
 Is the new test more sensitive (detecting more cases of disease) Is wide-spread use of the test feasible in practice")
6
SCREENING: OTHER CONSIDERATIONS
Involving patients in the decision What are the patient’s co-morbid conditions? Associated life expectancy, feasibility of treatment, effects of treatment on quality of life? What will you do with the results?

7
OUTLINE Colon cancer screening: which test is best?
Evaluating Screening Tests: general principles Colon cancer screening: which test is best? Prostate cancer screening: to screen or not to screen? Ovarian cancer: to screen high risk?

8
COLON CANCER

9
COLORECTAL CANCER: Principles of Screening
Disease has high prevalence: Second most common form of cancer in the U.S. Disease has serious consequences: second highest cancer mortality rate overall in U.S. Detectable preclinical phase – polyps Treatment for pre-symptomatic disease is more effective than after symptoms develop - yes Screening reduces cancer mortality: Several studies have shown that screening with fecal occult blood test (FOBT) or sigmoidoscopy is associated with a reduction in colorectal cancer mortality High prevalence disease with serious consequences. Impact on health outcomes – reduces
 or sigmoidoscopy is associated with a reduction in colorectal cancer mortality. High prevalence disease with serious consequences. Impact on health outcomes – reduces.")
10
COLON CANCER SCREENING RECOMMENDATIONS
U.S. Preventive Services Task Force recommends screening all persons over 50 Benefits of screening outweigh potential harms Quality of evidence, magnitude of benefit and potential harms vary with each method Unclear which is the best test: FOBT, FOBT plus sigmoidoscopy, colonoscopy

11
Changing Incidence Colon cancer incidence rates
decreased for White and Asian-Pacific Islander men and women in U.S. from ; were stable for African American, Latino and Native American men and women; Decrease in incidence largely due to screening and removing pre-cancerous polyps Disparities in incidence rate decline also likely due to disparities in screening rates Espey et al. Annual report to the nation on the status of cancer, , featuring cancer in American Indians and Alaska Natives. Cancer. Oct 15, 2007.

12
AVAILABLE TESTS Tests should be simple, inexpensive and acceptable with a high sensitivity and specificity: ???? Commonly used tests: Fecal occult blood test Sigmoidoscopy Colonoscopy Newer tests: CT Colonography Fecal DNA testing

13
WHICH TEST? Are the tests equally safe? Are the tests equally costly?
Are the tests equally specific? Are the tests equally sensitive? Is wide-spread use of the test feasible in practice?

14
TEST ISSUES Sigmoidoscopy GFOBT FIT (fecal immunochemical test)
Fair evidence for reducing mortality Sigmoidoscopy alone can miss proximal neoplasia – a positive test needs to be followed by colonoscopy GFOBT Good evidence for reducing mortality Trials used 6 sample every 1-2 years Positive test needs to be followed by colonoscopy FIT (fecal immunochemical test) More sensitive than GFOBT; somewhat less specific Specific to human globin; no dietary restrictions; less direct stool handling
 More sensitive than GFOBT; somewhat less specific. Specific to human globin; no dietary restrictions; less direct stool handling.")
15
FIT compared to GFOBT Screening Populations: 3 cohort studies
FIT appear to be more sensitive in detecting CRC and large ≥ 1cm adenomas than Hemoccult II; FIT appear to be somewhat less specific (higher false positive rates) than Hemoccut II FIT GFOBT (Hemoccult II) Sensitivity 57% - 82% 32% - 50% Specificity 95% – 96% 98%
 than Hemoccut II. FIT GFOBT. (Hemoccult II) Sensitivity 57% - 82% 32% - 50% Specificity 95% – 96% 98%")
16
IS COLONOSCOPY “BETTER?”
Two observational studies of patients undergoing colonoscopy Goals: prevalence and location of colonic neoplasia in asymptomatic patients, and Assess risk of proximal advanced neoplasia in patients with or without distal neoplasia Did NOT assess morbidity and mortality

