Download presentation
Presentation is loading. Please wait.

1
Mass Screening Using Tandem Mass Spectrometry: Friend or Foe?
Dawn C. Allain, MS, CGC Children’s Hospital of Wisconsin Each year about 4 million newborns in the US have dried blood spots analyzed through state run NBS programs. The screening is performed to identify infants with disorders that if untreated can result in early mortality or lifelong disability. Recent use of the tandem mass spectrometer has allowed for changes in our traditional newborn screening services leading to expansion and improvement of testing. The focus of my talk to this morning will be to provide you with an overview of the methodology involved in utilizing tandem mass spectrometry for newborn screening, as well as a discussion regarding the follow-up involved with positive tandem mass spectrometry NBS results.

2
History of NBS 1957 - Dr. Centerwall 1961 - Dr. Guthrie
MA and OR implement legislation In 1957, Dr. Willard Centerwall, a fellow at Children’s Hospital of Los Angeles and a father of a child with mental retardation, discovered that application of a ferric chloride solution to a wet diaper of a baby with untreated PKU would produce a green color. This test was the first step toward mass screening for PKU, although it was not reliable until a child was several weeks old and damage had already occurred We all recognize the name of Dr. Robert Guthrie, who was not only the father of a child with mental retardation, but the uncle of a child who had PKU. It was Dr. Guthri who developed the bacterial inhibition assay to test for the presence of phenylalanine on a filter paper spot collected from a heel stick. Dr. Guthrie’s invention of the BIA assay was not his only contribution. He was zealous in his mission to ensure that all babies be screened for PKU. His perservence got the attention of Dr. Robert MacCready, the director of the State Laboratory in Massachusetts who attend one of Dr. Guthrie’s training courses. By 1963, the Massachusetts legislature passed a law requiring that all newborns in that state be tested. By 1966, PKU screening was mandatory in the majority of states. Over the years additional disorders were added, such as galactosemia, biotinidase deficiency, hemoglobinopathies and congenital adrenal hyperplasia to name a few.

3
History of NBS 1997 - NC begins piloting MS/MS
NC and MA begin newborn screening with MS/MS WI begins MS/MS NBS Most recently, Tandem Mass Spectroscopy appears to be superceding Dr. Guthrie’s screening test. In 1997, North Carolina collaborating with Neo Gen began piloting the use of tandem mass spectroscopy for newborn screening. In 1999, NC and MA began “in-house” screening with MS/MS and Wisconsin begin piloting the use of tandem mass spectrometry going in 2000.

4
States Screening by MS/MS
Maine Massachusetts Minnesota North Carolina Ohio Wisconsin ** as of September 2001 – Currently a number of states are using tandem mass spectrometry in the newborn screening programs. Some are utilizing the technology to screen for specific disorders, such as Ohio which is currently screening for MCAD and a few of the aminoacidopathies. Others are offering only supplemental screening (meaning testing for diseases not on the state offered panel) as an option for a fee by a number of private and academic laboratories. Other states have either purchased equipment, are considering purchasing equipment or are researching the feasibility of using MS/MS in their states.
 as an option for a fee by a number of private and academic laboratories. Other states have either purchased equipment, are considering purchasing equipment or are researching the feasibility of using MS/MS in their states.")
5
Why Use MS/MS? Small sample size requirement Fast
Screens for many diseases Cost Public awareness and advocacy The question of why are we using tandem mass spectrometry begs to be asked. First and for most tandem mass spectrometry is a powerful tool. It requires a very small sample size to screen for a large number of rare disorders in a very quick amount of time, about 2 minutes. The methodology has a high specificity, sensitivity and less laborious sample preparation time then traditional newborn screening methods for PKU. Cost effectiveness is another important consideration and there are two ways to think about this. First, if you are going to purchase the instrumentation it more cost effective to screen for a number of diseases than just a few of these diseases. This is important to consider in states where the population size is small, making the expensive purchase of tandem mass spectrometry not feasible. Secondly, we must consider the estimated cost of treating individuals with these disorders if diagnosed early versus the cost of treatment if the children do not obtain treatment until damage is incurred. Wisconsin estimated that the cost of detecting and treating the FAOD and OA disorders would be about $400,000 dollars per year, saving approximately $500,000 annually in medical insurance and state programs because of early detection. I also can not emphasis enough how the overwhelming public advocacy for the use of tandem mass spectrometry has influenced many states to begin the implementation process. Organizations such as tyler for life, the organic acidemia association and other support groups have done a marvelous job of education the public and their state legislators about the benefits of newborn screening.

