Download presentation
Presentation is loading. Please wait.

1
Nutritional Aspects of ERP
Pete Turner Specialist Nutritional Support Dietitian

2
Programme ERP philosophy NBM Preoperative Carbohydrate Loading
Malnutrition and surgery Screening - MUST Treatment plan

3
Enhanced Recovery Programme (ERP)
Multifactorial approach to optimise recovery from surgery and reduce length of stay Optimal anaesthesia and analgesia Appropriate fluid management Early postoperative mobilisation Nutritional Aspects Good evidence in colorectal surgery – growing evidence in other surgery

4
Nutritional Aspects of ERP
Avoidance of nil by mouth (NBM) Appropriate fluids Preoperative carbohydrate loading Early postoperative nutrition ERP should include… Screening for risk of malnutrition Preoperative nutritional support for those at risk
 Appropriate fluids. Preoperative carbohydrate loading. Early postoperative nutrition. ERP should include… Screening for risk of malnutrition. Preoperative nutritional support for those at risk.")
5
Avoiding Preoperative NBM
ESPEN – Grade A evidence (Clinical Nutrition(25) 2006) Avoids dehydration Require less iv fluids Avoid sodium overload Quicker recovery GIFTASUP ESA 2011
 2006) Avoids dehydration. Require less iv fluids. Avoid sodium overload. Quicker recovery. GIFTASUP. ESA")
6
Sodium Basal Sodium Requirements? 1mmol/kg/day
How much Na in 1000mls saline? 150mmol How much Na in 1000mls Hartmann’s? 131mmol Oedema GIFTASUP (

7
Sodium Excess sodium Oedema Bowel oedema Delayed bowel function
Ileus (Lobo et al 2002, Lancet 25;359, ) Guidelines on Intravenous Fluid Therapy in Adult Surgical Patients – GIFTASUP (
 Guidelines on Intravenous Fluid Therapy in Adult Surgical Patients – GIFTASUP (")
8
Preoperative Carbohydrate (CHO)
Beneficial to anyone undergoing major surgery Traditional preoperative fast harmful 12 – 16 hours NBM Metabolism changes to “starved” state

9
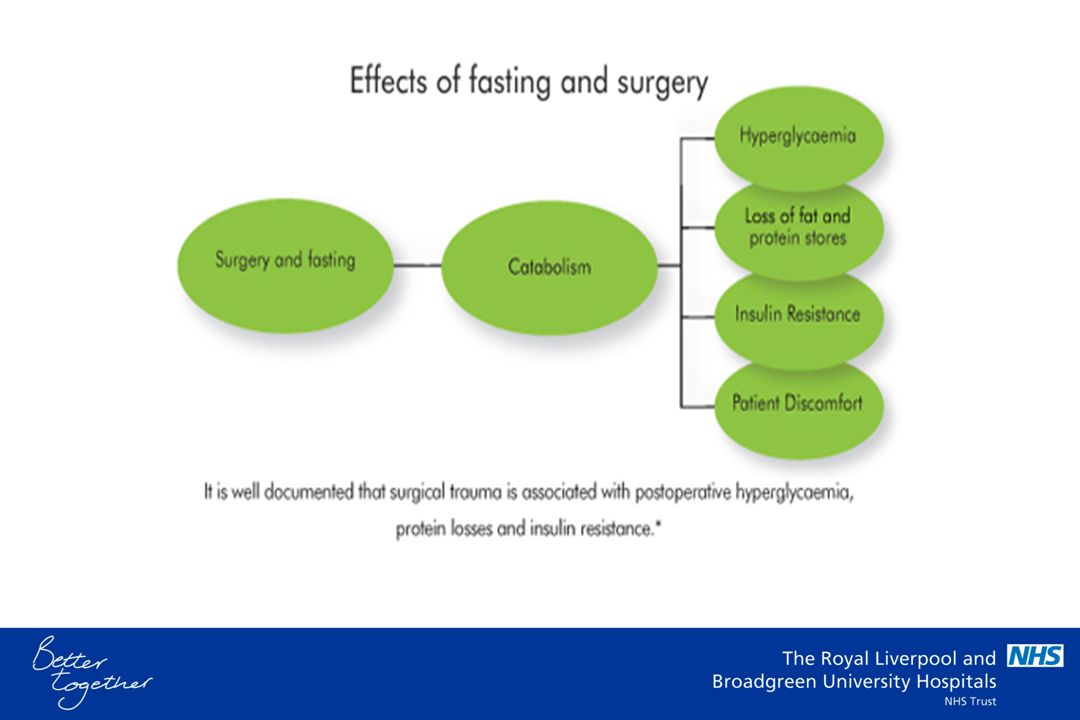
Starved State 12 hrs – 20 days Increased Glucagon Increased Cortisol
Catabolism Gluconeogenesis Insulin resistance

