Download presentation
Presentation is loading. Please wait.

1
TK Inhibitors in NSCLC Rossana Berardi
Clinica di Oncologia Medica Università Politecnica delle Marche Ospedali Riuniti di Ancona

2
Intracellular mTKI Targets
Vandetanib AKT PI3-K Erlotinib Lapatinib Gefitinib EGFR Proliferation/Survival ERK MEK Raf Ras Sunitinib Sorafenib Motesanib VEGFR MAPK MAPK Src Axitinib Angiogenesis Dasatinib Ras Raf MEK ERK STAT JAK Abl Nilotinib Imatinib PDGFR PI3-K AKT Transcription Metastasis Tumor Cell Endothelial Cell

3
IL TUMORE DEL POLMONE del Sig. Rossi
Obiettivo CURARE IL TUMORE DEL POLMONE del Sig. Rossi CURARE IL TUMORE DEL POLMONE Si va verso una TERAPIA SU MISURA FR Hirsch JTO 2008;3: Ohe Y, Clin Cancer Res Jul 1;14(13): .
:")
4
The Epidermal Growth Factor Pathway
Ciardiello F, et al. EGFR Antagonists in Cancer Treatment. N Engl J Med. 2008:358:

5
TARCEVA indicato nel trattamento di pazienti adulti con
carcinoma polmonare non a piccole cellule (NSCLC) localmente avanzato o metastatico dopo fallimento di uno o più trattamenti chemioterarpici 5
 localmente avanzato o metastatico. dopo fallimento di uno o più trattamenti chemioterarpici")
6
indicazione include la prima linea di trattamento
Approvazione EMEA 24 giugno 2009 IRESSA è indicato nel trattamento di pazienti adulti con carcinoma polmonare non a piccole cellule (NSCLC) localmente avanzato o metastatico con mutazione attivante l’EGFR-TK 6
 localmente avanzato o metastatico. con mutazione attivante l’EGFR-TK")
7
1st/2nd/3rd-Line NSCLC TREATMENT EGFR TKIs Clinical Development Route
GEFITINIB Phase I IDEAL I & II BR.21 ISEL INTACT 1&2 TALENT&TRIBUTE INVITE INTEREST IPASS TRUST Phase II ERLOTINIB 7