6
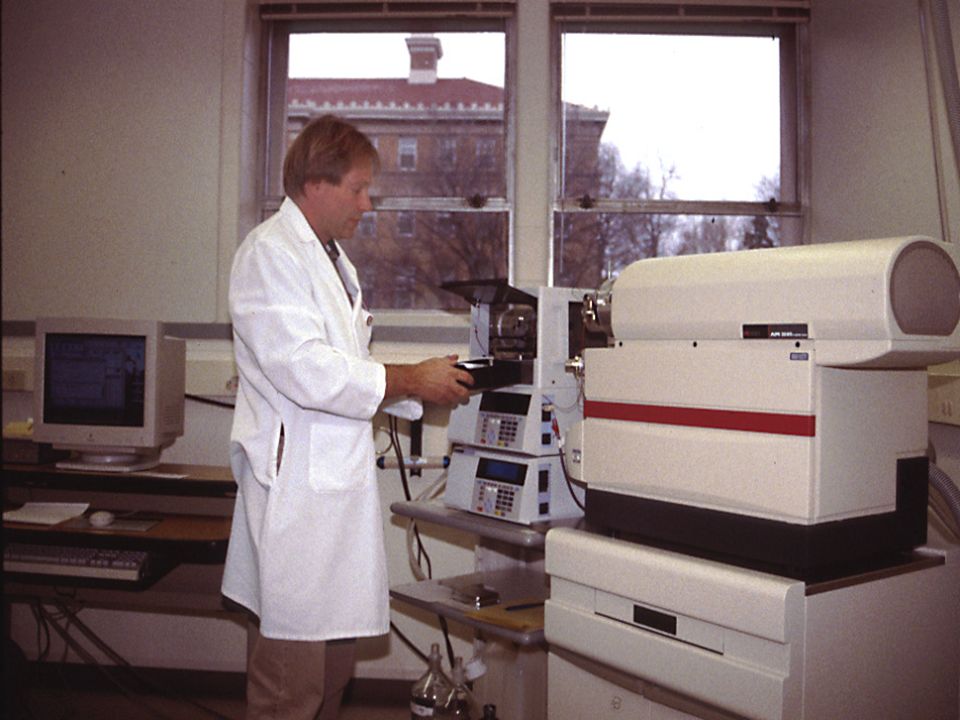
Mass Spectrometry Ion separation and quantification
Produces charged particles Uses electrical and magnetic fields Detection system Mass spectrometer is a devise that separates and quantifies ions based upon their mass/charge ratio. It does this by producing charged particles from the sample being analyzed. It then uses an electrical and magnetic field to separate and measure the mass of the charged particle. Once this is done a detection system produces a spectrograph of peaks which can be quantified using internal standards to determine the amount of each particle present.