17
IS COLONOSCOPY “BETTER?”
Colonoscopy showed some lesions that would have been missed by sigmoidoscopy alone distal polyps were a predictor of proximal neoplasia, but some patients with proximal neoplasia did not have distal polyps If sigmoidoscopy alone had been done and if every adenomatous polyp triggered colonoscopy, 80% of high risk lesions would have been detected

18
SCREENING COLONOSCOPY?
Would proximal lesions have been detected by FOBT? No assessment of morbidity and mortality

19
SCREENING COLONOSCOPY?
More sensitive than FOBT/sigmoidoscopy More specific than FOBT Higher risk (diagnostic colonoscopies have 1/2000 perforation rate; with polypectomy 1/ ) More costly? (USPSTF says all of these screening methods are probably cost-effective) Presumed to save lives because used as diagnostic test in FOBT studies, but at higher rate than FOBT? Feasibility in practice dependent on availability of gastroenterologists and insurance coverage
 More costly (USPSTF says all of these screening methods are probably cost-effective) Presumed to save lives because used as diagnostic test in FOBT studies, but at higher rate than FOBT Feasibility in practice dependent on availability of gastroenterologists and insurance coverage.")
20
CT COLONOGRAPHY Non-invasive colon imaging method using thin section CT Test characteristics in large 2003 study – 3-D scan N=1,233 average risk individuals, single site Sensitivity 94% for polyps ≥8 mm 89% for polyps ≥6 mm Specificity 96% for polyps ≥10 mm 80% for polyps ≥6 mm Pickhardt, 2003

21
CT COLONOGRAPHY Multicenter study of screening population
615 participants at 9 hospitals Two-dimensional scans Sensitivity 55% for lesions ≥10 mm 39% for lesions ≥6 mm Specificity 96% for lesions ≥10 mm 91% for lesions ≥6 mm Cotton, 2004

22
CT COLONOGRAPHY Kim et al NEJM Oct 4, 2007 Single site; 3-D scans
Comparison of diagnostic findings in two parallel large case series of CT colonography (3,120) and optical colonoscopy (3,163) If CTC patient had polyp ≥6mm then offered same day therapeutic colonoscopy (7.9%) Found similar rates of advanced neoplasia (3.2% vs 3.4%); a few more invasive cancers found on CTC (n=14 vs 4) 5 times as many polypectomies done in colonoscopy group
 and optical colonoscopy (3,163) If CTC patient had polyp ≥6mm then offered same day therapeutic colonoscopy (7.9%) Found. similar rates of advanced neoplasia (3.2% vs 3.4%); a few more invasive cancers found on CTC (n=14 vs 4) 5 times as many polypectomies done in colonoscopy group.")
23
CT COLONOGRAPHY Cornett et al Am J Gastroenterology; June 2008
159 patients with positive result on screening CTC Subsequent optical colonoscopy CTC overall miss rate 18.9% (25/132); but only 6.2% (4/65) for polyps >9mm Of the 4 large polyps missed, 2 had poor CTC colonic distention, 3 were sessile False positive CTC referral (no polyp seen on optical colonoscopy) = 5%
; but only 6.2% (4/65) for polyps >9mm. Of the 4 large polyps missed, 2 had poor CTC colonic distention, 3 were sessile. False positive CTC referral (no polyp seen on optical colonoscopy) = 5%")
24
CT COLONOGRAPHY Requires bowel prep and insufflation
Patients do not necessarily prefer over colonoscopy (50-50 in Kim et al study) Test interpretation is very time consuming Cost effectiveness Assuming 100% sensitivity and specificity To replace colonoscopy, it would have to be less than 50% the cost of colonoscopy and compliance would have to be 15-20% better Sonnenberg, 1999
 Test interpretation is very time consuming. Cost effectiveness. Assuming 100% sensitivity and specificity. To replace colonoscopy, it would have to be less than 50% the cost of colonoscopy and compliance would have to be 15-20% better. Sonnenberg,")
25
FECAL DNA TESTING DNA alterations in colorectal cancer can be detected in the stool Potential advantages Non-invasive No preparation Detection along entire length of the colon

