Download presentation
Presentation is loading. Please wait.

1
Lifestyle Interventions for the Management of Hypertension
Louise Beesley Hypertension Nurse Specialist

2
Lifestyle Interventions for the Management of Hypertension
Review current guidelines Review evidence base for key lifestyle interventions Explore less common lifestyle interventions

3
So what do the guidelines say?

4
BHS Guidelines for the management of hypertension
BHS IV, 2004 and Update of the NICE Hypertension Guideline, 2006 Guidelines for management of hypertension: report of the fourth Working Party of the British Hypertension Society, 2004 BHS IV B Williams et al: J Hum Hyp (2004); 18:
; 18:")
5
A population strategy is required to
- prevent the rise in blood pressure with age - reduce the need for antihypertensive drug therapy - reduce the CVD burden Remember primary prevention BHS IV

6
Lifestyle intervention may -decrease pharmacological intervention
Effective lifestyle modification may decrease BP as much as a single antihypertensive, combinations achieve more Lifestyle intervention may -decrease pharmacological intervention -enhance antihypertensive effect of drugs -reduce need for multiple drug treatment -positive influence on overall CVD risk BHS IV

8
Limitation of alcohol consumption Increased physical activity
Lifestyle measures that lower blood pressure Weight reduction Limitation of alcohol consumption Increased physical activity Increased fruit and vegetable consumption Reduced total fat and saturated fat intake Measures to reduce cardiovascular disease risk Cessation of smoking Replacement of saturated fats with mono-unsaturated fats Increased oily fish intake BHS IV

9
Encourage use of salt substitutes
Discourage excessive consumption of coffee and other caffeine rich products Tell patients about local initiatives that provide support and promote lifestyle change Consider relaxation therapies Lifestyle advice should be offered initially and then periodically to patients undergoing assessment or treatment for hypertension Offer guidance and written or audiovisual information NICE 2006

10
Impact of lifestyle interventions on blood pressure
2-4mmHg Alcohol 4-9mmHg Exercise 2-8 mmHg Salt 8-14 mmHg Dietary 5-10 mmHg per 10kg weight loss Weight reduction Expected systolic blood pressure reduction Intervention BHS IV

11
Lifestyle Interventions

12
The effect of weight loss on BP
Estimated 24% of the population in the UK have a BMI > 30 Neter et al (2003): 1mmHg reduction in BP per 1kg weight loss Weight reduction has beneficial effects on associated risk factors i.e. insulin resistance, diabetes, dyslipidaemia and LVH
: 1mmHg reduction in BP per 1kg weight loss. Weight reduction has beneficial effects on associated risk factors i.e. insulin resistance, diabetes, dyslipidaemia and LVH.")
13
Clinic measurements Weight Height BMI
Waist measurement – midway between lower rib margin and the ileac crest

14
BMI and Waist measurements
BMI Category < Underweight Normal Overweight Obese > Severely Obese Abdominal obesity Men >102cm Women >88cm Indio Asia decent Men >90cm Women >80cm JBS Guidelines 2005