7
Sansom, Molecular Medicine Today, March 1999
A tandem mass spectrometer is essentially two mass spectrometers in a series connected by a chamber called the collision cell. This technology has been used for many years to identify and measure carnitine esters in blood and urine of individuals suspected of having a metabolic disorder. Prior to being sent through the first chamber the sample is subjected to soft ionization either by fast atom bomardment or electrospray. This is why you may sometime see FAB-MS/MS or ES-MS/MS. This produces a charged but not fragmented ion for each organic compound (parent ion) in the sample. The first chamber separates these parent ions in order of their mass/charge ratio - sending through the mass charge ratio ion into the collision chamber. The collision cell fragments the parent ions and send these fragments through the second mass spectometer. The fragmentation pattern from each of the parent ions is analyzed and compared to the spectrum of known internal standards and your spectrograph is obtained. The entireprocess from ionization to data relay on the computer takes approximately 2 minutes. Sansom, Molecular Medicine Today, March 1999
 in the sample. The first chamber separates these parent ions in order of their mass/charge ratio - sending through the mass charge ratio ion into the collision chamber. The collision cell fragments the parent ions and send these fragments through the second mass spectometer. The fragmentation pattern from each of the parent ions is analyzed and compared to the spectrum of known internal standards and your spectrograph is obtained. The entireprocess from ionization to data relay on the computer takes approximately 2 minutes. Sansom, Molecular Medicine Today, March")
9
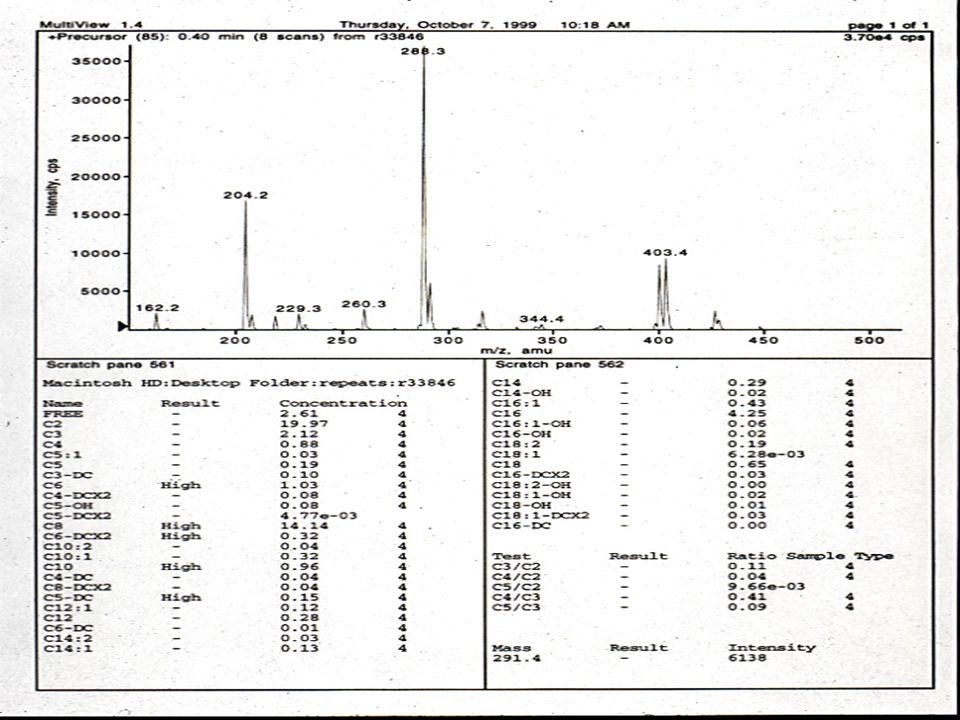
A typical result sheet

11
MS/MS Analysis Aminoacidopathies Organic acidurias
Fatty acid oxidation disorders So, what diseases can we detect if we utilize tandem mass spectrometry in newborn screening programs. These are the three groupings of disorders. Aminoacidopathies are detected using a methodology referred to as a neutral loss assay for specific amino acids in the sample. A full acylcarnitine profile is performed to detect fatty acid oxidation disorders and organic acidurias.

12
Aminoacidopathies Maple Syrup Urine Disease Arginosuccinic Aciduria
Citrullinemia Homocystinuria Maple Syrup Urine Disease Phenylketonuria Tyrosinemia MS/MS technology allows for improvement in and consolidation of methods for detecting amino acid disorders. Thus, along with MSUD, PKU and Homocystinuria, state programs can now test for arginosuccinic aciduria, citrullinemia and tyrosinemia.

