Download presentation
Presentation is loading. Please wait.

1
Febrile Neutropenia Prof. Arcangelo Liso

2
Recent Guidelines National Comprehensive Cancer Network Clinical Practice Guidelines in Oncology. Prevention and Treatment of Cancer-Related Infections v European Society for Medical Oncology. Management of Febrile Neutropenia: ESMO Clinical Practice Guidelines 2010 Infectious Disease Society of America Guidelines for the Use of Antimicrobial Agents in Neutropenic Patients with Cancer

3
Too many guidelines ?

4
Objectives Identify predisposing factors and common pathogens that cause infections Review initial investigations that will help direct therapy

5
Objectives II Compare recommendations for empiric antibiotic selections for high risk and low risk patients. Discuss assessment of response, treatment modifications and duration of therapy.

6
Incidence of Febrile Neutropenia Induction-remission for AML 70-90%
Elderly patients receiving CHOP 35-45% Mortality Estimates from Febrile Neutropenia Hematological malignancies Up to 11% Gram-positive bacteremia 5% Gram-negative bacteremia 18%

7
Definition of Febrile Neutropenia
Fever: Single oral temperature ≥38.3°C or persistent temperature ≥38.0 °C for >1 hour. Neutropenia: ANC <0.5, or ANC <1.0 and a predicted decline to <0.5 over next 48 hrs. (ANC= absolute neutrophil count)
")
8
Predisposing Factors Malignancy Surgical risk Grade of neutropenia
Type Advanced/refractory Obstructive Surgical risk Grade of neutropenia Disruption of mucosal barriers Corticosteroid use

9
Microbiology Gram-positive Coagulase-negative staphylococci Yeast
S. aureus S.viridans Enterococci Gram-negative Coliforms (E.coli, Klebsiella, Enterobacter) P.aeruginosa Yeast Candida Aspergillus Viruses Herpes simplex (HSV) Influenza, paranifluenza CMV
 P.aeruginosa. Yeast. Candida. Aspergillus. Viruses. Herpes simplex (HSV) Influenza, paranifluenza. CMV.")
10
Initial Investigations
History & physical exam Lab assessments Diagnostic imaging Microbiologic evaluations

11
Detailed H&P Chemotherapy regimen & last dose given Vascular devices
Prophylactic antibiotic Steroid use Allergies Major comorbid illnesses Recent surgical procedures Recent infections or positive cultures Previous antibiotic-resistant organisms Recent exposures

12
Site-Specific H&P Oropharynx Respiratory system Skin Genitourinary CNS
No mucositis Cough Skin lesions Yeast Infection CNS symptoms

13
Lab assessments CBC with differential BUN, SCr, LFTs Electrolytes
Urinalysis

14
Microbiologic evaluations
Blood cultures x2 1 catheter + 1 peripheral Urine culture if symptomatic urinary catheter or abnormal urinalysis

15
Site-Specific Cultures
Diarrhea: C.difficile assay, stool microscopy and culture Sputum microscopy and culture Aspirate/swab/biopsy of any skin lesions Viral tests Vesicular or ulcerated skin/mucosal lesions Throat or nasopharynx for respiratory symptoms (esp. during outbreaks) LP if CNS symptoms Fungal cultures
 LP if CNS symptoms. Fungal cultures.")
16
Risk Status Assessment
Low Risk High Risk Outpatient at time of fever Inpatient at time of fever No acute comorbid illnesses Significant medical comorbidity Anticipated short duration of severe neutropenia Anticipated severe or prolonged neutropenia No renal insufficiency CrCL <30 ml/min No hepatic insufficiency Transaminases ≥5x ULN Good performance status Uncontrolled/progressive cancer, Mucositis grade 3-4 MASCC Risk Index score ≥21 MASCC Risk Index score <21 Complex infection