8
BR.21 STUDY DESIGN ERLOTINIB* 150 mg daily Placebo “150 mg” daily
NSCLC unsuitable to receive CT stratified by: -Centre -Performance status 0/1 vs 2/3 -Response to prior Rx (CR/PR:SD:PD) -Prior regimens (1 vs 2) -Prior platinum (yes vs no) ERLOTINIB* 150 mg daily R A N D OM I S E * 2:1 randomisation Placebo “150 mg” daily F Shepherd et al, N Eng J Med 2005 8
 -Prior regimens. (1 vs 2) -Prior platinum. (yes vs no) ERLOTINIB* 150 mg daily. R. A. N. D. OM I. S. E. * 2:1 randomisation. Placebo 150 mg daily. F Shepherd et al, N Eng J Med")
9
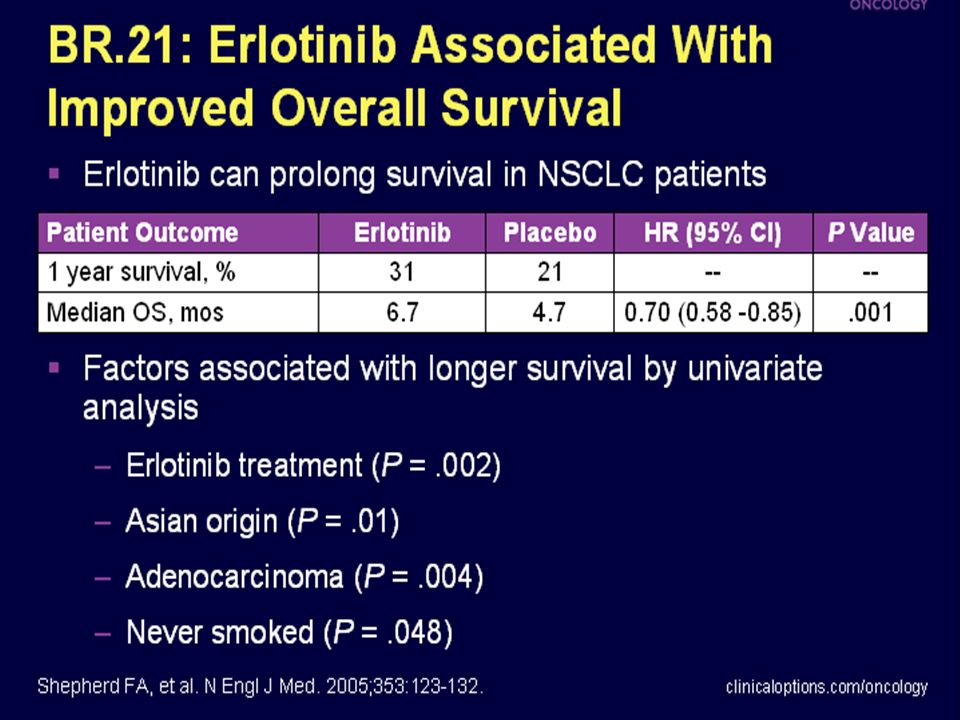
Shepherd FA, et al. N Engl J Med 2005
SECONDA LINEA Sopravvivenza (%) 1.00 0.75 0.50 0.25 Tarceva Placebo Tempo (mesi) Erlotinib prolunga significativamente la sopravvivenza nei pazienti con NSCLC avanzato Un discorso a parte merita Erlotinib che, nell'unico studio pubblicato, è stato confrontato a placebo in pazienti anche pesantemente pretrattatti. L' end point primario era la sopravvivenza globale e quelli secondari la risposta globale, la sopravvivenza libera da progressione, la durata della risposta, la tossicità e la qualità di vita. Rispetto al placebo l'inibitore della tirosin kinasi è certamente più efficace con una mediana di sopravvivenza di 6.7 verso 4,7 mesi, un tasso di risposta del 8.9% con durata di 7.9 mesi, una sopravvivenza libera da progressione di 2.2 mesi verso 1,8 con HR di 0.61, ed infine con un significativo miglioramento della qualità di vita per tosse, dispnea e dolore. I vantaggi, pur presenti, sono abbastanza modesti c'è da dire però che, a parte la tossicità cutanea e la diarrea, il trattamento è certamente ben tollerato Studio registrativo. Br21 Il farmaco, infatti, è stato registrato per il trattamento di seconda linea del NSCLC. Da ricordare riduzione dei sintomi. Autore Terapia N RR (%) PFS Mediana OS (m) 1-aa OS (%) Shepherd Tarceva Placebo 427 211 8.9 <1 2.2 1.8 6.7 4.7 31% 22% Shepherd FA, et al. N Engl J Med 2005
 Tarceva. Placebo. Tempo (mesi) Erlotinib prolunga significativamente la sopravvivenza nei pazienti con NSCLC avanzato Un discorso a parte merita Erlotinib che, nell unico studio pubblicato, è stato confrontato a placebo in pazienti anche pesantemente pretrattatti. L end point primario era la sopravvivenza globale e quelli secondari la risposta globale, la sopravvivenza libera da progressione, la durata della risposta, la tossicità e la qualità di vita. Rispetto al placebo l inibitore della tirosin kinasi è certamente più efficace con una mediana di sopravvivenza di 6.7 verso 4,7 mesi, un tasso di risposta del 8.9% con durata di 7.9 mesi, una sopravvivenza libera da progressione di 2.2 mesi verso 1,8 con HR di 0.61, ed infine con un significativo miglioramento della qualità di vita per tosse, dispnea e