13
Organic Acid Disorders
2,4-Dienoyl-CoA Reductase Deficiency 3-Hydroxy-3-Methylglutaryl-CoA Lyase Deficiency 3-Ketothiolase Deficiency MS/MS technology enables the detection of organic acid disorders such as those you see here. Many of these conditions are extremely rare. 2,4-dienoyl-coA reeducates deficiency is an auxiliary enzyme of beta oxidation that has been reported in one individual and to date has not been detected on newborn screening. 3-hydroxy-3-methylglutaryl-CoA lyase deficiency leads to death in childhood if untreated. Symptoms include metabolic acidosis, hypoglycemia, hepatomegaly, fever, sensitivity to dietary leucine and coma. The main symptom of 3-Ketothiolase deficiency (also known as mitochondrial acetoacetyl-CoA thiolase deficiency) is recurrent and severe metabolic acidosis. All three of these disorders are treated with dietary management and carnitine supplementation.
 is recurrent and severe metabolic acidosis. All three of these disorders are treated with dietary management and carnitine supplementation.")
14
Organic Acid Disorders
3-Methylcrotonyl-CoA Carboxylase Deficiency 3-Methylglutaconyl-CoA Hydratase Deficiency Glutaric Acidemia Type I Tandem mass spectrometry also screens for 3-methylcrotynl-CoA Carboxylase deficiency, symptoms of which may include hypotonia, muscle atrophy, seizures, and dermatological changes. Treatment involves dietary restriction and carnitine/biotin supplementation. Fewer than 50 cases of 3-methylglutaconyl-CoA hydratase deficiency have been described but little information about treatment exists. The disease is characterized by motor delays, short attention span, speech delay. GAI is characterized by hypoglycemia, dystonia and metabolic acidosis. Less than 100 cases are known in the US. Dietary restriction has had inconsistent outcomes.

15
Organic Acid Disorders
Isovaleric Acidemia Methylmalonic Acidemia Mulitple CoA Carboxylase Deficiency Propionic Acidemia And of course some old stand-by organic acid disorders. I assume Dr. Korson spoke to you already about many of these conditions, in the interest of time I will not summarize them.

16
Fatty Acid Oxidation Disorders
3-Hydroxy Long Chain Acyl-CoA Dehydrogenase Deficiency (LCHAD) Carnitine Palmitoyl Transferase Deficiency Type II (CPT II) Long Chain Acyl-CoA Dehydrogenase Deficiency (LCAD) Medium Chain Acyl-CoA Dehydrogenase Deficiency (MCAD) Lastly, the utilization of tandem mass spectrometry technology allows for the detection of the fatty acid oxidation disorders. Again, as Dr. Matern will be presenting later today on this topic I am only acknowledging what conditions can be detected via newborn screen on this and the following slide.
 Carnitine Palmitoyl Transferase Deficiency Type II (CPT II) Long Chain Acyl-CoA Dehydrogenase Deficiency (LCAD) Medium Chain Acyl-CoA Dehydrogenase Deficiency (MCAD) Lastly, the utilization of tandem mass spectrometry technology allows for the detection of the fatty acid oxidation disorders. Again, as Dr. Matern will be presenting later today on this topic I am only acknowledging what conditions can be detected via newborn screen on this and the following slide.")
17
Fatty Acid Oxidation Disorders
Multiple Acyl-CoA Dehydrogenase Deficiency (Glutaric Aciduria type II) Short Chain Acyl-CoA Dehydrogenase Deficiency (SCAD) Very Long Chain Acyl-CoA Dehydrogenase Deficiency (VLCAD) It is important for me to point out here, that tandem mass spectrometry can not replace current methods of screening for biotinidase deficiency, hypothyroidism, hemoglobinopathies, congenital adrenal hyperplasia, or galactosemia.
 Short Chain Acyl-CoA Dehydrogenase Deficiency (SCAD) Very Long Chain Acyl-CoA Dehydrogenase Deficiency (VLCAD) It is important for me to point out here, that tandem mass spectrometry can not replace current methods of screening for biotinidase deficiency, hypothyroidism, hemoglobinopathies, congenital adrenal hyperplasia, or galactosemia.")
18
Newborn Screening Criteria
Incidence >1/100,000 Significant morbidity/mortality Successful treatment Reasonable cost Technology OA/FAOD/AA 1/5,000 to 1/10,000 Severe medical complications/death Diet & avoid fasting < $10.00 MS/MS This slide illustrates the diseases in relation to the newborn screening criteria – as we must consider this criteria prior to adding on new disease screening. As you can see here, the combination of these conditions are estimated to affect approximately 1 in 5,000 to 1 in ten thousand livebirths. The conditions can cause severe medical complications or death - FAOD alone are thought to account for 5% of sudden infant death. Treatment in the form of dietary management and avoidance of fasting, is effective at preventing mortality and improving quality of life. The initial cost of performing the analysis by tandem mass spec for these disorders is less than $10.00. Although effective treatments do not exist yet for all of the metabolic disorders identifiable by tandem mass spectrometry,it is thought that some advantage can be achieved for the family and healthcare professionals through early diagnosis. This benefit is clearly seen when even though a child may die in the neonatal period before results are available information is now available for future reproductive use.

