Download presentation
Presentation is loading. Please wait.

1
Q Prostate D. Robert Siemens, M.D. Queen’s University

2
GU Oncology Prostate Cancer Bladder Cancer Kidney Cancer Testes
20,700 cases, 4200 deaths (2006, CCS) Bladder Cancer 6400 cases, 1700 deaths Kidney Cancer 4600 cases, 1550 deaths Testes 840 cases, 30 deaths
 Bladder Cancer cases, 1700 deaths. Kidney Cancer cases, 1550 deaths. Testes. 840 cases, 30 deaths.")
3
Web Resources http://cancernet.nci.nih.gov/cancertypes.html

4
Objectives To be able to state the two components that can cause bladder obstruction in benign prostatic hyperplasia To be able to state 3 management options for early prostate cancer To understand the importance of the grading of prostate cancer

5
Prostate Diseases Benign Prostatic Hyperplasia (BPH) Prostate Cancer
Prostatitis

6
BPH Prostate size increases with age
Total prostate volume increases from approximately 25 mL for a man in his 30s to 35–45 mL for a man in his 70s Increased cell numbers Balance between cell proliferation and impaired apoptosis Benign prostatic hyperplasia (BPH) can be a progressive condition. In general, prostate volume increases with advancing age; this has been demonstrated in many cross-sectional studies assessing prostate volume by transrectal ultrasound. Studies have found that total prostate volume increases from approximately 25 mL for men in their 30s to 35 to 45 mL for men in their 70s.1 Reference: 1. Roehrborn CG, McConnell JD. Etiology, pathophysiology, epidemiology, and natural history of benign prostatic hyperplasia. In: Walsh PC, Retik AB, Vaughan ED Jr, et al, eds. Campbell’s Urology. 8th ed. Philadelphia, Pa: Saunders; 2002:1297–1336. 7
 can be a progressive condition. In general, prostate volume increases with advancing age; this has been demonstrated in many cross-sectional studies assessing prostate volume by transrectal ultrasound. Studies have found that total prostate volume increases from approximately 25 mL for men in their 30s to 35 to 45 mL for men in their 70s.1. Reference: 1. Roehrborn CG, McConnell JD. Etiology, pathophysiology, epidemiology, and natural history of benign prostatic hyperplasia. In: Walsh PC, Retik AB, Vaughan ED Jr, et al, eds. Campbell’s Urology. 8th ed. Philadelphia, Pa: Saunders; 2002:1297–")
7
BPH Hyperplasia of epithelial (glandular) or stromal (smooth muscle) components Commonly cause lower urinary tract symptoms in men (over 50) Relative obstruction of bladder

11
BPH Risk Factors Male Aging Androgens (testosterone, DHT)
Androgen receptor Intraprostatic 5 alpha reductase Estrogens Apoptosis regulation Stromal-epithelial interactions Growth Factors bFGF, KGF, EGF, TGF-beta, IGF

