Download presentation
Presentation is loading. Please wait.

1
EVALUATION AND MANAGEMENT OF AMENORRHEA Assistant Professor at JUH
Mazen Freij, MBBS MRCOG Assistant Professor at JUH

2
Objectives Know the definition of Amenorrhea and Oligomenorrhea
Understand the endocrine, genetic and anatomical basis for these disorders

3
Definitions Primary amenorrhea
No menses by age 14, absence of 2º sexual characteristics. No menses by age 16 , presence of 2º sexual characteristics.

4
Secondary amenorrhea No menses for 3 months if previous menses were regular. No menses for 6 months if previous menses were irregular

5
Oligomenorrhea Interval of more than 35 days between periods

6
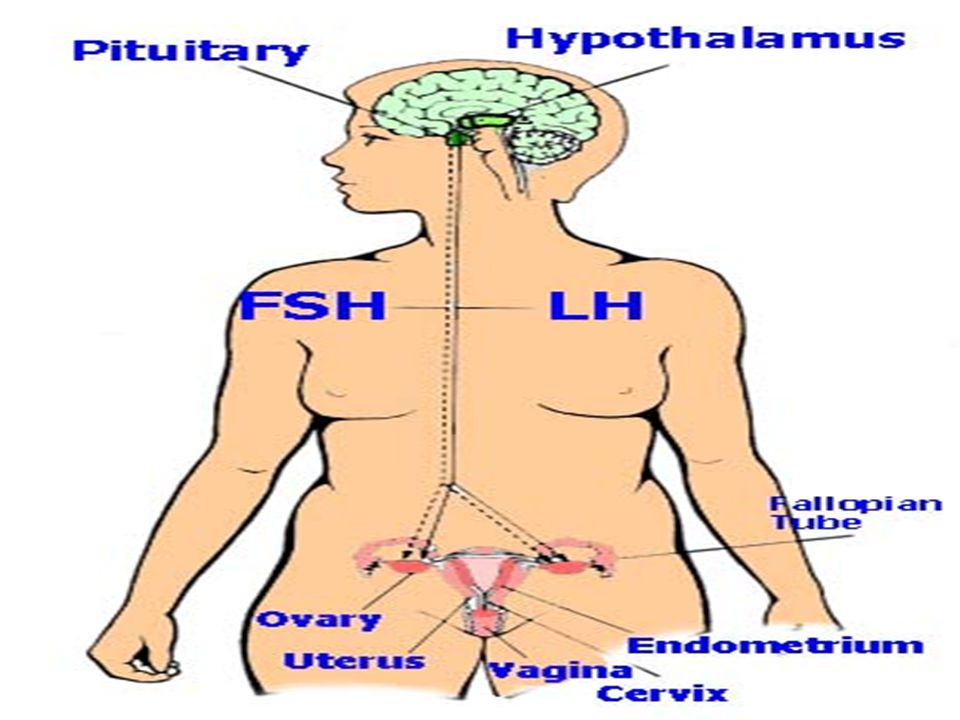
± – ? Menses Neural control Chemical control Dopamine (-)
Norepiniphrine (+) Endorphines (-) Hypothalamus Gn-RH ? – Ant. pituitary FSH, LH Ovaries Estrogen Progesterone Uterus Menses
 Endorphines. (-) Hypothalamus. Gn-RH. – Ant. pituitary. FSH, LH. Ovaries. Estrogen. Progesterone. Uterus. Menses.")
7
AN APPROACH FOR DIAGNOSIS
AMENORRHOEA AN APPROACH FOR DIAGNOSIS HISTORY PHYSICAL EXAMINATION BLOOD TESTS ULTRASOUND EXAMINATION Exclude Pregnancy Exclude Cryptomenorrhea

8
Cryptomenorrhea Outflow obstruction to menstrual blood
- Imperforate hymen - Transverse Vaginal septum with functioning uterus - Isolated Vaginal agenesis with functioning uterus - Isolated Cervical agenesis with functioning uterus

9
Imperforated hymen

10
Amenorrhea and no breast development.
FSH Serum level Low / normal High Hypogonadotropic hypogonadim Gonadal dysgenesis