dolore. I vantaggi, pur presenti, sono abbastanza modesti c è da dire però che, a parte la tossicità cutanea e la diarrea, il trattamento è certamente ben tollerato. Studio registrativo. Br21 Il farmaco, infatti, è stato registrato per il trattamento di seconda linea del NSCLC. Da ricordare riduzione dei sintomi. Autore. Terapia. N. RR (%) PFS. Mediana. OS (m) 1-aa. OS (%) Shepherd. Tarceva. Placebo < % 22% Shepherd FA, et al. N Engl J Med")
10
TRUST PHASE IV STUDY TaRceva LUng Cancer Survival Treatment
N>7000 in 31 paesi del mondo (531 centri) 10
 10.")
11
TRUST vs BR.21: an indirect comparison
Progression Free Survival in UE Subpopulation 1.00 0.75 0.50 0.25 BR.211 Median PFS: erlotinib 2.2 mo vs placebo 1.8 mo (p<0.001) TRUST2 Median PFS: 3.2 mo Survival distribution function Erlotinib (TRUST), n=6,580 Erlotinib (BR.21), n=488 Placebo (BR.21), n=243 Although a simple comparison is difficult, the median PFS in TRUST was somewhat longer than that reported for the erlotinib treatment arm in BR21. NOTE: this slide contains a PowerPoint animation. Please view in slideshow mode. PFS (months) 1Shepherd FA, et al. N Engl J Med M Reck et al, ESMO 2008
 TRUST2. Median PFS: 3.2 mo. Survival distribution function. Erlotinib (TRUST), n=6,580. Erlotinib (BR.21), n=488. Placebo (BR.21), n=243. Although a simple comparison is difficult, the median PFS in TRUST was somewhat longer than that reported for the erlotinib treatment arm in BR21. NOTE: this slide contains a PowerPoint animation. Please view in slideshow mode PFS (months) 1Shepherd FA, et al. N Engl J Med M Reck et al, ESMO")
12
TRUST vs BR.21: an indirect comparison
Overall Survival in UE Subpopulation 1.00 0.75 0.50 0.25 BR.211 Median OS: erlotinib 6.7 mo vs placebo 4.7 mo (p<0.001) TRUST 2 Median OS: 7.9 months (28% censored) Survival distribution function Erlotinib (TRUST), n=6,580 Erlotinib (BR.21), n=488 Placebo (BR.21), n=243 Survival time (months) 1Shepherd FA, et al. N Engl J Med 2005 2 M Reck et al, ESMO 2008
 TRUST 2. Median OS: 7.9 months (28% censored) Survival distribution function. Erlotinib (TRUST), n=6,580. Erlotinib (BR.21), n=488. Placebo (BR.21), n= Survival time (months) 1Shepherd FA, et al. N Engl J Med M Reck et al, ESMO")
14
NEW OPTIONS IN A-NSCLC Prolongation of Disease Control
It is exactly for these results that it is possible suppose a role for these new biological agents with a sequential use after the induction with active citotoxic drugs for a maintenance of response as a single agent as Roy Herbst has presented during last ASCO meeeting with this slide. RS Herbst et al, ASCO 2003

15
SATURN TRIAL DESIGN F Cappuzzo et al, P ESMO 2009

16
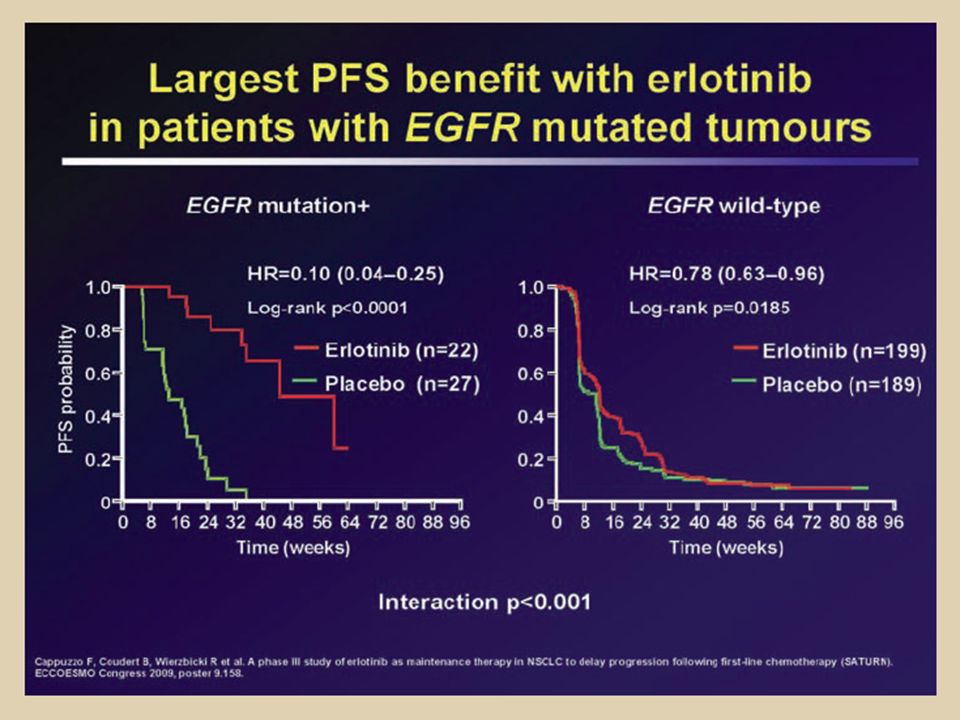
SATURN: PFS (all patients)
PRIMARY END-POINT F Cappuzzo et al, P ESMO 2009

