Download presentation
Presentation is loading. Please wait.

1
DIAGNOSIS, EVALUATION AND THERAPY PLANNING FOR VELOPHARYNGEAL INSUFFICIENCY
Virginia Dixon-Wood, MA CCC-SLP University of Florida Craniofacial Center UF Speech and Hearing Clinic

2
Common Misconceptions
Any speech pathologist can treat children with VPI Hypernasality is the major speech problem Speech therapy won’t help until surgery is done VPI is a voice disorder Refer to ENT or neurologist

3
Insufficiency vs. Incompetency
Structurally based -cleft palate, submucous cleft Motor based - stroke, cerebral palsy, low tone, TBI Mix- VCFS (22q-)
")
4
PRE-NATAL COUNSELING Cleft lip only
Potential for cleft palate based on severity (width) of cleft lip Up to 50% of families now know prenatally In the long run, families do much better
 of cleft lip. Up to 50% of families now know prenatally. In the long run, families do much better.")
5
Birth to 6 months Feeding instruction and counseling
Speech and Language development Hearing related issues

6
SPEECH COUNSELING Many children may never need speech therapy
Palate closure at 8-12 mo. Six month speech evaluations Parent counseling

7
6 months- 1 year REEL Scale 2
Receptive-Expressive Emergent Language Scale – Bzoch Birth to 3 years

8
6 months – 1 year Discuss surgery (9-12 months) Parents expectations
Surgery counseling

9
12 mo. - 2 years Begin phonological inventory range of sounds
oral/nasal contrast REEL Scale – refer for EI Parent counseling

10
Stages of Speech Development
Vocalizations - birth Babbling - C+V repetition, 3 mo. Jargon - mixed C+V, 8 mo. First “true word” mo. Two word combinations - 18 mo.

11
Early Speech Development
Cleft m, n g y, h, w Non- cleft m, n d, b, p, g y, w

12
Speech Characteristics of the Young Child with Possible VPI
Delayed expressive language development Very limited phonologic inventory - m,n,h,y and some vowels Use of speech template Consistent nasal substitutions

13
Early Speech Development
Sound differentiation Nasal vs. Oral bye-bye vs. mye mye bye-bye vs. i i bye-bye vs. ? ?

14
Preschool Can assess palatal function
Informally – predominately nasals and vowels vs. combination of nasal and pressure sounds Stimuli – baby, puppy, bye bye Formally – Measures of nasal emission and articulation testing

15
Speech Characteristics of VPI
Glottal compensations Nasal substitutions Inappropriate nasal air emission Weak pressure consonants Hypernasality

16
Preschool Evaluation of VPI: Sound Production Audible nasal emission
Glottal Compensations

17
Perceptual testing Nasal emission Articulation Resonance
Intelligibility

18
Communicative Disorders Test Kenneth R.Bzoch
Designed for specific speech characteristics of cleft palate clients Articulation Resonance Nasal emission Voice - hoarseness, aspirate voice quality

19
Audible nasal air emission
Inappropriate air leakage through the nose during the production of consonants Tested on high pressure sounds - plosives or continuants /p,b,s/

20
Nasal Air Emission Tests inappropriate nasal air escape during the production of high pressure consonants /p,b/ Use visual or auditory feedback - p-paddle, mirror, listening tube Base 10 index Document change

23
Resonance Relationship between size of oral and nasal resonating cavities Normal resonance – balanced VPI creates a increased nasal resonating cavity Cold/allergies create a decreased nasal resonating cavity

24
Resonance Perceived during vowel production Cul-de-sac testing
Listener perception

25
Hypernasality Abnormal amount of nasal resonance
Negative impact on listener Perceived during vowel production Tested on vowels with oral consonants beet, bit, bait, bought, boat

26
Hyponasality Too little nasal resonance
Not perceived as negatively by listener Common cold, allergies, sinusitis, enlarged tonsils and adenoids, pharyngeal flap Cul-de-sac testing Nasometry

27
Hypernasality Vowels with /b/
If resonance is normal (oral)- there should be no difference between the 2 productions Base 10 index Document change
- there should be no difference between the 2 productions. Base 10 index. Document change.")
29
Hyponasality Vowels with /m/
If normal resonance, there should be a difference (shift) between words Base 10 Document change
 between words. Base 10. Document change.")
30
Significance Indexes of 3/10 or greater
Do indexes match what you are hearing in conversational speech? Impact on the child and/or family?

31
Voice Vowel prolongation- timed
Aspirate -may be compensation to conceal hypernasality Hoarseness - may be caused by glottal compensations

32
Error Pattern Diagnostic Articulation Test
Developed for patients with cleft lip/palate Based on manner of production Classifies many different errors - correct, NE, distortion, simple/glottal substitution, omission Error and articulation scores Documents change

33
Speech Sample Spontaneous single words Conversation Estimate a %
Does it validate your other test results?

34
Palatal Fistulae Opening along the suture line Assess size (mm)
Document location Can be responsible for abnormal articulation patterns Nasal emission

35
Fistula Important part of oral exam
Anterior fistulae - impact on articulation Nasal emission - may be inconsistent or phoneme specific Resonance - may be normal

36
Fistula Recommendations based on speech results: surgical closure
obturate do nothing

37
NOW WHAT ?

39
Creating the Treatment Plan
Age Articulation vs. resonance Severity of articulation disorder What is interfering the most with intelligibility Child and family reaction What can you treat?