17
Klastersky J,J Clin Oncol 2000; 18:3038–51.
MASCC Index Multinational Association for Supportive Care in Cancer Prospectively validated tool to rapidly assess risk before access to neutrophil count. Scores 21 are at low risk of complications (max score 26). MASCC scoring index: Burden of illness: no or mild symptoms 5 Burden of illness: moderate symptoms 3 Burden of illness: severe symptoms 0 No hypotension (systolic BP >90 mmHg) 5 No chronic obstructive pulmonary disease 4 Solid tumour/lymphoma with no previous fungal infection 4 No dehydration 3 Outpatient status at onset of fever 3 Age <60 years (not valid in children <18 years) 2 Klastersky J,J Clin Oncol 2000; 18:3038–51.
. MASCC scoring index: Burden of illness: no or mild symptoms 5. Burden of illness: moderate symptoms 3. Burden of illness: severe symptoms 0. No hypotension (systolic BP >90 mmHg) 5. No chronic obstructive pulmonary disease 4. Solid tumour/lymphoma with no previous fungal infection 4. No dehydration 3. Outpatient status at onset of fever 3. Age <60 years (not valid in children <18 years) 2. Klastersky J,J Clin Oncol 2000; 18:3038–51.")
18
Low Risk Treatment Low risk, adult patients Vigilant observation
No focus of infection, hemodynamically stable No systemic symptoms other than fever No organ failure, pneumonia, soft tissue infection Recovering bone marrow Reliable patient Vigilant observation Access to medical care 24-7 Return to clinic if Positive cultures Persistent/recurrent fever (3-5 days) Unable to tolerate PO regimen Cipro 500 mg PO Q8h + amoxicillin-clavulanate 500 mg PO Q8h
 Unable to tolerate PO regimen. Cipro 500 mg PO Q8h + amoxicillin-clavulanate 500 mg PO Q8h.")
19
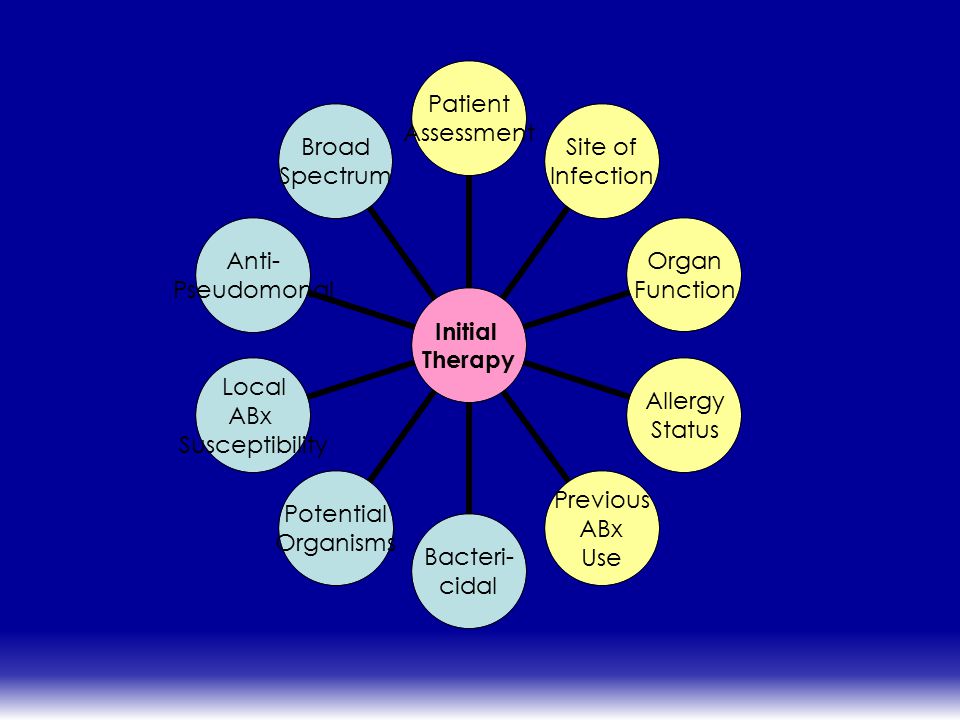
Principles of High Risk Treatment
Inpatient treatment with IV antibiotics (60 min) Coverage for MRSA or resistant Gram-negative bacteria may be required. Monotherapy is equivalent to combinations (with few exceptions)
 Coverage for MRSA or resistant Gram-negative bacteria may be required. Monotherapy is equivalent to combinations (with few exceptions)")
21
IV Monotherapy Cefepime Imipenem-cilastin Meropenem**
Piperacillin-tazobactam** (NCCN) Ceftazidime** (with concerns) **Formulary (all others Non-formulary at THC) The options for IV monotherapy are consistent between guidelines and are listed here in alphabetical order except that ceftazidime is not preferred due to reduced efficacy against gram-positive and ESBL organisms. Quinolones have been evaluated as monotherapy but have shown equivocal results in clinical trials (some positive and some negative) and are not recommended in the current versions of any of the guidelines.
 Ceftazidime** (with concerns) **Formulary (all others Non-formulary at THC) The options for IV monotherapy are consistent between guidelines and are listed here in alphabetical order except that ceftazidime is not preferred due to reduced efficacy against gram-positive and ESBL organisms. Quinolones have been evaluated as monotherapy but have shown equivocal results in clinical trials (some positive and some negative) and are not recommended in the current versions of any of the guidelines.")
22
IV Combination Therapy
Advantages: Synergistic effect against gram-neg Reduced emergence of resistance Disadvantages: Lack of activity against gram-pos? Toxicity