17
SATURN: OS* (all patients, ITT)
1.0 0.8 0.6 0.4 0.2 HR=0.81 (0.70–0.95) Log-rank p=0.0088 OS probability Erlotinib (n=438) Placebo (n=451) 11.0 12.0 Time (months) *OS is measured from time of randomisation into the maintenance phase; ITT = intent-to-treat population F Cappuzzo et al, P ESMO 2009
 Log-rank p= OS probability. Erlotinib (n=438) Placebo (n=451) Time (months) *OS is measured from time of randomisation into the maintenance phase; ITT = intent-to-treat population. F Cappuzzo et al, P ESMO")
18
Subgroup analysis of PFS
HR (95% CI) n 0.71 (0.62–0.82) 884 0.78 (0.66–0.92) 654 0.56 (0.42–0.76) 230 0.75 (0.64–0.88) 744 0.58 (0.38–0.87) 128 0.60 (0.48–0.75) 401 0.76 (0.60–0.95) 359 0.56 (0.38–0.81) 152 0.66 (0.50–0.88) 242 0.80 (0.67–0.97) 490 All Male Female Caucasian Asian Adenocarcinoma Squamous-cell Never smoker Former smoker Current smoker escopfsba_t_2000 escopfsdm_t_2000 for bac and non-bac Escopfss2_t_2000 for smoking status Bac and non-bac are subgroup of adeno. Order needs to be: Adeno bac non-bac Squamous other Check for other races – not available BAC vs Other = escopfsaba_t_2000 SCC/ADK/others = escopfsdm_t_2000 Non-SCC vs others = see mail Race = escopfs2_t_2000 Smoke/Gender = ettpfsgr01_t_2000 Rash = ettpfsgr25_t_2000 0.4 0.6 0.8 1.0 1.2 Favours erlotinib HR Favours placebo
 n (0.62–0.82) (0.66–0.92) (0.42–0.76) (0.64–0.88) (0.38–0.87) (0.48–0.75) (0.60–0.95) (0.38–0.81) (0.50–0.88) (0.67–0.97) 490. All. Male. Female. Caucasian. Asian. Adenocarcinoma. Squamous-cell. Never smoker. Former smoker. Current smoker. escopfsba_t_2000. escopfsdm_t_2000 for bac and non-bac. Escopfss2_t_2000 for smoking status. Bac and non-bac are subgroup of adeno. Order needs to be: Adeno. bac. non-bac. Squamous. other. Check for other races – not available. BAC vs Other = escopfsaba_t_2000. SCC/ADK/others = escopfsdm_t_2000. Non-SCC vs others = see mail. Race = escopfs2_t_2000. Smoke/Gender = ettpfsgr01_t_2000. Rash = ettpfsgr25_t_ Favours erlotinib. HR. Favours placebo.")
19
SATURN: PFS based on histology Squamous-cell carcinoma
Adenocarcinoma Squamous-cell carcinoma PFS probability PFS probability 1.0 0.8 0.6 0.4 0.2 1.0 0.8 0.6 0.4 0.2 HR=0.60 (0.48–0.75) HR=0.76 (0.60–0.95) Log-rank p<0.0001 Log-rank p=0.0148 Erlotinib (n=204) Placebo (n=197) Erlotinib (n=166) Placebo (n=193) Time (weeks) Time (weeks)
 HR=0.76 (0.60–0.95) Log-rank p< Log-rank p= Erlotinib (n=204) Placebo (n=197) Erlotinib (n=166) Placebo (n=193) Time (weeks) Time (weeks)")
20
Zd1839-Iressa in refractary lung cancer
IDEAL 1 (Europe) - GEM/CDDP RR Median OS 250 mg 18. 4% 7.6 mo R 500 mg 19.0% 8.1 mo IDEAL 2 (US) - Carbo/Taxol 250 mg 11.8% 6.1 mo 500 mg 8.8% 6.0 mo
 - GEM/CDDP. RR Median OS. 250 mg 18. 4% 7.6 mo. R. 500 mg 19.0% 8.1 mo. IDEAL 2 (US) - Carbo/Taxol. 250 mg 11.8% 6.1 mo. 500 mg 8.8% 6.0 mo.")
21
INTACT Trials GEM/CDDP + Iressa GEM/CDDP + Placebo
CarboCDDP/Paclitaxel + Iressa CarboCDDP/Paclitaxel + Placebo 1200 patients No differences (October 2002)
")
23
IPASS Study Design Up to six 3-wk cycles Gefitinib 250 mg/day PO
Previously untreated NSCLC patients (N = 1217) Paclitaxel 200 mg/m2 IV on Day 1 + Carboplatin AUC 5-6 mg/mL/min IV on Day 1 (n = 608) Mok TS, et al. N Engl J Med. 2009;361:
 Paclitaxel 200 mg/m2 IV on Day 1 + Carboplatin AUC 5-6 mg/mL/min IV on Day 1. (n = 608) Mok TS, et al. N Engl J Med. 2009;361:")
24
Baseline Characteristics
Gefitinib (n = 609) Paclitaxel/Carboplatin (n = 608) Female, % 79.5 79.1 Median age, yrs (range) 57 (24-84) 57 (25-84) Smoking history, % Nonsmoker Former light smoker 93.8 6.1 93.6 6.2 WHO PS, % 1 2 25.8 64.2 10.0 26.5 62.8 10.7 Disease stage at entry, % IIIB IV Unknown 24.6 75.4 23.7 76.2 0.2 Mok TS, et al. N Engl J Med. 2009;361:
 Paclitaxel/Carboplatin. (n = 608) Female, % Median age, yrs (range) 57 (24-84) 57 (25-84) Smoking history, % Nonsmoker. Former light smoker WHO PS, % Disease stage at entry, % IIIB. IV. Unknown Mok TS, et al. N Engl J Med. 2009;361:")
25
Objective response rate 43% vs 32% p=0.0001
IPASS: PFS e ORR Probability of PFS 1.0 Carboplatin / paclitaxel Gefitinib N Events 609 453 (74.4%) 608 497 (81.7%) 0.8 HR (95% CI) = (0.651, 0.845) p<0.0001 0.6 Median PFS (months) 4 months progression-free 6 months progression-free 12 months progression-free 5.7 61% 48% 25% 5.8 74% 48% 7% 0.4 Primary objective exceeded: Gefitinib demonstrated superiority relative to carboplatin / paclitaxel in terms of PFS 0.2 However, the hazard ratio was not constant over time, as can be seen from the crossing Kaplan Meier curves and the pattern of the 4, 6 and 12 month progression-free rates, favouring carboplatin/paclitaxel for the first 6 months and gefitinib for the remaining 16 months. Because of this crossing of the curves, the median progression-free survival is similar on both treatments, 5.7 months for gefitinib and 5.8 months for carboplatin/paclitaxel. Therefore the medians are clearly not a good reflection of the treatment effect in this study. It is important to note that the hazard ratio, confidence interval and p-value are still valid when interpreted as a representation of the entire study period, i.e. an average. Also, supportive secondary analyses including a log rank test (which does not require curves to be proportional i.e. not crossing) were consistent with the primary analysis. The crossing of the curves is thought to be driven by differences in progression-free survival outcomes for patients with EGFR mutation positive and negative tumours. This will be explained later in the presentation. Reference: Mok et al. ESMO Abstract LBA2. 0.0 4 8 12 16 20 24 Months At risk : Gefitinib 609 363 212 76 24 5 Carboplatin / paclitaxel 608 412 118 22 3 1 Objective response rate 43% vs 32% p=0.0001 25 25
 (81.7%) 0.8. HR (95% CI) = (0.651, 0.845) p< Median PFS (months) 4 months progression-free 6 months progression-free 12 months progression-free % 48% 25% % 48% 7% 0.4. Primary objective exceeded: Gefitinib demonstrated superiority relative to carboplatin / paclitaxel in terms of PFS However, the hazard ratio was not constant over time, as can be seen from the crossing Kaplan Meier curves and the pattern of the 4, 6 and 12 month progression-free rates, favouring carboplatin/paclitaxel for the first 6 months and gefitinib for the remaining 16 months. Because of this crossing of the curves, the median progression-free survival is similar on both treatments, 5.7 months for gefitinib and 5.8 months for carboplatin/paclitaxel. Therefore the medians are clearly not a good reflection of the treatment effect in this study. It is important to note that the hazard ratio, confidence interval and p-value are still valid when interpreted as a representation of the entire study period, i.e. an average. Also, supportive secondary analyses including a log rank test (which does not require curves to be proportional i.e. not crossing) were consistent with the primary analysis. The crossing of the curves is thought to be driven by differences in progression-free survival outcomes for patients with EGFR mutation positive and negative tumours. This will be explained later in the presentation. Reference: Mok et al. ESMO Abstract LBA Months. At risk : Gefitinib Carboplatin / paclitaxel Objective response rate 43% vs 32% p=")
26
EGFR mutations: the strongest predictor of response