15
Referral pathway Exercise on prescription Dietician “Weight Watchers”
Obesity clinic Surgical Intervention

16
Long term benefits of weight reduction
He et al. (2000) “Beneficial effects are still evident 7 years after study ended.” n= 208 high impact weight reduction advice and support 7 years later 181 brought back Incidence of hypertension: 19% in weight loss group 40% control group Effect, despite being an equal amount of weight gain in both groups over the period
 Beneficial effects are still evident 7 years after study ended. n= 208 high impact weight reduction advice and support. 7 years later 181 brought back. Incidence of hypertension: 19% in weight loss group. 40% control group. Effect, despite being an equal amount of weight gain in both groups over the period.")
17
Dietary interventions and BP
DASH – Dietary approach to stop hypertension diet (2000) Participants with mild hypertension had approx. 11.4mmHg reduction in systolic BP compared to control diet Combination of a Mediterranean diet with low fat dairy products Low fat, high fibre including increased amounts of potassium, calcium, and magnesium Effects potentiated by salt restriction Diet better tolerated than salt restrictions
 Participants with mild hypertension had approx. 11.4mmHg reduction in systolic BP compared to control diet. Combination of a Mediterranean diet with low fat dairy products. Low fat, high fibre including increased amounts of potassium, calcium, and magnesium. Effects potentiated by salt restriction. Diet better tolerated than salt restrictions.")
18
5 a day (or 7-9 if possible!)
1 portion of fruit or vegetable represents 80g i.e 1 apple, 1 orange, 1 banana, 2 satsumas, 2 plums, 3 heaped tbsp peas or carrots, 1 bowl of mixed salad 1 glass of 100% fruit juice can replace 1 portion 1 portion of fruit and vegetables a day lowers CVD risk by 4% (Joshipura et al. 2001) Beneficial effects due to array of compound i.e. vitamins and minerals, phytochemicals, antioxidants Individual compounds not enough – supplements containing isolated compound do not have same effect – may cause more harm than good
 Beneficial effects due to array of compound i.e. vitamins and minerals, phytochemicals, antioxidants. Individual compounds not enough – supplements containing isolated compound do not have same effect – may cause more harm than good.")
19
Physical activity and BP
Aerobic endurance based activities reduce resting BP in adults with normal BP and in those with hypertension Places demands on the cardiovascular system Reductions in BP last for up to 22hrs after exercise (ACSM, 2004) BP reductions are independent of weight loss (Whelton et al. 2002)
 BP reductions are independent of weight loss (Whelton et al. 2002)")
20
Exercise training in the management of and treatment of hypertension
2.4 4.6 6,805 105 Dickenson et al. 2006 3.0 3,936 72 Cornelissen and Fagard 2005 2.5 4.0 2,419 54 Whelton et al. 2002 3.4 2,674 44 Fagard 2001 3.1 4.7 1,553 29 Halbert et al Decrease in DBP (mmHg) in SBP Number of subjects RCTs included Meta-analysis Adapted from EUROACTION data BJC Sept 2006
 in SBP. Number of subjects. RCTs included. Meta-analysis. Adapted from EUROACTION data BJC Sept")
21
Exercise Recommendations
Frequency –x5, preferably all days of the week Intensity – moderate Time – 30 minutes or more of continuous activity, alternatively 3 bouts of no less than 10 minutes accumulated during the day Type – aerobic exercise using large muscle groups Caution if systolic >160mmHg and/or diastolic >110mmHg

22
Alcohol and BP Association seen as long ago as 1917
Study of trench soldiers “tres grands buveurs” – hypertensive “sobres” – normotensive Klatsky (1977) n= 84,000 men 3 or more drinks per day – dose dependent relationship Beevers (1984) direct pressor effect of alcohol established –observed alcohol consumption and withdrawal
 n= 84,000 men. 3 or more drinks per day – dose dependent relationship. Beevers (1984) direct pressor effect of alcohol established –observed alcohol consumption and withdrawal.")
23
Reduction in alcohol consumption may reduce
BP by an average of 3/2 mmHg (Xin 2001) Daily drinking and on empty stomach associated with higher BP There should be 2 alcohol free days per week There are probably no safe alcohol limits ≤ 14 units per week for women and ≤ 21units per week for men Binge drinking is now defined as >3 units/day ?? Cardioprotective properties……Jackson argued may be due to confounding
 Daily drinking and on empty stomach associated. with higher BP. There should be 2 alcohol free days per week. There are probably no safe alcohol limits. ≤ 14 units per week for women and ≤ 21units per week for men. Binge drinking is now defined as >3 units/day. Cardioprotective properties……Jackson 2005 argued may be due to confounding.")
24
Assess number of units per week
Number of alcohol free days Binge drinking GGT 125ml wine 1 pub shot of spirit (35ml) ½ pint lager / beer / cider
 ½ pint lager / beer / cider.")
25
Wine strength 11.1 10.5 9.6 9.0 8.4 7.5 6.9 750ml bottle 3.7 3.5 3.2 3.0 2.8 2.5 2.3 250ml 2.6 2.1 1.9 1.8 1.6 175ml 1.7 1.5 1.4 1.3 1.1 125ml 15% 14% 13% 12% 11% 10% 9% Glass size The Times Dec 2006

26
Smoking and BP Cigarette smoking does not appear to be associated with hypertension BP does rise acutely during smoking leading to underestimation of BP in regular smokers Extensive observational data show that smoking has a graded adverse effect on risk of cardiovascular complications Use of nicotine replacement therapies is safe in hypertensives and doubles smoking cessation rates

27
Assess smoking history
- smoker / non smoker - how long given up - number of years / pack years - method of smoking - previous attempts at cessation - NRT - desire to give up Smoking cessation clinic / NRT

28
Effect on CVD risk Age 51 Gender male SBP 156 Smoker no Hx diabetes no
LVH no Cholesterol 5.1 HDL 1.2 CVD RISK % Age 51 Gender male SBP 156 Smoker yes Hx diabetes no LVH no Cholesterol 5.1 HDL 1.2 CVD RISK %