12
BPH Components Static Dynamic Increased muscle tone
There are two components of obstruction: static or mechanical obstruction due to increased size of glandular tissue and stroma, dynamic obstruction due to increased muscle tone. Benign Prostatic Hyperplasia is an abnormal increase in the number of prostatic cells. Thus, it is responsible only for the static component of obstruction. In the past, Lower Urinary Tract Symptoms (LUTS) were thought to be due exclusively to the static component or BPH. It is now known that the gland size does not correlate with LUTS. It is believed that the dynamic component is critical in this symptomatology. NOTE: Discuss the concept of static versus dynamic obstruction with the audience. This concept will be important later when you discuss medical therapy. Increased muscle tone
 were thought to be due exclusively to the static component or BPH. It is now known that the gland size does not correlate with LUTS. It is believed that the dynamic component is critical in this symptomatology. NOTE: Discuss the concept of static versus dynamic obstruction with the audience. This concept will be important later when you discuss medical therapy. Increased. muscle tone.")
13
Lower Urinary Tract Symptoms (LUTS)
Obstructive (voiding) Irritative (filling) Weak stream Hesitancy Sensation of incomplete emptying Intermittent stream Prolonged urination Frequency Nocturia Urgency Urge incontinence LUTS is a new term for prostatism. LUTS has two types of symptoms: obstructive & irritative. Obstructive symptoms are as listed on the slide. Irritative symptoms are as listed on the slide. NOTE: Questions to ask participants: Can you have BPH without symptoms? (Yes, many men do) Can you have symptoms without BPH? (Yes, women do not have prostates but can have LUTS (see Jepsen JV, et al in Reading below) How does BPH cause different symptoms (hesitancy, weak stream, etc.)? Discuss the applicability of BPH vocabulary – the term should be changed (refer to the previous slide). READING: Jepsen JV, et al. Comprehensive patient evaluation for benign prostatic hyperplasia. Urol 1998;51(Suppl 4A):13-8
 Irritative. (filling) Weak stream. Hesitancy. Sensation of. incomplete emptying. Intermittent stream. Prolonged urination. Frequency. Nocturia. Urgency. Urge incontinence. LUTS is a new term for prostatism. LUTS has two types of symptoms: obstructive & irritative. Obstructive symptoms are as listed on the slide. Irritative symptoms are as listed on the slide. NOTE: Questions to ask participants: Can you have BPH without symptoms (Yes, many men do) Can you have symptoms without BPH (Yes, women do not have prostates but can have LUTS (see Jepsen JV, et al in Reading below) How does BPH cause different symptoms (hesitancy, weak stream, etc.) Discuss the applicability of BPH vocabulary – the term should be changed (refer to the previous slide). READING: Jepsen JV, et al. Comprehensive patient evaluation for benign prostatic hyperplasia. Urol 1998;51(Suppl 4A):13-8.")
14
Differential Diagnosis
Polyuria Bladder dysfunction (diabetes) Myogenic Cystitis Extrinsic pelvic mass Neurogenic Cystolithiasis Bladder cancer Hypertrophy or stenosis of bladder neck BPH Prostate Cancer There are many possible causes of LUTS. BPH is only one of them. These possibilities must be considered when making a diagnosis. READING: Bennett JK, et al. Terazosin for vesicosphincter dyssynergia in spinal cord-injured male patients. Mol Urol 2000;4(4):415-20 Cromie WJ, et al. Anatomical alignment for the connection of buries penis. J Urol 1998;160(4):1482-4 Gaur C, et al. Diabetic autonomic neuropathy causing gall bladder dysfunction. J Assoc Physicians India 2000;48(6):603-5 Glazier DB, et al. Epidermolysis bullosa: a review of the associated urological complications. J Urol 1998;159(6):2122-5 (continued on next page) Holtgrewe HL. Current trends in management of men with lower urinary tract symptoms and benign prostatic hyperplasia. Urol 1998;51(Suppl 4A):1-7 Hopkins SC, et al. Primary carcinoma of male urethra. Urol 1984;23(2):128-33 Kasraeian A. Recent update in benign prostatic hyperplasia. Mattiason A. Management of overactive bladder – looking to the future. Urol 1997;50(Suppl 6A):111-3 Matthiesen TB, et al. Nocturia and polyurea in men referred with lower urinary tract symptoms, assessed using a 7-day frequency-volume chart. BJU Int 1999;83(9): Nzeh DA. Intravenous urographic findings in Burkitt’s lymphoma. Trop Geogr Med 1989;41(3):261-5 Ouslander JG. Aging and the lower urinary tract. Am J Med Sci 1997;314(4):214-8 Rovner ES, et al. The treatment of overactive bladder in the geriatric patient. Clin Geriat 2002;10(1):20-35 Urethral carcinoma Vesicosphincter dyssynergia Urethritis Urethral stricture Stenosis of urinary meatus (Ouslander JG. Am J Med Sci 1997;314(4):214-8; Kasraeian A. other references upon request) Phimosis
 Myogenic. Cystitis. Extrinsic pelvic mass. Neurogenic. Cystolithiasis. Bladder cancer. Hypertrophy or stenosis of bladder neck. BPH. Prostate Cancer. There are many possible causes of LUTS. BPH is only one of them. These possibilities must be considered when making a diagnosis. READING: Bennett JK, et al. Terazosin for vesicosphincter dyssynergia in spinal cord-injured male patients. Mol Urol 2000;4(4): Cromie WJ, et al. Anatomical alignment for the connection of buries penis. J Urol 1998;160(4): Gaur C, et al. Diabetic autonomic neuropathy causing gall bladder dysfunction. J Assoc Physicians India 2000;48(6): Glazier DB, et al. Epidermolysis bullosa: a review of the associated urological complications. J Urol 1998;159(6): (continued on next page) Holtgrewe HL. Current trends in management of men with lower urinary tract symptoms and benign prostatic hyperplasia. Urol 1998;51(Suppl 4A):1-7. Hopkins SC, et al. Primary carcinoma of male urethra. Urol 1984;23(2): Kasraeian A. Recent update in benign prostatic hyperplasia. Mattiason A. Management of overactive bladder – looking to the future. Urol 1997;50(Suppl 6A): Matthiesen TB, et al. Nocturia and polyurea in men referred with lower urinary tract symptoms, assessed using a 7-day frequency-volume chart. BJU Int 1999;83(9): Nzeh DA. Intravenous urographic findings in Burkitt’s lymphoma. Trop Geogr Med 1989;41(3): Ouslander JG. Aging and the lower urinary tract. Am J Med Sci 1997;314(4): Rovner ES, et al. The treatment of overactive bladder in the geriatric patient. Clin Geriat 2002;10(1): Urethral carcinoma. Vesicosphincter dyssynergia. Urethritis. Urethral stricture. Stenosis of urinary meatus. (Ouslander JG. Am J Med Sci 1997;314(4):214-8; Kasraeian A. other references upon request) Phimosis.")
15
-Blockers: Mode of Action
Relaxes prostate and bladder neck smooth-muscle tone By relaxing prostatic smooth muscle, -blockers may relax prostatic pressure on the urethra, increasing flow.1 Reference: 1. Lepor H, Lowe FC. Evaluation and nonsurgical management of benign prostatic hyperplasia. In: Walsh PC, Retik AB, Vaughan ED Jr, et al, eds. Campbell’s Urology. 8th ed. Philadelphia, Pa: Saunders; 2002:1337–1378. 26