27
MUTAZIONI DI EGFR 85% circa di queste mutazioni delezioni multinucleotidiche “in-frame” (ESONE 19) Mutazioni più frequenti: delezione esone 19 o sostituzione L858R dell’esone 21 mutazioni puntiformi (ESONE 21)
")
28
Stratification of NSCLC according to activating mutations
PFS: 14 mo with erlotinib in pts with EGFR mutations Sharma, Haber & Settleman. Nat Rev Cancer 2010

29
BR.21 study: EGFR mutation status predicts response…
Response rate (%) p value EGFR Mutation status1 Wild-type* 106 8 0.05 Mutant† 10 30 EGFR protein expression (IHC)2 Negative 80 4 NS Positive 11 EGFR gene copy number (FISH)2 Negative3 41 2 0.03 Positive3 25 20 …but not survival MS Tsao et al, N Engl J Med 2005
 p value. EGFR Mutation status1. Wild-type* Mutant† EGFR protein expression (IHC)2. Negative NS. Positive. 11. EGFR gene copy number (FISH)2. Negative Positive …but not survival. MS Tsao et al, N Engl J Med")
30
IPASS Baseline Characteristics: EGFR Status
EGFR Mutation Status, % Gefitinib (n = 609) Paclitaxel/Carboplatin (n = 608) Negative 14.9 14.0 Positive • Exon 19 deletion* • Exon 21 L858R* • Exon 20 T790M* • Other* 21.7 10.8 10.5 0.8 0.5 21.2 12.2 7.7 1.0 1.2 Unknown 63.4 64.8 *11 patients had multiple EGFR mutations and are counted for each mutation present. Mok TS, et al. N Engl J Med. 2009;361:
 Paclitaxel/Carboplatin. (n = 608) Negative Positive. • Exon 19 deletion* • Exon 21 L858R* • Exon 20 T790M* • Other* Unknown *11 patients had multiple EGFR mutations and are counted for each mutation present. Mok TS, et al. N Engl J Med. 2009;361:")
31
IPASS: Main Findings: Significance of EGFR Mutation Status
Significant interaction between treatment and EGFR mutation status In EGFR mutation–positive subgroup, significantly longer PFS with gefitinib (HR: 0.48; 95% CI: ; P < .001) In EGFR mutation–negative subgroup, significantly shorter PFS with gefitinib (HR: 2.85; 95% CI: ; P < .001) EGFR Mutation Positive EGFR Mutation Negative 1.0 Events Gefitinib: 97 (73.5%) Pac/carbo: 111 (86.0%) 1.0 Events Gefitinib: 88 (96.7%) Pac/carbo: 70 (82.4%) 0.8 0.8 0.6 HR: (95% CI: ; P < .001) 0.6 Probability of PFS Probability of PFS HR: (95% CI: ; P < .001) 0.4 0.4 Paclitaxel/ carboplatin Gefitinib Paclitaxel/ carboplatin 0.2 0.2 Gefitinib 4 8 12 16 20 24 4 8 12 16 20 24 Mos Since Randomization Mos Since Randomization Mok TS, et al. N Engl J Med. 2009;361: Reproduced with permission. Copyright © 2009 Massachusetts Medical Society. All rights reserved.
 In EGFR mutation–negative subgroup, significantly shorter PFS with gefitinib (HR: 2.85; 95% CI: ; P < .001) EGFR Mutation Positive. EGFR Mutation Negative Events Gefitinib: 97 (73.5%) Pac/carbo: 111 (86.0%) 1.0. Events Gefitinib: 88 (96.7%) Pac/carbo: 70 (82.4%) HR: 0.48 (95% CI: ; P < .001) 0.6. Probability of PFS. Probability of PFS. HR: 2.85 (95% CI: ; P < .001) Paclitaxel/ carboplatin. Gefitinib. Paclitaxel/ carboplatin Gefitinib Mos Since Randomization. Mos Since Randomization. Mok TS, et al. N Engl J Med. 2009;361: Reproduced with permission. Copyright © 2009 Massachusetts Medical Society. All rights reserved.")
32
IPASS Main Findings: Response Rates
Significantly higher ORR with gefitinib than carboplatin- paclitaxel Driven by EGFR mutation–positive subgroup Significantly higher quality of life improvements with gefitinib than paclitaxel/carboplatin Rates of symptom reduction similar between arms ORR, % Gefitinib Paclitaxel/ Carboplatin P Value Overall population 43.0 32.2 < .001 EGFR mutation positive 71.2 47.3 EGFR wild type 1.1 23.5 .001 Mok TS, et al. N Engl J Med. 2009;361:

33
IPASS: diversa Risposta Tumorale nei pz EGFR M+ ed EGFR M-
Odds ratio >1 implica una maggior probabilità di risposta con gefitinib Gefitinib Carboplatino/ paclitaxel EGFR M+ odds ratio (IC 95%) = 2.75 ( ), p<0.0001 EGFR M- odds ratio (IC 95%) = 0.04 (0.01 to 0.27), p=0.0001 71,2% Risposta tumorale (%) 47,31% 23,5% 1,1% (n=132) (n=129) (n=91) (n=85) Mok T NEJM 2009 33 33
 = 2.75 ( ), p< EGFR M- odds ratio (IC 95%) = 0.04 (0.01 to 0.27), p= ,2% Risposta. tumorale. (%) 47,31% 23,5% 1,1% (n=132) (n=129) (n=91) (n=85) Mok T NEJM")
34
IPASS: Superior quality of life and symptom improvement rates for gefitinib in EGFR mutation positive patients p<0.0001 p<0.0001 p=0.0003 % patients with sustained clinically relevant improvement Quality of life was assessed using the FACT-L total score and the FACT-L Trial Outcome Index. Symptoms were assessed using the FACT-L Lung Cancer Subscale (LCS). Clinically relevant improvement was pre-defined as a 6-point improvement for FACT-L and TOI; 2-point improvement for LCS, maintained for at least 21 days. This graph shows statistically significant increased outcomes for gefitinib compared with carboplatin/paclitaxel doublet chemotherapy in clinically relevant and validated measures of QoL and symptom improvement: Lung Cancer Subscale, Trial Outcome Index and Total FACT-L. In summary, the data presented demonstrate that patients should be assessed for a tumour biomarker to clearly identify those patients that will have a better outcome with gefitinib compared with carboplatin/paclitaxel. Reference: Mok et al. ESMO Abstract LBA2. p-values from logistic regression with covariates. Post-hoc analysis, EFQ population Clinically relevant improvement pre-defined as 6-point improvement for FACT-L and TOI; 2-point improvement for LCS, maintained for at least 21 days. EFQ, evaluable for quality of life; FACT-L, Functional Assessment of Cancer Therapy-Lung; TOI, Trial Outcome Index; LCS, Lung Cancer Subscale 34 34
. Clinically relevant improvement was pre-defined as a 6-point improvement for FACT-L and TOI; 2-point improvement for LCS, maintained for at least 21 days. This graph shows statistically significant increased outcomes for gefitinib compared with carboplatin/paclitaxel doublet chemotherapy in clinically relevant and validated measures of QoL and symptom improvement: Lung Cancer Subscale, Trial Outcome Index and Total FACT-L. In summary, the data presented demonstrate that patients should be assessed for a tumour biomarker to clearly identify those patients that will have a better outcome with gefitinib compared with carboplatin/paclitaxel. Reference: Mok et al. ESMO Abstract LBA2. p-values from logistic regression with covariates. Post-hoc analysis, EFQ population Clinically relevant improvement pre-defined as 6-point improvement for FACT-L and TOI; 2-point improvement for LCS, maintained for at least 21 days. EFQ, evaluable for quality of life; FACT-L, Functional Assessment of Cancer Therapy-Lung; TOI, Trial Outcome Index; LCS, Lung Cancer Subscale")
37
ESMO 2010 Efficacy results from the randomised phase III OPTIMAL (CTONG 0802) study comparing first-line erlotinib versus carboplatin (CBDCA) plus gemcitabine (GEM), in Chinese advanced non-small-cell lung cancer (NSCLC) patients (pts) with EGFR activating mutations Caicun Zhou,1 Yi-long Wu,2 Gongyan Chen,3 Jifeng Feng,4 Xiaoqing Liu,5 Changli Wang,6 Shucai Zhang,7 Jie Wang,8 Songwen Zhou,1 Shengxiang Ren,1 on behalf of the OPTIMAL investigators 1Shanghai Pulmonary Hospital, Tongji University, Shanghai; 2Guangdong Lung Cancer Institute, Guangdong General Hospital & Guangdong Academy of Medical Sciences, Guangzhou; 3The Cancer Hospital of Harbin Medical University, Harbin; 4Jiangsu Province Cancer Hospital, Nanjing; 5307 Hospital of the Academy of Military Medical Sciences, Cancer Center, Beijing; 6Tianjin Cancer Hospital, Tianjin; 7Beijing Chest Hospital, Beijing; 8Peking University School of Oncology, Beijing Cancer Hospital, Beijing; China
 study comparing first-line erlotinib versus carboplatin (CBDCA) plus gemcitabine (GEM), in Chinese advanced non-small-cell lung cancer (NSCLC) patients (pts) with EGFR activating mutations. Caicun Zhou,1 Yi-long Wu,2 Gongyan Chen,3 Jifeng Feng,4 Xiaoqing Liu,5 Changli Wang,6 Shucai Zhang,7 Jie Wang,8 Songwen Zhou,1 Shengxiang Ren,1 on behalf of the OPTIMAL investigators. 1Shanghai Pulmonary Hospital, Tongji University, Shanghai; 2Guangdong Lung Cancer Institute, Guangdong General Hospital & Guangdong Academy of Medical Sciences, Guangzhou; 3The Cancer Hospital of Harbin Medical University, Harbin; 4Jiangsu Province Cancer Hospital, Nanjing; 5307 Hospital of the Academy of Military Medical Sciences, Cancer Center, Beijing; 6Tianjin Cancer Hospital, Tianjin; 7Beijing Chest Hospital, Beijing; 8Peking University School of Oncology, Beijing Cancer Hospital, Beijing; China.")
38
OPTIMAL study design R Erlotinib 150mg/day Chemonaїve
Stage IIIB/IV NSCLC EGFR Act Mut+ (exon 19 deletion or exon 21 L858R mutation) ECOG PS 0–2 (n=165) R 1:1 Gemcitabine (1,000 mg/m2 d1,8) Carboplatin (AUC5 d1) q3w, up to 4 cycles Primary endpoint Progression-free survival (PFS) Secondary endpoints Overall survival (OS), objective response rate (ORR), time to disease progression, duration of response, safety, HRQoL (FACT-L, LCSS), exploratory biomarker analyses Stratification factors Mutation type Histology Smoking status Efficacy assessment Every 6 weeks Act Mut+ = activating mutations; ECOG = Eastern Cooperative Oncology Group; PS = performance status HRQoL = health-related quality of life; FACT-L = Functional Assessment of Cancer Therapy-Lung; LCSS = lung cancer symptom scale 38 38
 ECOG PS 0–2. (n=165) R. 1:1. Gemcitabine (1,000 mg/m2 d1,8) Carboplatin (AUC5 d1) q3w, up to 4 cycles. Primary endpoint. Progression-free survival (PFS) Secondary endpoints. Overall survival (OS), objective response rate (ORR), time to disease progression, duration of response, safety, HRQoL (FACT-L, LCSS), exploratory biomarker analyses. Stratification factors. Mutation type. Histology. Smoking status. Efficacy assessment. Every 6 weeks. Act Mut+ = activating mutations; ECOG = Eastern Cooperative Oncology Group; PS = performance status HRQoL = health-related quality of life; FACT-L = Functional Assessment of Cancer Therapy-Lung; LCSS = lung cancer symptom scale")
39
OPTIMAL PFS: primary analysis (ITT)
1.0 0.8 0.6 0.4 0.2 Erlotinib (n=82) Gem/carbo (n=72) HR=0.16 (0.10–0.26) Log-rank p<0.0001 PFS probability Time (months) Patients at risk Erlotinib Gem/carbo
 Gem/carbo (n=72) HR=0.16 (0.10–0.26) Log-rank p< PFS probability Time (months) Patients at risk. Erlotinib Gem/carbo")
40
OPTIMAL PFS: updated analysis (ITT)
1.0 0.8 0.6 0.4 0.2 Erlotinib (n=82) Gem/carbo (n=72) HR=0.16 (0.10–0.26) Log-rank p<0.0001 PFS probability 4.6 13.1 Time (months) Patients at risk Erlotinib Gem/carbo
 Gem/carbo (n=72) HR=0.16 (0.10–0.26) Log-rank p< PFS probability Time (months) Patients at risk. Erlotinib Gem/carbo")
41
Subgroup analysis of PFS
Overall Stage IV Stage IIIB Female Male Age ≥65 Age <65 PS 0–1 PS 2 Never smoker Current/former smoker Adenocarcinoma Non-adenocarcinoma 0.16 (0.10–0.26) 154 0.18 (0.11–0.28) 138 0.27 (0.06–1.16) 16 0.13 (0.07–0.24) 91 0.26 (0.14–0.50) 63 0.17 (0.07–0.43) 38 0.19 (0.11–0.31) 116 0.16 (0.10–0.26) 144 0.21 (0.04–1.28) 10 0.14 (0.08–0.25) 109 0.21 (0.09–0.49) 45 0.17 (0.11–0.28) 134 0.22 (0.06–0.73) 20 HR (95% Cl) n HR Favours erlotinib Favours gem/carbo
 (0.11–0.28) (0.06–1.16) (0.07–0.24) (0.14–0.50) (0.07–0.43) (0.11–0.31) (0.10–0.26) (0.04–1.28) (0.08–0.25) (0.09–0.49) (0.11–0.28) (0.06–0.73) 20. HR (95% Cl) n HR. Favours erlotinib. Favours gem/carbo.")
42
DCR = disease control rate (CR + PR + SD)
Best tumour response* Erlotinib [n=82] n (%) Gem/carbo [n=72] CR 2 (2) 0 (0) PR 66 (81) 26 (36) ORR 68 (83) p<0.0001 SD 11 (13) 33 (46) DCR 79 (96) 59 (82) p=0.002 PD 3 (4) 12 (17) *in evaluable patients; CR = complete response; PR = partial response; SD = stable disease; DCR = disease control rate (CR + PR + SD)
 Gem/carbo. [n=72] CR. 2 (2) 0 (0) PR. 66 (81) 26 (36) ORR. 68 (83) p< SD. 11 (13) 33 (46) DCR. 79 (96) 59 (82) p= PD. 3 (4) 12 (17) *in evaluable patients; CR = complete response; PR = partial response; SD = stable disease; DCR = disease control rate (CR + PR + SD)")
43
K-RAS mutations?