26
FECAL DNA TESTING Evaluated as a screening test in asymptomatic individuals aged 50 and older Fecal DNA test (21 mutations), Hemoccult II and colonoscopy 4404/5486 completed all three aspects of the study Subgroup of 2507 patients were analyzed Imperiale, 2004
, Hemoccult II and colonoscopy. 4404/5486 completed all three aspects of the study. Subgroup of 2507 patients were analyzed. Imperiale,")
27
FECAL DNA TESTING Fecal DNA Hemoccult II
Sensitivity for invasive cancer 51.6% 12.9% Sensitivity for invasive cancer/adenoma with high grade dysplasia 40.8% 14.1% Sensitivity for advanced neoplasia 18.2% 10.8% Specificity

28
FECAL DNA TESTING 20% of the subjects either did not provide samples or did not have colonoscopy Many were aged 65 and over Both FOBT and fecal DNA had relatively low sensitivities compared with what was expected based on prior studies

29
FECAL DNA: REMAINING QUESTIONS
Are health outcomes improved? Even if we assume benefit based on FOBT trials, how much? Do the benefits outweigh the risks? Public expectations about accuracy of DNA testing Frequency of testing? Interval unclear Cost $400 to $800 vs $3 to $40 for FOBT

30
WHICH TEST? Most preventable cases of colon cancer are found in those who have never been screened If we screened with the currently available tests at the recommended intervals, we could make a big impact – particularly in ethnic minorities who have lower screening rates than whites Any screening is better than no screening for reducing colorectal cancer mortality

31
SCREENING FOR HIGH RISK POPULATIONS
Family History 1st degree relative with colon CA or adenomatous polyp diagnosed at age <60, or 2 1st degree relatives with colon ca at any age Screening colonoscopy age 40 or 10 years prior to earliest family diagnosis Repeat screen every 5 years 1st degree relative colon CA/adenomatous polyp diagnosed at age ≥ 60, or two 2nd degree relative with colon ca at any age Screened as average risk persons, starting age 40 Familial Adenomatous Polyposis (FAP) Annual sigmoidoscopy starting age 10-12 HNPCC Colonoscopy q1-2 years beginning age or 10 years prior to earliest CA diagnosis in family
 Annual sigmoidoscopy starting age HNPCC. Colonoscopy q1-2 years beginning age or 10 years prior to earliest CA diagnosis in family.")
32
SCREENING FOR HIGH RISK POPULATIONS
History of Adenomatous Polyps: surveillance based on pathology and number of adenomas at most recent prior colonoscopy Any adenoma w/high grade dysplasia or villous features, or multiple adenomas (≥3) Repeat colonoscopy in 3 years 1-2 small (<1cm) tubular adenomas w/ low grade dysplasia only Repeat colonoscopy in 5 years-10 years
 Repeat colonoscopy in 3 years. 1-2 small (<1cm) tubular adenomas w/ low grade dysplasia only. Repeat colonoscopy in 5 years-10 years.")
33
OUTLINE Prostate cancer screening: to screen or not to screen?
Evaluating Screening Tests: general principles Colon cancer screening: which test is best? Prostate cancer screening: to screen or not to screen? Ovarian cancer: to screen high risk?

34
Prostate Cancer

35
PROSTATE CANCER: SHOULD WE SCREEN?
Disease has high prevalence: Most commonly diagnosed cancer in U.S. men 10% lifetime risk 30% of men have prostate cancer at autopsy Disease has serious consequences: variable; prostate cancer may be a benign disease for many men Detectable preclinical phase – ?PSA Treatment for pre-symptomatic disease is more effective than after symptoms develop - Does early detection do more good than harm or vice versa? Complications of prostate cancer treatment 8.4% incontinence 60% impotence Prostate Cancer Outcomes Study 24 month follow up Screening reduces cancer mortality: ???