16
5-Reductase Inhibitors
Block conversion of testosterone to dihydrotestosterone (DHT) within the prostate 5-Reductase inhibitors block the intraprostatic conversion of testosterone to dihydrotestosterone (DHT), the potent androgen responsible for prostate growth. 33
 within the prostate. 5-Reductase inhibitors block the intraprostatic conversion of testosterone to dihydrotestosterone (DHT), the potent androgen responsible for prostate growth. 33.")
17
Transurethral Resection of Prostate (TURP)
Resectoscope Bladder There are 3 indications for surgical therapy (see READING): Complications Failure of management with pharmacologic therapy Refusal of pharmacologic therapy by the patient The key messages are: Only the central portion of the prostate is removed during TURP. Thus, the patient is at the same risk of having prostate cancer as before the surgery. TURP is a surgical procedure often performed under spinal anaesthesia. The surgeon dissects as much tissue as necessary to achieve the prescribed outcome. The prostatic tissue is then sent to pathology for analysis to determine if there is any malignancy. READING: De la Rosette JJ, et al. EAU Guidelines on benign prostatic hyperplasia (BPH). Eur Urol 2001;40(3):256-63 Prostate Removal of Hypertrophied Tissue
: Complications. Failure of management with pharmacologic therapy. Refusal of pharmacologic therapy by the patient. The key messages are: Only the central portion of the prostate is removed during TURP. Thus, the patient is at the same risk of having prostate cancer as before the surgery. TURP is a surgical procedure often performed under spinal anaesthesia. The surgeon dissects as much tissue as necessary to achieve the prescribed outcome. The prostatic tissue is then sent to pathology for analysis to determine if there is any malignancy. READING: De la Rosette JJ, et al. EAU Guidelines on benign prostatic hyperplasia (BPH). Eur Urol 2001;40(3): Prostate. Removal of Hypertrophied Tissue.")
18
Prostate Cancer is Common!
13% lifetime risk of prostate cancer 3% lifetime risk of dying of prostate cancer