19
False Positives Cut-off levels of acylcarnitines may be too low
TPN feedings Prematurity Sampling Error The importance of reducing the false positive rate is obvious, as it leads to unnecessary familial anxiety as well as increased costs in the work-up. Tandem mass spectrometry is estimated to reduce the false positive rate seen with traditional testing methodololgies from about 1.5% to about 0.26%. However, it is important to keep in mind that there are still false positive results. Laboratories providing this service must take a close look at what their established cut-offs are for their acylcarnitine profiles. If these cut-offs are too low, you are obviously going to be generating results that appear elevated, but are in actuality normal. In Wisconsin and other states, we have found that TPN feedings and prematurity have led to elevations of amino acids, specifically for tyrosinemia. Infants who are in severe catabolic state secondary to viral infections or sepsis can also lead to false positive test results. And of course, if samples are taken prior to 24 hours of age the rate of false positive results can increase.

20
False Negatives Cut-off levels of acylcarnitines may be too high
Mild clinical course Sampling Error As with false-positive results the cut-offs determined for laboratory analysis of acylcarnitine profiles has a direct impact on the number of false-negative results. The diseases natural history also impacts the false negative rate with variable conditions not being detected in the newborn period if they have a milder clinical course. And of course, as always sampling error is a concern – insufficient blood spot or taken to early in neonatal life. The diagnostic significance of false positive and he incidence of false negatives can not be determined at this time without more clinical follow-up and continued metabolic surveillance.

21
Positive MS/MS NBS Result
Follow-up Positive MS/MS NBS Result PMD called and faxed results Consultant names provided Medical management recommended F-up by PMD or Genetic Center Follow-up protocols must be in place prior to implementing screening for new disorders and they can be modeled after existing protocols for traditional screening. In Wisconsin, results are called out and faxed to the Primary care physician. The PMD is provided with the name of our two state supported genetic centers and their consultants for guidance regarding follow-up and medical management.

22
Organic Acidemia Follow-Up
Initial Follow-Up Urine organic acids Acylcarnitine profile Plasma carnitine Plasma amino acids Unlike traditional screening for PKU, only a few of the disorders screened for by tandem mass spectrometry have a very specific and diagnosis is simplified. For the majority of the disorders, the elevations may cause more than one metabolic disorder so additional testing must be done to verify the diagnosis. These next few slides illustrate the work-up necessary to confirm a diagnosis following a positive newborn screen result. For organic acid disorders, the first phase of the work-up entails obtaining urine organic acids, a plasma carnitine, plasma amino acids and an acylcarnitine profile from a diagnostic laboratory. To complicate matters, the work-up pursued may vary depending on the clinician performing the evaluation. Cost to family must also be kept in mind.

23
Additional OA Follow-Up
Enzyme analysis in lymphocytes Enzyme analysis in fibroblasts Molecular testing Enzyme analysis in lymphocytes or fibroblasts may also be obtained, as well as molecular testing when available.