44
Mutazioni k-RAS: fattore prognostico negativo e fattore predittivo di resistenza primaria ai TKI

45
Resistance to EGFR TK inhibitors

46
Acquired resistance to EGFR TK inhibitors
MET amplification: Proto-oncogene detected in 4 of 18 pts with initial response to gefitinib or erlotinib, who then had progressive disease Found to cause resistance by ErbB3 (HER3)- dependent activation of PI3K Inhibition of MET signaling in these cells restored sensitivity to gefitinib Engelman et al, Science 2007; 316: Amplificazione MET responsabile del 10-20% delle resistenze ai TKI per attivazione attraverso HER3 di PI3K e AKT (indipendente da EGFR)
- dependent activation of PI3K. Inhibition of MET signaling in these cells restored sensitivity to gefitinib. Engelman et al, Science 2007; 316: Amplificazione MET responsabile del 10-20% delle resistenze ai TKI per attivazione attraverso HER3 di PI3K e AKT (indipendente da EGFR)")
47
ARQ-197=oral c-met inhibitor
Dual EGFR-MET inhibition for overcoming MET-mediated resistance to EGFRinhibitors ARQ-197=oral c-met inhibitor

50
Tumor cell proliferation
ALK Pathway Or Inversion Translocation ALK ALK fusion protein* Cell survival PI3K BAD AKT STAT3/5 mTOR S6K RAS MEK ErK PLC-Y PIP2 IP3 Tumor cell proliferation *Subcellular localization of the ALK fusion gene, while likely to occur in the cytoplasm, is not confirmed.1,2 1. Inamura K et al. J Thorac Oncol 2008;3:13– Soda M et al. Proc Natl Acad Sci U S A 2008;105:19893–19897 Figure based on: Chiarle R et al. Nat Rev Cancer 2008;8(1):11–23; Mossé YP et al. Clin Cancer Res 2009;15(18):5609–5614; and Data on file. Pfizer Inc. 50
:11–23; Mossé YP et al. Clin Cancer Res 2009;15(18):5609–5614; and Data on file. Pfizer Inc. 50.")
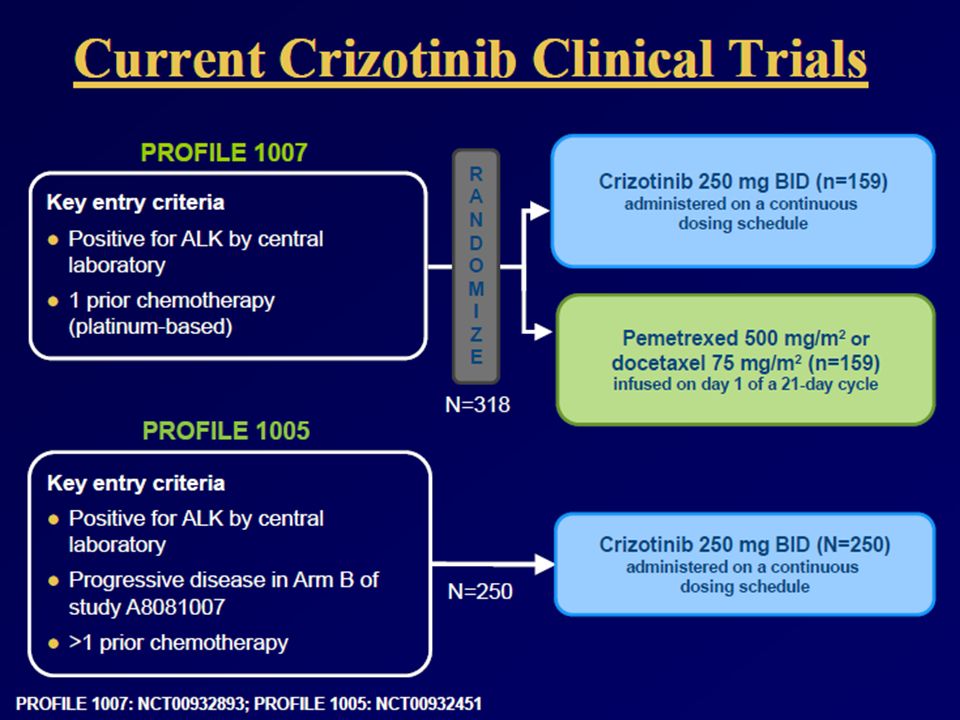
52
Clinical Activity of the Oral ALK Inhibitor, Crizotinib (PF ), in Patients with ALK-positive Non-Small Cell Lung Cancer Bang Y,1 Kwak EL,2 Shaw A,2 Camidge DR,3 Iafrate AJ,2 Maki RG,4 Solomon B,5 Ou SI,6 Salgia R,7 Clark J2 1Seoul National University, Seoul, Korea; 2Massachusetts General Hospital, Boston, MA, USA; 3University of Colorado Cancer Center, Aurora, CO, USA; 4Memorial Sloan-Kettering Cancer Center, New York, NY, USA; 5Peter MacCallum Cancer Centre, East Melbourne, Australia; 6University of California at Irvine, Irvine, CA, USA; 7University of Chicago Cancer Center, Chicago, IL, USA Abstract 3 ASCO Annual Meeting 2010

53
Patients with ALK-positive NSCLC Do not Appear to Respond to EGFR TKIs
Platinum-based chemotherapy EGFR TKI TTP for EGFR TKI1 TTP for chemotherapy1 Months 12 24 36 48 60 100 80 40 20 EML4–ALK EGFR WT/WT % *WT/WT = wild type: no ALK fusion or EGFR mutation 1Shaw AT et al. J Clin Oncol 2009;27:4247–4253