37
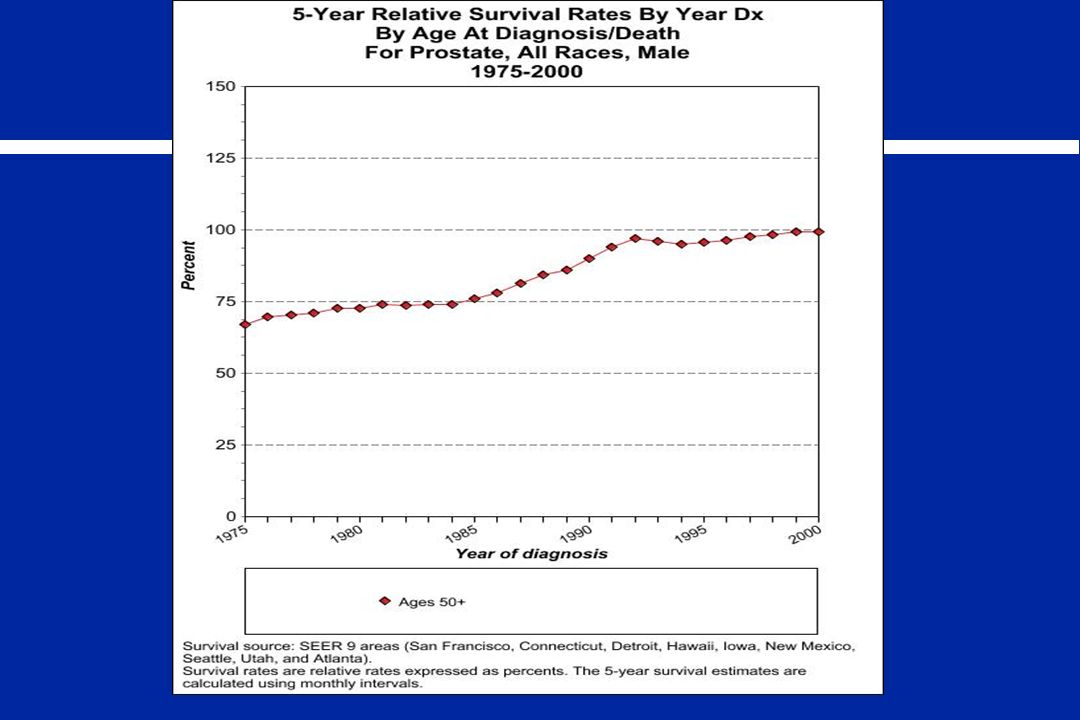
DOES SCREENING DECREASE MORTALITY? EPIDEMIOLOGIC EVIDENCE
Prostate cancer mortality has decreased following the introduction of prostate cancer screening Reduction in mortality followed an initial increase in incidence Due to PSA screening? Changes in treatment? Serendipitous effects of non-cancer-directed treatments?

38
IS TREATMENT OF EARLY DISEASE EFFECTIVE?
Does treatment of early prostate cancer reduce morbidity and mortality? Radical prostatectomy vs. watchful waiting RCT of 695 men reduction in all-cause mortality, reduction in prostate cancer specific mortality, metastatic disease and local progression Absolute reduction in prostate ca specific mortality 30 in prostatectomy group vs. 50 in watchful waiting group 5-year follow-up 2% fewer deaths in prostatectomy group 10 year follow-up 5.3% fewer deaths in prostatecomy group Bill-Axelson, NEJM 2005

39
RANDOMIZED CLINICAL TRIALS
46,000 men underwent DRE and PSA 11 year follow-up 23% of invited group and 6.5% of comparison group underwent screening Decrease in prostate cancer mortality, but small numbers of deaths overall (10/7,348 screened vs. 74/14,231 unscreened: NNS=263) Labrie, Prostate 2004
 Labrie, Prostate")
40
ONGOING RCTs PLCO trial sponsored by the NCI :
Intervention group (38,350) annual screens (PSA x 5 and DRE x 3) vs. usual care (38,355) in healthy men 55-74 Enrolled ; following for 13 years European Randomized Study of Screening for Prostate Cancer (ERSPC) – 8 countries Randomizing close to 220,000 men to screening with PSA, DRE (and for positive tests transrectal ultrasound) vs usual care Results expected “between ”
 annual screens (PSA x 5 and DRE x 3) vs. usual care (38,355) in healthy men Enrolled ; following for 13 years. European Randomized Study of Screening for Prostate Cancer (ERSPC) – 8 countries. Randomizing close to 220,000 men to screening with PSA, DRE (and for positive tests transrectal ultrasound) vs usual care. Results expected between")
41
DIGITAL RECTAL EXAMINATION
One-third of prostate cancers occur in areas which can be reached Higher sensitivity performed by urologists An abnormal digital rectal examination increases the likelihood of prostate cancer somewhat A negative examination does not change the likelihood of a clinically significant prostate cancer Low sensitivity of the examination