24
Fatty Acid Oxidation Follow-Up
Initial work-up Urine organic acids Urine acylglycines Acylcarnitine Profile Plasma carnitine DNA mutations (MCAD and LCHAD)
")
25
Other FAOD Work-Up Fibroblast studies Test siblings
Fatty acid oxidation studies Direct enzyme analysis Western blot Test siblings The use of fibroblasts for oxidation rates of c-1 substrates, tritium release assays using palmitate and myristate, in-vitro probe of fat oxidation pathways, specific enzyme or uptake assays may have to be pursued to better delineate the diagnosis. And I have to point out that the use of skin biopsy is often not well received by parents of a newborn infant, particularly when the child appears perfectly healthy Since many of these disorders appear asymptomatic until a crisis actually occurs, testing of older siblings is recommended. I will discuss two families were testing the older siblings revealed that they were also affected.

26
Aminoacidopathy Follow-Up
Initial work-up Plasma amino acids Other Laboratory Analysis Orotic acid Ammonia Urine organic acids DNA analysis Plasma amino acids to confirm diagnosis. Other labs may need to be performed depending on the condition being considered – such as as orotic acid and ammonia levels for the urea cycle defects or measuring the presence of succinylacetone in urine organic acid for tyrosinemia. DNA testing may also be pursued.

27
Wisconsin Experience Pilot testing began May 1999
Analyzed all specimens received Established instrument reliability Developed reporting policies Developed follow-up protocols Routine testing began April 2000 OA and FAO disorders only The State of Wisconsin purchased a tandem mass spectrometer in Upon completion of internal validation studies the laboratory began a pilot study to test the reliability of the instrumentation under nearly routine conditions, determine abnormal report profiling, establish a reporting mechanism including referral to a biochemical geneticist consultant, and further refine the abnormal acylcarnitine cut-off levels. During the pilot phase, we did not report normal results, we did follow-up on all abnormal results. Results of the first 16,000 samples tested yielded one confirmed case of MCAD, one false positive 3-MCC, and one false negative PA. In April of 2000, routine testing for organic acidurias and fatty acid oxidation disorders began.

28
Wisconsin Experience Organic Acidemia
1 - PA 2 - 3-MBCDD 2 - C3/C2 12 - C3 2 - C5,C5/C3 1 - C5/C2,C5/C3 5 - C5 1 - C3, C5 23 Possible 5 – 3-MCC 2 - MMA 1 - MA 8 - C5OH 5 - C3,C3/C2 18 - C5,C5/C3,C5/C2 1 - C3DC 1 - C5DC 33 Definite Total screened: 85,882. Total of 11 confirmed cases of OA Definite cases are defined as those disorders whose spectrograph is classic for our cutoffs, possible results are borderline abnormal where only a few of the acylcarnitines are abnormal. As you can see we had 8 cases of elevated hydroxy-C5 which is c/w with the profile associated with 3-MCC. Of these 8 cases, we confirmed a total of five cases of 3-methylcrotynl CoA carboxylase deficiency. Elevations of C3 acylcarnitine and C3/C2 ratios lead to the confirmation of one classic methylmalonic acidemia and one benign MMA case. In addition, a borderline result with elevated C3/C2 acylcarnitine ratio was the result of the mild propionic acidemia case that was missed during our pilot period. We also diagnosed two children with 3-methlybutyrl CoA dehydrogenase deficiency which is a condition that was first reported in 2000 – all of the children were of Hmong ancestry and have never been sick.