11
Amenorrhea and normal breast development.
- FSH, LH, Prolactin, TSH Provera 10 mg PO daily x 5 days Prolactin TSH + Bleeding No bleeing - Mild hypothalamic dysfunction - PCO (LH/FSH) Further Work-up (Endocrinologist) Review FSH result And history (next slide)
 Further. Work-up. (Endocrinologist) Review FSH result. And history (next slide)")
12
Amenorrhea Utero-vaginal absence Andogen Insenitivity (TSF syndrome)
Karyotype 46-XY 46-XX Andogen Insenitivity (TSF syndrome) Rokitansky syndrome) Normal breasts & absent sexual hair Normal breasts & sexual hair
 Rokitansky syndrome) Normal breasts. & absent sexual. hair. Normal breasts. & sexual hair.")
13
Amenorrhea PRIMARY AMENORRHEA . Ovarian failure . Hypogonadotrophic
Hypogonadism. . PCOS . Congenital lesions (other than dysgenesis) . Hypopituitarism Hyperprolactinaemia . Weight related SECONDARY AMENORRHEA . Polycystic ovary syndrome . Premature ovarian failure . Weight related amenorrhoea . Hyperprolactinaemia . Exercise related amenorrhoea . Hypopituitarism
 . Hypopituitarism Hyperprolactinaemia. . Weight related. SECONDARY AMENORRHEA. . Polycystic ovary syndrome. . Premature ovarian failure. . Weight related amenorrhoea. . Hyperprolactinaemia. . Exercise related amenorrhoea. . Hypopituitarism.")
14
Gonadal dysgeneis Classic turner’s syndrome (45XO)
- Turner variants (45XO/46XX),(46X-abnormal X) - Mixed gonadal dygenesis (45XO/46XY)
,(46X-abnormal X) - Mixed gonadal dygenesis (45XO/46XY)")
15
Turner’s syndrome • Sexual infantilism and short stature.
• Associated abnormalities, webbed neck,coarctation of the aorta,high-arched pallate, cubitus valgus, broad shield-like chest with wildely spaced nipples, low hairline on the neck, short metacarpal bones and renal anomalies. • High FSH and LH levels. • Bilateral streaked gonads. • Karyotype % 45, X0 - 20% mosaic forms (46XX/45X0) • Treatment: HRT
 • Treatment: HRT.")
16
Turner’s syndrome (Classic 45-XO) Mosaic (46-XX / 45-XO)
 Mosaic (46-XX / 45-XO)")
17
Ovarian dysgenesis

18
Hypogonadotrophic Hypogonadism
Normal hight Normal external and internal genital organs (infantile) Low FSH and LH 30-40% anosmia (kallmann’s syndrome) Treat with HRT
 Low FSH and LH % anosmia (kallmann’s syndrome) Treat with HRT.")
19
Constitutional pubertal delay
• delayed bone age ( X-ray Wrist joint) • Positive family history • Diagnosis by exclusion and follow up
 • Positive family history. • Diagnosis by exclusion and follow up.")
20
Weight-related amenorrhoea Anorexia Nervosa
1o or 2o Amenorrhea is often first sign A body mass index (BMI) <17 kg/m² menstrual irregularity and amenorrhea Hypothalamic suppression Low estradiol risk of osteoporosis Treatment : body wt. (Psychiatrist referral)
 <17 kg/m² menstrual irregularity and amenorrhea. Hypothalamic suppression. Low estradiol risk of osteoporosis. Treatment : body wt. (Psychiatrist referral)")
21
Utero-vaginal Agenisis Mayer-Rokitansky-Kuster-Hauser syndrome
Second most common cause of Primary amenorrhea. Normal breasts and Sexual Hair Normal looking external female genitalia Karyotype 46-XX 15-30% renal abnormalities. Treatment : Vaginal creation (Dilatation VS Vaginoplasty)
")
22
Androgen insensitivity Testicular feminization syndrome
Normal breasts but no sexual hair Normal looking female external genitalia Absent uterus and upper vagina Karyotype 46, XY Male range testosterone level Treatment : gonadectomy after puberty + HRT

23
Amenorrhea Endocrine causes. Genetic causes. Anatomic causes.

25
TEST

26
A. History of leukemia during infancy B. Short stature
A 17-year-old girl presents to the clinic for the evaluation of primary amenorrhea. Which would be an important aspect of her clinical history? A. History of leukemia during infancy B. Short stature C. History of delayed puberty in the family D. All of the above E. None of the above

27
B. Estradiol of 100 pg/ml (normal 40–410)
After receiving Chemotherapy, which of the following labs results would make you consider the diagnosis of ovarian failure? FSH of 60 IU/L (normal 0.33–10.54) B. Estradiol of 100 pg/ml (normal 40–410) C. LH of < 0.2 IU/L (normal 0.69–7.15) D. All of the above E. None of the above
 B. Estradiol of 100 pg/ml (normal 40–410) C. LH of < 0.2 IU/L (normal 0.69–7.15) D. All of the above. E. None of the above.")
28
The commonest cause for primary amenorrhea is
A. Turner Syndrome B. CAH C. Rokitansky Syndrome D. Imperforsted Hymen E. PCOS

29
C. Androgen insensitivity. D. Rokitansky syndrome
One of the following can be the cause for primary amenorrhea with normal secondary sexual development. A. Imperforated hymen. B. Turner Syndrome C. Androgen insensitivity. D. Rokitansky syndrome E. Hypogonadotropic hypogonadism

30
What is the definition of Primary Amenorrhea?

31
19 year old presented with primary amenorrhea, normal breast development but no pubic hair, absent uterus. The most likely diagnosis is: A. Rokitansky syndrome B. Turner Syndrome C. Androgen insensitivity D.Hypogonadotropic Hupogonadism

32
Thank You

Similar presentations





(6)(7)>")






>")






 Professor of OB/GYN Qassim,College of Medicine Amenorrhea Salah Roshdy (MD) Professor of OB/GYN Qassim,College of Medicine.>")