42
PSA SCREENING: TEST ISSUES
15% of men over the age of 50 have an elevated PSA PSA >10 ng/ml: 66% have prostate cancer PSA 4-10 ng/ml: 22% have prostate cancer

43
PSA SCREENING: TEST ISSUES
Levels of 4.0 ng/ml or less have typically been considered to be normal Results from the Prostate Cancer Prevention Trial show that prostate cancer is not rare even in these men 27% cancer in those with PSA 3.1 to 4.0 24% in those with PSA 2.1 to 3.0 17% in those with PSA 1.1 to 2.0 10% in those with PSA 0.6 to 1.0 7% in those with PSA up to 0.5 How many cancers would be clinically important? Thompson IM et al, NEJM, 2004

44
Risk Calculation Based on date from the Prostate Cancer Prevention Trial Can use for men ≥ age 50 without a h/o prostate cancer, who have undergone PSA and DRE for screening within the past year Assesses risk for biopsy positive prostate cancer and risk for high grade disease Takes into account: age, ethnicity, PSA and DRE results, history of negative biopsy Thompson IM & Ankert DP; CMAJ June 19, 2007

45
PROSTATE CANCER SCREENING: RECOMMENDATIONS
USPSTF: insufficient evidence to recommend for or against routine screening for prostate cancer using PSA or DRE in men <75 PSA can detect early prostate cancer, but inconclusive evidence about whether early detection improves health outcomes Discussion age (or age 45 for high risk: African American; 1st degree relative with h/o prostate ca) Recommends against screening in men >75 ACP: individualize the decision to screen after discussion with patient about potential benefits and harms ACS: offer PSA and DRE annually starting at age 50, or age for high risk (African American; strong family history); men asking their doctor to decide should be screened
 Recommends against screening in men >75. ACP: individualize the decision to screen after discussion with patient about potential benefits and harms. ACS: offer PSA and DRE annually starting at age 50, or age for high risk (African American; strong family history); men asking their doctor to decide should be screened.")
46
OUTLINE Ovarian cancer: to screen high risk?
Evaluating Screening Tests: general principles Colon cancer screening: which test is best? Prostate cancer screening: to screen or not to screen? Ovarian cancer: to screen high risk?

47
OVARIAN CANCER

48
OVARIAN CANCER: SHOULD WE SCREEN?
Disease has high prevalence: 8th most common cause of CA in women Disease has serious consequences: Usually diagnosed late (>60% stage III or IV): 5th cause of CA death in women High risk group: family history Lifetime risk of ovarian cancer No affected relatives 1.2% One affected relative 5% 2 affected relatives 7% Hereditary syndrome 40% Treatment for pre-symptomatic disease is more effective than after symptoms develop: Ovarian cancer limited to the ovaries is associated with a much higher survival rate Overall 50 year survival: 35% Early stage survival: 90% Does screening decrease mortality: ???
: 5th cause of CA death in women. High risk group: family history. Lifetime risk of ovarian cancer. No affected relatives 1.2% One affected relative 5% 2 affected relatives 7% Hereditary syndrome 40% Treatment for pre-symptomatic disease is more effective than after symptoms develop: Ovarian cancer limited to the ovaries is associated with a much higher survival rate. Overall 50 year survival: 35% Early stage survival: 90% Does screening decrease mortality:")
49
OVARIAN CANCER: SCREENING TECHNIQUES
Serum CA-125 assay Trans-vaginal ultrasound Serum CA-125 plus ultrasound

50
OVARIAN CANCER SCREENING: CLINICAL TRIAL
22,000 U.K. women Annual screening vs no screening for 3 years with 7 year follow-up Screening CA-125 Ultrasound if elevated CA-125 Surgical evaluation if ultrasound abnormal Slight increase in mean survival No difference in mortality Jacobs et al, Lancet 1999