29
3-MCC Case Study Initial NBS result (6/7/01)
C5OH = 6.45 (>0.6) Referred to state consultant (6/9/01) Patient seen on 6/12/01 F-up laboratory analysis Results obtained (6/15/01) Sibling tested (6/22/01) This child was born on June 5, NBS result revealed an elevation of 3-hydroxy-isovalerylcarnitine c/w 3-methylcrotynl coA carboxylase deficiency. The family was seen for genetic counseling and follow-up labs. Urine acylglycines revealed elevated etylmalonic acid and minimally elevated long-chain dicarboxylic acids. Acylcarnitine profile revealed elevated C5 hydroxyacylcarntine as did the repeat newborn screen. Plasma carnitine revealed low levels of total and free carnitine. The child was placed on carnitine supplementation and we recommended testing his older 2 year old sibling. Testing of his sibling revealed that he too had 3-MCC. Carnitine supplementation was begun. Dietary restriction is currently leucine restriction at the recommended daily allowance.
 Referred to state consultant (6/9/01) Patient seen on 6/12/01. F-up laboratory analysis. Results obtained (6/15/01) Sibling tested (6/22/01) This child was born on June 5, NBS result revealed an elevation of 3-hydroxy-isovalerylcarnitine c/w 3-methylcrotynl coA carboxylase deficiency. The family was seen for genetic counseling and follow-up labs. Urine acylglycines revealed elevated etylmalonic acid and minimally elevated long-chain dicarboxylic acids. Acylcarnitine profile revealed elevated C5 hydroxyacylcarntine as did the repeat newborn screen. Plasma carnitine revealed low levels of total and free carnitine. The child was placed on carnitine supplementation and we recommended testing his older 2 year old sibling. Testing of his sibling revealed that he too had 3-MCC. Carnitine supplementation was begun. Dietary restriction is currently leucine restriction at the recommended daily allowance.")
30
3-MCC NBS Issues Prevalence Diagnosis Severity
Prevalence is much higher than we expected Diagnosis requires skin biopsy because the enzyme is unstable in lymphocytes. In addition we have had several patients with borderline enzyme activities in fibroblasts. Some have also had borderline-low propinyl CoA carboxylases activities.

31
Wisconsin Experience FAOD
1 - SCAD 10 - C4 7 - C10 1 - C6,C8,C10 1 - C14,C14:1, C14:2 2 - C14,C14:1 1 - C10,C16 1 - C16,C18,C16:1,C18:1 24 Possible 4 - SCAD 2 - MCAD 1 - GAII 5 - C4,C4/C2,C4/C3 2 - C6,C8,C10:1,C8/C10 1 - C4,C5,C14,C16 1 - C14,C14:1,C14:2,C16:1 9 Definite Total screened: 85,882. Total of 7 confirmed FAOD cases. Both of our MCAD cases had classic profile, and both are heterozygous for the common mutation and have been asymptomatic. Of the 5 confirmed cases of SCAD – 4 had classic elevations of C4 acylcarntine and abnormal C4/C2 and C4/C3 ratios. One had only an elevated C4 carnitine on a borderline result. Three of the confirmed cases have been hospitalized with episodes of vomiting, diarrhea, dehydration, but normal glucose levels. Unfortunately, the child who had glutaric aciduria type II died before results were obtained, however, with the results available appropriate counseling for recurrence risk was available.

32
SCAD - NBS Issues Prevalence Mild presentation
2 homozygous for G625A polymorphism* *Corydon et al, Ped Res 49 (1):28-23, 2001 Prevalence is much higher than we expected and many of these individuals are asymptomatic. Impaired oxidation of short chain fats, but little to no SCAD activity measured in fibroblasts Research from Corydon and his group suggested that the homozygousity for the G635A mutation (which is estimated to be present in 7% of the general population) may lead to clinical symptoms depending on other genetic, cellular or environmental factors. TREATMENT????
:28-23, Prevalence is much higher than we expected and many of these individuals are asymptomatic. Impaired oxidation of short chain fats, but little to no SCAD activity measured in fibroblasts. Research from Corydon and his group suggested that the homozygousity for the G635A mutation (which is estimated to be present in 7% of the general population) may lead to clinical symptoms depending on other genetic, cellular or environmental factors. TREATMENT")
33
Wisconsin Experience Aminoacidopathies
3 Tyrosinemia – none confirmed 1 Citrullinemia - confirmed I don’t have the total for the number of cases screened before we obtained these four abnormal results. I can tell you that all three cases of tyrosinemia have been found to be false-positives and there has been one confirmed case of citrullinemia.