10
Surgery Inflammatory response Increased cortisol, cytokines
Catabolism, gluconeogenesis Insulin resistance Hyperglycaemia Exacerbated by starvation

12
CHO loading 50g glucose polymer 2 servings night before surgery
1 Serving 2 hours before surgery Block metabolic changes to starvation Safe (ESPEN 2006 Grade A) PreLoad – Vitaflo PreOp - Nutricia
 PreLoad – Vitaflo. PreOp - Nutricia.")
13
CHO loading Decreased catabolism Decreased hyperglycaemia
Preserved muscle mass Improved grip strength Reduced LOS Reduced Anxiety

14
LOS Study meta-analysis
Ljungqvist et al 1998 Clin Nutr 17, Suppl1:3. Meta-analysis of 3 RCTs Preoperative CHO vs overnight fast 20% reduction in LOS Preop CHO beneficial to all patients undergoing major surgery (ESPEN Grade B)
")
15
Not Just Colorectal Urology Pancreatic Hip replacement
Knee replacement

16
All elective surgery

17
Contraindications? Diabetes?
Safe in type II in hospital (Gustafsson et al 2008, Acta Anaesthesiol Scand 52(7), ) Alcoholics – Wernicke Korsakoff syndrome? Severely malnourished Refeeding syndrome? Emergency surgery?
, ) Alcoholics – Wernicke Korsakoff syndrome Severely malnourished. Refeeding syndrome Emergency surgery")
18
Post Operative - ACRU Ensure Plus Nutritionally balanced
Used 4 hrs post op on ACRU Well tolerated Stop day 4 in well nourished Continue in malnourished

19
Balanced oral nutritional supplements
Fortisip Fresubin Ensure Plus Milkshake Clinutren NICE CG32 Grade A

20
Early Post Operative Nutrition
NICE CG32 Promote gut function Attenuate stress response Prevent bacterial translocation Immune function - GALT Reduced anastamotic dehiscence NICE – Grade A evidence in malnutrition

21
Malnutrition 1 in 5 malnourished (Edington 2000) Increased LOS
More infections More antibiotics BAPEN NSW 2007 – RLBUHT

22
Cost of Malnutrition Annual cost of obesity to NHS?
£4.2 billion (DOH 2011) Annual cost of malnutrition to NHS? £13 billion (BAPEN 2009)
 Annual cost of malnutrition to NHS £13 billion (BAPEN 2009)")
23
Malnutrition and Surgery
NICE 2006 CG 32 3 times as many post operative complications 4 times greater risk of death at surgery Increased infection Poor wound healing Depression Hip fracture – BMI <18.9 increased mortality

24
Enhanced Recovery & Malnutrition
Does ER include preoperative treatment of malnutrition? ESPEN 2006 – Grade A BAPEN Council Mike Stroud – NICE Professor Marinos Elia – Govt policy – Malnutrition Matters

25
What can we do? Screen at Preop & OPD – NICE CG 32
Malnutrition Universal Screening Tool (MUST) OSCAR Management guidelines Dietetic referral Preoperative sip feeds Southampton – Mike Stroud
 OSCAR. Management guidelines. Dietetic referral. Preoperative sip feeds. Southampton – Mike Stroud.")
26
MUST Malnutrition Universal Screening Tool BAPEN
Identifies Malnourished At risk of Malnutrition Validated NICE CG 32 NHS litigation agency

28
MUST Management Plan MUST Score 0 – Low risk. Routine Care
1 – Medium risk. High protein diet sheet 2 – High Risk. High protein diet sheet Dietitian Oral Nutritional Supplements

30
How long? ESPEN 10 -14 days (Grade A) NICE CG 32
“Most trials showing benefit from short-term nutrition support, do so despite ‘too little nutrition’ being given for ‘too short a time’ for the benefit to accrue from maintaining or improving body energy and protein stores”

31
Artificial Nutrition

32
Portable Pumps

33
TPN

34
Conclusions Preoperative starvation is harmful
Preoperative CHO loading is beneficial Most major surgery Safe in elective surgery

35
Conclusions High incidence of malnutrition
Greatly increases risk of surgery Morbidity and mortality Preoperative treatment effective ESPEN, NICE CG32 European & UK experts – include in ER Evidence –

Similar presentations












. 2 Hyperglycaemia Learning objectives >Can state what hyperglycaemia is >Is aware of the short term and.>")