51
OVARIAN CANCER SCREENING: CONCLUSIONS
Many women must be screened to detect a few cases Small increase in survival: Is it worth it? Low disease prevalence limits utility of the tests despite high sensitivity and specificity

52
SCREENING RECOMMENDATIONS
USPSTF: potential harms outweigh potential benefits NIH Consensus Conference: Insufficient evidence Many organizations recommend annual pelvic examination No evidence Although there are no data regarding screening in high risk women (family history; BRCA1 and BRCA2 carriers; HNPCC), experts recommend: annual screening with recto-vaginal pelvic examination, CA-125 and trans-vaginal ultrasound BRCA1 and BRCA2 carriers can consider prophylactic oophorectomy
, experts recommend: annual screening with recto-vaginal pelvic examination, CA-125 and trans-vaginal ultrasound. BRCA1 and BRCA2 carriers can consider prophylactic oophorectomy.")
53
FUTURE TRIALS PLCO Trial
74,000 women aged 55-74 CA-125 at entry and annually for 5 years Annual transvaginal ultrasound 13 year follow-up Novel biomarkers are being investigated United Kingdom Trial of Ovarian Cancer Screening RCT 200,000 women with 7 year follow-up to complete in 2010 CA-125 Ultrasound if elevated CA-125 Surgical evaluation if ultrasound abnormal

54
SUMMARY OF RECOMMENDATIONS
Ovarian cancer: maybe in high risk women only; otherwise await PLCO trial women at high risk should consider oral contraceptives (37% reduction in incidence)
")
55
SUMMARY OF RECOMMENDATIONS
Colon cancer: any screening is better than no screening, use commonly available tests Consider CT colonography if your center has 3-D technology, experienced radiologists, willing patient population, easy access to follow-up colonoscopy Await further research on fecal DNA Prostate cancer: discuss pros and cons of PSA with eligible men age 50-70; await PLCO trial Consider using risk calculation in discussion of screening and in discussion of biopsy

56
WHERE TO GO FOR THE EVIDENCE
U.S. Preventive Services Task Force American Cancer Society Guidelines for Early Detection of Cancer National Cancer Institute Technology Evaluation Center / Blue Cross - Blue Shield Association California Technology Assessment Forum / Blue Shield of California Foundation

57
ADDITIONAL SYLLABUS SLIDES
LUNG CANCER

58
LUNG CANCER

59
LUNG CANCER: Principles of Screening
Disease has high prevalence: In US in 2007, there will be an estimated 213,380 new cases of lung cancer Disease has serious consequences: – #1 cause of cancer mortality for both men & women in US Detectable preclinical phase – ??? Treatment for pre-symptomatic disease is more effective than after symptoms develop – when detected in Stage I, improves 5-year survival from 15% to 40-70% Screening reduces cancer mortality: Neither x-rays nor sputum cytology screening reduces mortality, what about CT scans? High prevalence disease with serious consequences. Impact on health outcomes – reduces