54
Crizotinib Selectivity Profile
Upstate 102 kinase Cellular selectivity on 10 of 13 relevant hits Kinase IC50 (nM) mean* Selectivity ratio c-MET 8 – ALK 20 2X RON 298 34X 189 22X Axl 294 322 37X Tie-2 448 52X Trk A 580 67X Trk B 399 46X Abl 1,159 166X IRK 2,887 334X Lck 2,741 283X Sky >10,000 >1,000X VEGFR2 PDGFR Crizotinib (PF ) 13 kinase “hits” <100X selective for c-MET Crizotinib: inhibits ALK and c-met Selectivity findings Crizotinib – ALK and c-MET inhibition at clinically relevant dose levels Crizotinib – low probability of pharmacologically relevant inhibition of any other kinase at clinically relevant dose levels *The cellular kinase activities were measured using ELISA capture method
 mean* Selectivity ratio. c-MET. 8. – ALK X. RON X X. Axl X. Tie X. Trk A X. Trk B X. Abl. 1, X. IRK. 2, X. Lck. 2, X. Sky. >10,000. >1,000X. VEGFR2. PDGFR Crizotinib (PF ) 13 kinase hits <100X selective for c-MET. Crizotinib: inhibits ALK and c-met. Selectivity findings. Crizotinib – ALK and c-MET inhibition at clinically relevant dose levels. Crizotinib – low probability of pharmacologically relevant inhibition of any other kinase at clinically relevant dose levels. *The cellular kinase activities were measured using ELISA capture method.")
55
Clinical and Demographic Features of Patients with ALK-positive NSCLC
Mean (range) age, years 51 (25–78) Gender, male/female 43/39 Performance status,* n (%) 24 (29) 1 44 (54) 2 13 (16) 3 1 (1) Race, n (%) Caucasian 46 (56) Asian 29 (35) Smoking history, n (%) Never smoker 62 (76) Former smoker 19 (23) Current smoker Histology, n (%) Adenocarcinoma 79 (96) Squamous Other 2 (2) Prior treatment regimens, n (%) 5 (6) 27 (33) 15 (18) ≥3 34 (41) Not reported *Performance status = Eastern Cooperative Oncology Group
 age, years. 51 (25–78) Gender, male/female. 43/39. Performance status,* n (%) 24 (29) (54) (16) 3. 1 (1) Race, n (%) Caucasian. 46 (56) Asian. 29 (35) Smoking history, n (%) Never smoker. 62 (76) Former smoker. 19 (23) Current smoker. Histology, n (%) Adenocarcinoma. 79 (96) Squamous. Other. 2 (2) Prior treatment regimens, n (%) 5 (6) 27 (33) 15 (18) ≥3. 34 (41) Not reported. *Performance status = Eastern Cooperative Oncology Group.")
56
Tumor Responses to Crizotinib for Patients with ALK-positive NSCLC
60 40 20 –20 –40 –60 –80 –100 Progressive disease Stable disease Confirmed partial response Confirmed complete response Maximum change in tumor size (%) –30% * *Partial response patients with 100% change have non-target disease present
 –30% * *Partial response patients with 100% change have non-target disease present.")
57
PFS probability at 6 months: 72%
Treatment with crizotinib resulted in impressive clinical activity in patients with ALK-positive advanced NSCLC ORR: 57% DCR at 8 weeks: 87% PFS probability at 6 months: 72% 57

58
Median PFS has Not been Reached 70% of Patients in Follow-up for PFS
1.00 0.75 0.50 0.25 0.00 Progression-free survival probability Progression-free survival (months) PFS probability at 6 months: 72% (95% CI: 61, 83%) Median follow-up for PFS: 6.4 months (25–75% percentile: 3.5–10 months) 95% Hall–Wellner confidence bands
 PFS probability at 6 months: 72% (95% CI: 61, 83%) Median follow-up for PFS: 6.4 months. (25–75% percentile: 3.5–10 months) 95% Hall–Wellner confidence bands.")
59
Treatment-related Grade 3/4 Adverse Events in ALK-positive NSCLC
Grade 3 n (%) Grade 4 n (%) Any adverse event 10 (12) 1 (1) ALT elevation* 4 (5) AST elevation 5 (6) Lymphopenia 2 (2) Hypophosphatemia Neutropenia Hypoxia Dyspnea Pulmonary embolism *Based on laboratory data (n=71), ALT increase to grade 1, 52%; to grade 2, 4% (In preclinical toxicology studies, no histologic changes in the liver were observed) 1 patient discontinued for ALT elevation
 Grade 4. n (%) Any adverse event. 10 (12) 1 (1) ALT elevation* 4 (5) AST elevation. 5 (6) Lymphopenia. 2 (2) Hypophosphatemia. Neutropenia. Hypoxia. Dyspnea. Pulmonary embolism. *Based on laboratory data (n=71), ALT increase to grade 1, 52%; to grade 2, 4% (In preclinical toxicology studies, no histologic changes in the liver were observed) 1 patient discontinued for ALT elevation.")
61
A-NSCLC Clinical Practice 1st-Line Options in 2010
EGFR Mut+ PTS Gefitinib P-based Doublets: Cis+Gemcitabine Cis+Docetaxel better than Cis+Vin or Cb+Pac P-based CT+Cetuximab(*) SQUAMOUS & NOS PTS P-based Doublets: Cis+Pemetrexed better than Cis+ Gemcitabine P-based CT (**)+ Bevacizumab in selected patients (**) Cb+Pac > Cis+Gem NON SQUAMOUS LC PTS P-based CT+Cetuximab (*) (*) According to registration for EGFR status and CT Courtesy Dr De Marinis 61
 SQUAMOUS. & NOS PTS. P-based Doublets: Cis+Pemetrexed. better than. Cis+ Gemcitabine. P-based CT (**)+ Bevacizumab. in selected patients. (**) Cb+Pac > Cis+Gem. NON SQUAMOUS. LC PTS. P-based CT+Cetuximab (*) (*) According to registration for. EGFR status and CT. Courtesy Dr De Marinis. 61.")
62
Progressi nel 2010?

63
We will need strategies…

64
GREAT (Group REsearch And Trials)
MD Oncologists: Azzurra Onofri Data Managers: Alessandra Lucarelli Chiara Pierantoni Michela Burattini Research Nurse: Fabiana Marcucci Chest Surgeons: Armando Sabbatini Pathologist: Alfredo Santinelli Alessandro Brunelli Pharmacists: Celestino Bufarini Radiologist: Gianluca Valeri Andrea Marinozzi

Similar presentations












 Department of Clinical Oncology>")