30
Effect of Salt on Blood pressure
Recommended salt intake is 5g/day Estimated that average intake is 9.5g/day A max of 25% comes from adding at table or cooking Na value x 2.5 to gain NaCl value DASH Sodium - reduction in blood pressure with lower sodium intake – direct relationship Few observational studies and virtually no trial data exist on the effect of sodium intake on subsequent cardiovascular disease

31
Sacks et al. N Eng J of Med 2001;344:3-10

33
TOHP I and II, adjusted for age, sex, and clinic
Fig 2 Cumulative incidence of cardiovascular disease (CVD) by sodium intervention group in TOHP I and II, adjusted for age, sex, and clinic Cook, N. R et al. BMJ 2007;334:885 Copyright ©2007 BMJ Publishing Group Ltd.
 by sodium intervention. group in. TOHP I and II, adjusted for age, sex, and clinic. Cook, N. R et al. BMJ 2007;334:885. Copyright ©2007 BMJ Publishing Group Ltd.")
34
Fig 3 Total mortality by sodium intervention group in TOHP I and II, adjusted for age,
sex, and clinic Cook, N. R et al. BMJ 2007;334:885 Copyright ©2007 BMJ Publishing Group Ltd.

35
< 5 grams?!!! 1g 0.5g 0.8g 2g 3.5g TOTAL 9.3g Breakfast
30g cornflakes with skimmed milk and red berries 1 Slice brown bread with low fat spread Lunch 1 tortilla wrap 2 slices “carvery ham” 1 packet popular brand crisps Apple Evening meal Healthy options lasagne, side salad, jacket potato Yoghurt and strawberries Snack 2 digestive biscuits, banana 1g 0.5g 0.8g 2g 3.5g TOTAL 9.3g

36
Salt Friendly??? <0.25g salt per 100g of food - low
Fresh fruit, vegetables Pulses, lentils Meat, chicken Unsalted nuts Rice Pasta Egg noodles Chicken Egg <0.25g salt per 100g of food - low 0.25 – 1.25g salt per 100g of food moderate >1.25g salt per 100g food heavily salted High Canned produce Processed meats Ready meals Packet food Bread Some cereals Cheese Bottle sauces i.e. ketchup,soy Bacon/ sausage/ beefburgers Pates/ smoked or tinned fish

37
Salt substitutes Losalt 131mg of Sodium 346mg of Potassium
1 gram contains: 131mg of Sodium 346mg of Potassium 800mg of Potassium in the average daily diet from salt substitute. Combined multisource daily intake is approx 3000mg potassium Guidance on high Potassium intake: daily range: 1600mg to 5900mg harmful range: 17,600mg (50g of LoSalt)
")
38
Effects of other minerals
Potassium: ↓ BP 4.4/2.5 mmHg in hypertensive patients ↓ BP 1.8/1.0 mmHg in normotensives Observational studies show links to calcium and magnesium Less consistent evidence supporting omega -3 fatty acids, vits C, E and B6, folate and flavenoids. NICE/BHS ‘do not give supplements’

39
Caffeine rich products and BP
Potent physiological effects Caffeine given as tablets resulted in BP elevations ( x4 greater than for caffeinated coffee) Noordzij et al. 2004 Winkelmayer et al. (2005) found association with caffeinated cola drinks and risk of hypertension (but not with caffeinated coffee) Caffeine intake may only be a risk factor in individuals who are genetically slow caffeine metabolisers (Cornelis,2005)
 Noordzij et al Winkelmayer et al. (2005) found association with caffeinated cola drinks and risk of hypertension (but not with caffeinated coffee) Caffeine intake may only be a risk factor in individuals who are genetically slow caffeine metabolisers (Cornelis,2005)")
40
Hamer,M (2006) Journal of human hypertension.20, 909-912
Coffee Effect on health remains equivocal 2 prospective cohort studies give conflicting opinions - Winkelmayer et al showed no relationship between coffee intake and incidence of hypertension (n=155,594 US women over 12 years) - Klag et al – John Hopkins precursor study demonstrated a 0.19 and 0.29 mmHg rise in systolic and diastolic respectively (n=1017 men consuming 1 cup of coffee per day Hamer,M (2006) Journal of human hypertension.20,
 - Klag et al – John Hopkins precursor study. demonstrated a 0.19 and 0.29 mmHg rise in systolic and diastolic respectively (n=1017 men consuming 1 cup of coffee per day. Hamer,M (2006) Journal of human hypertension.20,")
41
Hamer,M (2006) Journal of human hypertension. 20, 909-912.
?? Beneficial effects ? Anti-oxidant properties ? Anti-inflammatory effects ? Inhibit harmful effects of other dietary components i.e. inhibition of alcohol- related hypertensive effects by lowering serum GGT Hamer,M (2006) Journal of human hypertension. 20,
 Journal of human hypertension. 20,")
42
Dietary peptides and BP
Certain dietary peptides shown to lower BP Peptides are now being incorporated into food products Derived from the milk product casein either through fermentation or enzymatic hydrolysis IPP (transpeptides isoleucine proline-proline) and VPP (valine proline- proline) inhibit angiotensin converting enzyme Dose dependent response in reduction of both systolic and diastolic BP
 and VPP (valine proline- proline) inhibit angiotensin converting enzyme. Dose dependent response in reduction of both systolic and diastolic BP.")
43
Stress management Often quoted as cause of hypertension – no evidence to support this Stress and anxiety cause a temporary rise in BP, but when relaxed will fall to normal levels