60
LOW DOSE SPIRAL COMPUTERIZED TOMOGRAPHY (LDCT)
Helical, volumetric studies (like conventional chest CT) Continuous data acquisition Scans entire lung in < 20 seconds (single breath hold) No IV contrast More radiation exposure than CXR, less than conventional CT
 Continuous data acquisition. Scans entire lung in < 20 seconds (single breath hold) No IV contrast. More radiation exposure than CXR, less than conventional CT.")
61
Published English-language studies of LDCT screening for lung cancer
1 cross-sectional 6 longitudinal cohort studies 1 randomized control trial – feasibility pilot study comparing LDCT to CXR 4 studies with high risk populations (smokers/former smokers) 4 studies with mixed-risk populations (ranging from 46-86% smokers)
 4 studies with mixed-risk populations (ranging from 46-86% smokers)")
62
Published English-language studies of LDCT screening for lung cancer
Overall the studies show that LDCT: can detect lung cancer tends to detect early stage (Stage I) cancers (53%-93% of cancers found at baseline screen) The studies with high-risk only populations 1.2-2% prevalence of lung cancer on LDCT 0.6-2% incidence of lung cancer on follow-up/annual screens One study compared mortality to historical controls and found no difference (Swenson et al) 2.8/1000 person-years in CT screened population versus 2.0/1000 person years in Mayo Lung Project participants
 cancers (53%-93% of cancers found at baseline screen) The studies with high-risk only populations % prevalence of lung cancer on LDCT % incidence of lung cancer on follow-up/annual screens. One study compared mortality to historical controls and found no difference (Swenson et al) 2.8/1000 person-years in CT screened population versus 2.0/1000 person years in Mayo Lung Project participants.")
63
LDCT screening for lung cancer
Henschke et al Oct 2006 NEJM: results of the International- Early Lung Cancer Action Project (I-ELCAP) 83% smokers; 12% second hand smoke; 5% occupational exposure N=31,567 Extensive protocol for follow-up of abnormal scans Formal adjudication of all cases Longitudinal cohort study Baseline screen by LDCT Follow-up screen for most participants No comparison group
 83% smokers; 12% second hand smoke; 5% occupational exposure. N=31,567. Extensive protocol for follow-up of abnormal scans. Formal adjudication of all cases. Longitudinal cohort study. Baseline screen by LDCT. Follow-up screen for most participants. No comparison group.")
64
LDCT screening for lung cancer
Baseline Screen (n= 31,567) 4,186 positive test 405 (1.3%) lung cancers Annual Screen (n=27,456) 1,460 positive test 74 (0.27%) lung cancers 5 cases interim diagnoses of lung cancer 412/484 (85%) Stage I Estimated 10-year lung cancer specific mortality (average follow-up 5 years) All cancers 20% For Stage I cancers 12%
 4,186 positive test. 405 (1.3%) lung cancers. Annual Screen (n=27,456) 1,460 positive test. 74 (0.27%) lung cancers. 5 cases interim diagnoses of lung cancer. 412/484 (85%) Stage I. Estimated 10-year lung cancer specific mortality (average follow-up 5 years) All cancers 20% For Stage I cancers 12%")
65
Potential Biases Lead-time bias
Screening identifies disease earlier, but does not increase actual survival False increase in apparent survival time by diagnosing cases earlier From: Newman & Kohn, 2006

66
Potential Biases Length-time bias
False increase in apparent survival time by diagnosing more indolent disease From: Newman & Kohn, 2006

67
Potential Biases Overdiagnosis bias (pseudo-disease bias)
False increase in apparent survival time by misclassifying detected abnormality as disease which would never have presented clinically Volunteer bias People who participate in screening trials may be inherently different (healthier) than those who do not --healthier habits, --better access to health care, and --different education and income levels
 than those who do not. --healthier habits, --better access to health care, and. --different education and income levels.")
68
LUNG CANCER SCREENING RECOMMENDATIONS
The U.S. Preventive Services Task Force (USPSTF) evidence is insufficient to recommend for or against screening asymptomatic persons for lung cancer with either low dose computerized tomography (LDCT), chest x-ray (CXR), sputum cytology, or a combination of these tests.
 evidence is insufficient to recommend for or against screening asymptomatic persons for lung cancer with either low dose computerized tomography (LDCT), chest x-ray (CXR), sputum cytology, or a combination of these tests.")
69
LDCT screening for lung cancer: potential harm
Up to 93% of the non-calcified nodules >4mm found in the studies have been false-positives All require follow-up: conventional CT to surgical biopsy All follow-up carries some risk: increased radiation exposure to bleeding/infection/death Risks of higher radiation exposure due to LDCT at regular intervals are unknown

70
LDCT screening for lung cancer
LDCT promising modality to screen for lung cancer and find it early Studies to date have not been designed to account for potential biases Do not yet have convincing data that LDCT screening for lung cancer leads to decreased mortality. Ongoing large NCI RCT: National Lung Screening Trial Results anticipated in 2009

71
Smoking Cessation! Lung cancer incidence rates have stabilized in women and are declining in men in the U.S. True across race-ethnicities Espey et al. Annual report to the nation on the status of cancer, , featuring cancer in American Indians and Alaska Natives. Cancer. Oct 15, 2007.

Similar presentations











: Department.>")