40
SPEECH THERAPY WHAT? WHY? WHEN? HOW?

42
Treatment Plan You have to understand the problem before you can create a treatment plan Not understanding the problem can create additional articulatory compensations Can waste valuable time and money

43
Treatment Plan Nasalized – diagnostic therapy to see if child can impound oral pressure (short term) Glottal compensations – help the child learn to create oral breath pressure

44
What NOT to do Muscle Training: (Cole, 1979) Indirect Semidirect
 Indirect Semidirect")
45
What NOT to do Yules, 1968 Subjects were able to reduce nasal emission on short tests but that establishment of performance in automatic speech remained to be demonstrated

46
What NOT to do McWilliams-no evidence that muscle training had any impact on improving speech or reducing nasal emission

47
Misarticulations Judy Trost-Cardamone, 1997
Obligatory errors - physical management hypernasality, nasal emission, weak pressure consonants Passive/Learned Errors - compensatory errors, phoneme specific

48
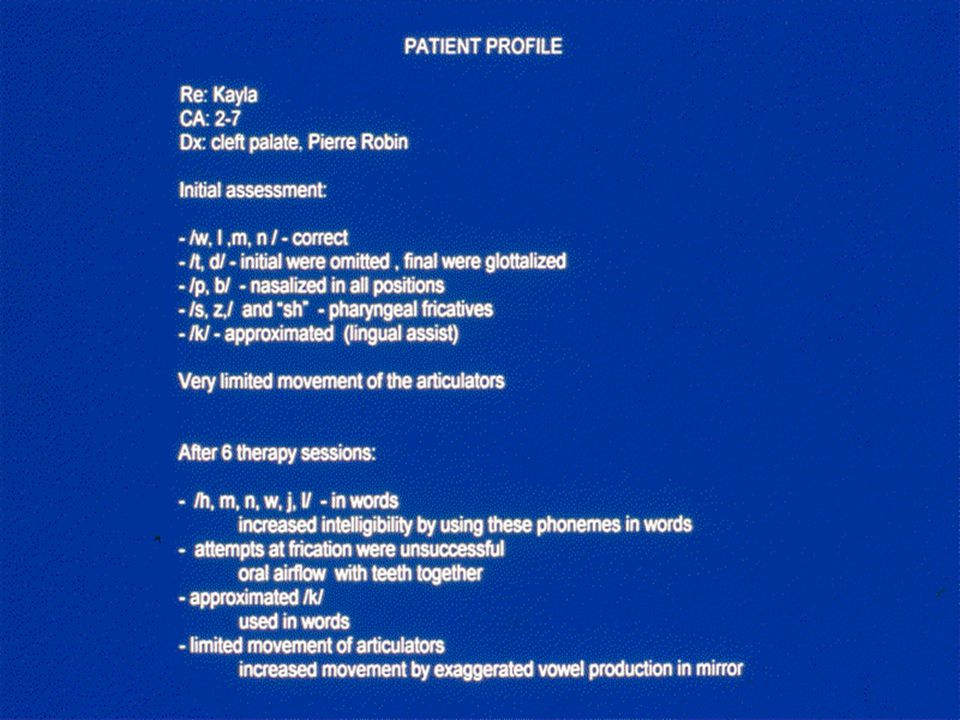
Treatment Planning Child 1 Increase movement of articulators Vowels
Increase intelligibility /m,n,y,h,w,l/ Frication Pressure sounds

49
Treatment Planning Child 2 Develop oral air flow Vowels
Increase intelligibility /m,n,y,h,w,l/ Frication Pressure phonemes

50
Speech Therapy Delayed speech development in young children but without glottal compensations Nasal emission distortion/unintelligible speech Poor articulatory movement

51
Speech Therapy Goal: Improve articulation/intelligibility
Hypernasality and nasal emission are not priorities Improve movement of articulators Accurate vowel production Low pressure consonants

52
Speech Therapy Delayed speech development with glottal compensation
Improve intelligibility Establish oral airflow - this is imperative Can create “popping” or “clicking” for pressure sounds

53
Speech Therapy Child with glottal compensations:
Improve articulatory movements Accurate vowels Low pressure consonants - oral airflow Frication Plosives

54
Speech Therapy Glottal compensations Sonorants Unvoiced Final position

55
Speech Therapy Glottal compensations- Begin with ANTERIOR sounds

56
Speech Therapy Multisensory
Not successful at duplicating what they have heard Visual Tactile Kinesthetic

57
Speech Therapy Glottal Articulation TEACHING PLACEMENT IS NOT ENOUGH
CAN CREATE CO-ARTICULATIONS

58
Palatal Fistula vs. VPI Obturate fistula Speech therapy - 3-6 months
Objective testing

59
VIDEOFLUOROSCOPY Poor candidates: compensatory articulation
poor articulation skills significant palatal fistula very young or uncooperative child

60
Impact of Articulation on Velar Function
Glottal articulation can “shut down” palatal movement Often there is little movement of the articulators as well Palatal fistulae can also impact velar function

Similar presentations















 Mechanism Delivery of Service Linda D. Vallino-Napoli, PhD, MS, CCC-SLP/A.>")



: Definition: Faulty articulation of one or more of speech sounds.>")