34
Tyrosinemia Issues Transient tyrosinemia Prematurity False negatives
There appear to be a high rate of false positive results for tyrosinemia. First, transient tyrosinemia is common leading to elevated tyrosine. In addition, premature infants or those receiving hyperalimentation may also have elevated tyrosine levels. Lastly, true tyrosinemia often causes minimal elevation of the tyrosine in newborns so most state laboratories do not have a good data establishing the false-negative rate at this time.

35
Impact of NBS by MS/MS on Families
Anxiety Unknown Limited Resources The most difficult aspect of genetic counseling for positive NBS results by tandem mass spectometry is helping families cope with the anxiety raised by results. This anxiety is very different from dealing with traditional results because of the prolonged waiting time for follow-up lab results which can take up to two weeks. Anxiety can continue long after results have been verified depending on how much information is available regarding the effectiveness of treatment for these conditions. And of course, there is the fear of recurrence risk in future pregnancies or identifying affected siblings. Since many of these disorders have not been diagnosed before in the neonatal time frame or because they are extremely rare, educational resources are scarce. Many of the national support groups are working to fill this void, however, there is still a great gap in the knowledge base regarding the natural history for some of these disorders that make patient literature difficult to generate.

36
Impact of NBS by MS/MS on State Laboratories
Start-up cost/New technology Programming False negatives and false positives Detection of undefined disorders The cost of the tandem mass spectrometer itself is expensive and may be prohibitive for some states. In addition, once a state laboratory decides to obtain the machine laboratory staff must be trained to run the machine and the laboratory must have professionals who are capable of interpreting the data obtained. All of which cost more money. Nonetheless, the cost of the instrument and the training is estimated to lead to a total incremental cost on the order of $10.00 a sample. In Wisconsin, it raised our newborn screening card costs by four dollars. Program administrators need to decide what they are going to test for. The MS/MS can be set up to screen for specific disorders or groups of disorders. For example, if I only want to look for MCAD patients I can program it to only look at C8, C10:1, C8/C10, and C10 levels. Thereby ignoring all other acylcarnitines which may be abnormal. Or I may decide to test only for FAO and OA disorders, but not test for aminoacidopathies. Again, as we just discussed it is important to remember that false positive and false negative results do occur. This makes the follow-up work-up and services in NBS programs critical.

37
Impact of NBS by MS/MS on Genetic Clinics
Increased clinic load Long-term treatment Improved quality of life Natural history Those who have mild disease may never get ill, but need to be followed and treated. Those who avoid neonatal death and survive because of early diagnosis and treatment will also need to be followed, thus increasing the clinic load. This could require the need for more physicians, nutritionists and genetic counselors to provide follow-up and care to affected individuals and their families. Reimbursement for medical foods needed to treat these disorders must also be addressed, as some insurances will not cover the cost of medical foods. As well as the long term costs of treatment for these children. Of course most importantly by treating early we will be decreasing incidence of death and illness from these diseases. We may also gain a better understanding of the natural history of these disorders.

38
Summary Collaboration Close Follow-up Supportive Counseling
MS/MS technology is a powerful tool to detect specific metabolic conditions through newborn screening, however, false negative and positive results do occur. Close coordination between the laboratories performing the screening and the biochemical clinical geneticist and centers is needed to determine screening parameters, adjust cut-off levels to reduce false-positive and false-negative results and to facilitate follow-up. Centers following these children and families need a wide array of clinical services with competent dietitians being critical. In addition, genetic counselors must be prepared to provide the supportive counseling necessary to help families cope with the anxiety raised by positive test results.

39
Acknowledgements WI Newborn Screening Laboratory
Gary Hoffman, PhD Children’s Hospital of Wisconsin William J. Rhead, MD, PhD Waisman Center, UW Jon Wolff, MD, PhD Kristine Hanson, MS, CGC

Similar presentations