19
Prostate Cancer is Common!
Most common cancer in men (27%) 18,200 new cases in 2002 4316 deaths in 2002 1 death every 13 minutes
 18,200 new cases in deaths in death every 13 minutes.")
20
Prostate Cancer Incidence
Roberts ‘99

21
Risk factors? Male Testosterone Age Others…..
family history, race, diet etc

22
Family History in Prostate Cancer
First degree relative affected ? No RR= 1 x Yes RR= 2-3 x Diagnosed <65 RR= 6 x 3 relatives RR= 11 x

23
GENETICS HPC1 CAG repeats SDR5A2

24
VITAMIN E Antioxidant Plant derived oils
Induces cell cycle arrest in PC-3 , LNCaP ATBC trial 1/3rd reduced 4 yrs 41% reduced 6 years

25
SELENIUM Inconsistent dietary intake Antioxidant
Induces cell cycle arrest in LNCaP Clarke 1312 men with NMSC 200 micrograms selenium as Brewer’s yeast 69 % reduced incidence of CaP

26
SOY Japanese paradox Isoflavones : Genistein / Daidzein Phytoestrogens
Tyrosine kinase inhibition Induce apoptosis in PC-3 / LNCaP

27
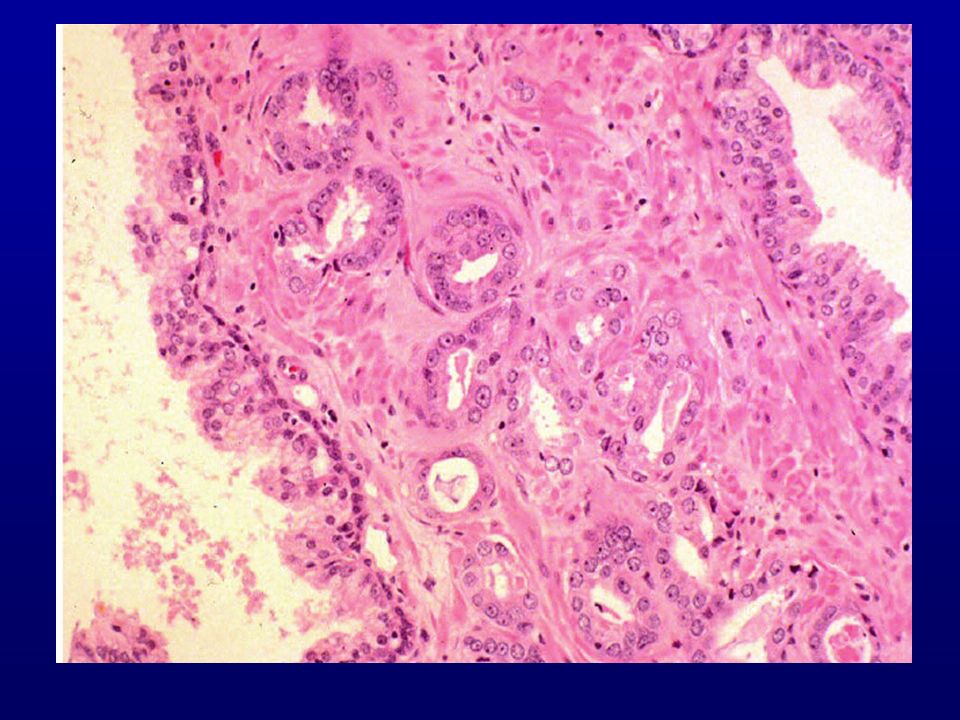
Diagnosis Digital rectal examination PSA PSA test characteristics
Serine protease secreted into lumen of prostate glands Liquefies semen Elevated in BPH, prostate cancer, prostatitis PSA test characteristics PSA 4-10 … cancer risk ~25% PSA >10 … cancer risk ~50-60%