44
Relaxation Therapies Stress management Meditation Cognitive therapies
Muscle relaxation Biofeedback Shown to result in short term reductions in BP, but the interventions studied have been so varied, it is difficult to be prescriptive

45
Changes (start-end) in systolic blood pressure for stress management interventions
Bandolier Oct 2002

46
Resperate “relaxes constricted blood vessels to lower BP”
15mins paced breathing few times per week leads to vasodilation of vascular smooth muscle

47
Herbal remedies Limited and inadequate evidence available to support the use of garlic, herbal and complimentary medicines to lower BP - potassium supplement - dandelion leaf (diuretic) - hawthorn (vasodilator) - linden (vasospasm) - ginkgo biloba (peripheral blood flow) - mistletoe (vasodilator) - ginger (Mg2+,Ca2+,K+)
 - hawthorn (vasodilator) - linden (vasospasm) - ginkgo biloba (peripheral blood flow) - mistletoe (vasodilator) - ginger (Mg2+,Ca2+,K+)")
48
Motivation, Motivation, Motivation
NICE 2006 “education alone is unlikely to be effective” Referral to outside agencies Support and encouragement Achievable and sustainable

49
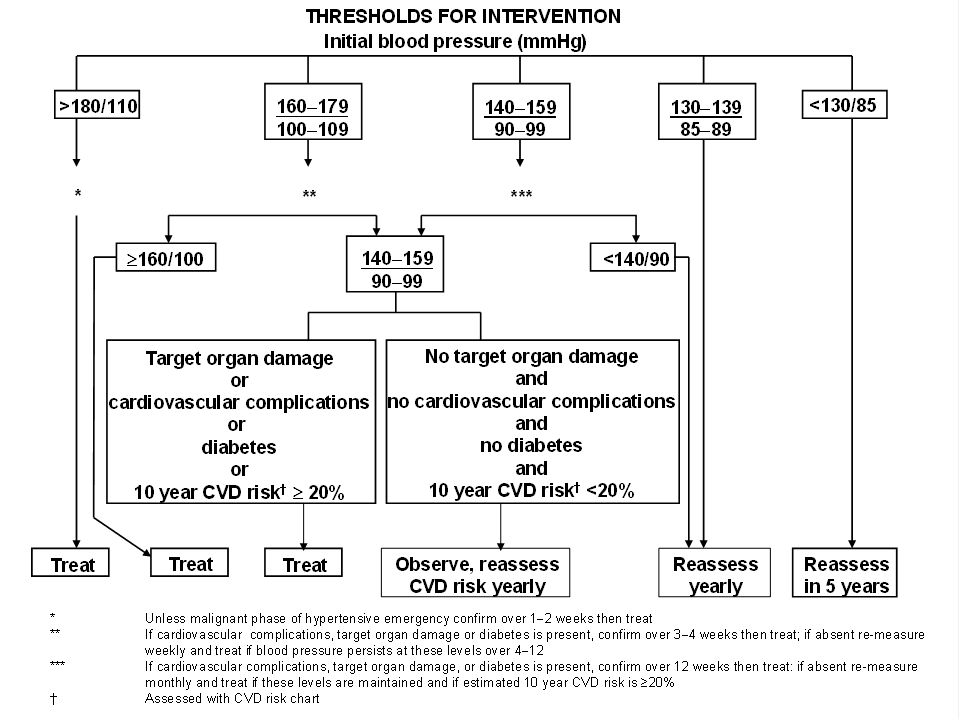
Outcome of annual review of borderline hypertensives

Similar presentations