28
Prostate Cancer Stage T1 T3 incidental locally invasive T1a, T1b, T1c
fixation T4a, T4b T2 confined T2a, T2b, T2c

31
Organ Confined Disease Treatment Options
Radical Surgery Radiation (ext beam and brachytherapy) Watchful Waiting
 Watchful Waiting.")
34
Advanced Prostate Cancer

35
Management of Advanced Prostate Cancer
Use hormonal therapy to control progressive or metastatic disease The object of androgen deprivation in the treatment of advanced prostate cancer is to intervene in the cycle of testosterone production and its eventual utilization by cancer cells. Such intervention can reduce the growth stimulus of testosterone on the cancer, often resulting in slowed doubling times and shrinkage of the tumor, and perhaps a delay in development of further metastasis. The most widely established interventions to inhibit testosterone production include castration, either by bilateral orchiectomy (surgical castration) or through administration of an LHRH analog (medical castration). Nonsteroidal antiandrogens inhibit the testosterone cycle by serving as specific androgen receptor antagonists; they have been investigated as monotherapy and in combination therapy with surgical or medical castration in the treatment of advanced prostate cancer. Coffey DS. The molecular biology, endocrinology, and physiology of the prostate and seminal vesicles. In: Walsh PC, Retik AB, Stamey TA, Vaughn ED Jr, eds. Campbell’s Urology. 7th ed. Philadelphia, Pa; WB Saunders; 1997:
 or through administration of an LHRH analog (medical castration). Nonsteroidal antiandrogens inhibit the testosterone cycle by serving as specific androgen receptor antagonists; they have been investigated as monotherapy and in combination therapy with surgical or medical castration in the treatment of advanced prostate cancer. Coffey DS. The molecular biology, endocrinology, and physiology of the prostate and seminal vesicles. In: Walsh PC, Retik AB, Stamey TA, Vaughn ED Jr, eds. Campbell’s Urology. 7th ed. Philadelphia, Pa; WB Saunders; 1997:")
36
Charles Huggins 1901-1998 Awarded Nobel Prize in 1966
Only Canadian-born doctor to win the Nobel Prize in Physiology or Medicine

37
Castration Decrease prostate volume Primary tumor shrinks (30-40%)
Metastatic deposits decrease (40-80%) and disappear (5-10%)
 and disappear (5-10%)")
38
Surgical Castration Immediate and complete castrate levels (0.2 ng/ml)
Adrenal androgens (5-10%) $1940
 $1940.")
39
Medical Castration LH-RH agonists
suppression after initial flare of LH and T castrate levels of T ( ng/ml) in 9 days to 4 weeks need to treat “flare” with antiandrogen
 in 9 days to 4 weeks. need to treat flare with antiandrogen.")
40
Medical Castration LH-RH agonists
goserelin (Zoladex®), leuprolide (Lupron®), buserelin (Suprefact®) depot injections 1 to 3-4 months $ /year
, leuprolide (Lupron®), buserelin (Suprefact®) depot injections 1 to 3-4 months. $ /year.")
41
Adverse Effects Castration loss of libido and potency (>75%)
hot flashes (50-60%) sweating (10%) painful gynecomastia (~1-2%) osteoporosis (5% fracture) cardiovascular effects weight gain, loss of muscle mass
 sweating (10%) painful gynecomastia (~1-2%) osteoporosis (5% fracture) cardiovascular effects. weight gain, loss of muscle mass.")
Similar presentations