23
IV Combination Therapy
Aminoglycoside + (meropenem, imipenem-cilastin or piperacillin-tazobactam) Aminoglycoside + (cefepime or ceftazidime) Ciprofloxacin + (meropenem, imipenem-cilastin or piperacillin-tazobactam) Although meta-analysis found equivalent efficacy, bactericidal activity and synergistic effect of a b-lactam antibiotic in combination with an aminoglycoside is preferable to monotherapy with antipseudomonal cephalosporins in high risk patients. Although there have been many comparative trials, results have proven similar in meta-analysis when study design variations are taken into consideration.
 Aminoglycoside + (cefepime or ceftazidime) Ciprofloxacin + (meropenem, imipenem-cilastin or piperacillin-tazobactam) Although meta-analysis found equivalent efficacy, bactericidal activity and synergistic effect of a b-lactam antibiotic in combination with an aminoglycoside is preferable to monotherapy with antipseudomonal cephalosporins in high risk patients. Although there have been many comparative trials, results have proven similar in meta-analysis when study design variations are taken into consideration.")
24
IV Therapy Options: Comparison
Piperacillin-tazobactam Broad spectrum gram(-), gram(+) & anaerobic coverage Use for intra-abdominal source Not recommended for meningitis (poor CSF penetration) Imipenem-cilastin Broad spectrum gram(-), gram(+) & anaerobic and ESBL coverage Risk of seizures in CNS malignancy or renal impairment
, gram(+) & anaerobic coverage. Use for intra-abdominal source. Not recommended for meningitis (poor CSF penetration) Imipenem-cilastin. Broad spectrum gram(-), gram(+) & anaerobic and ESBL coverage. Risk of seizures in CNS malignancy or renal impairment.")
25
IV Therapy Options: Comparison
Meropenem Broad spectrum gram(-), gram(+) & anaerobic and ESBL coverage Use for intra-abdominal source Preferred for meningitis/CNS infection Ceftazidime Poor gram(+) activity Breakthrough streptococcal infections No activity against anaerobes, enterococcus Good CSF penetration
, gram(+) & anaerobic and ESBL coverage. Use for intra-abdominal source. Preferred for meningitis/CNS infection. Ceftazidime. Poor gram(+) activity. Breakthrough streptococcal infections. No activity against anaerobes, enterococcus. Good CSF penetration.")
26
IV Treatment Options: Comparison
Aminoglycosides Gram(-) coverage, synergy with beta-lactams against S.aureus and Enterococcus Nephrotoxicity, ototoxicity Ciprofloxacin Gram(-) and atypical bacterial coverage No anaerobic coverage, less gram(+) activity than other options Good clinical studies as empirical PO or IV therapy Avoid in patients recently treated with quinolone prophylaxis Levofloxacin: better gram (+) coverage but limited studies available for use as empiric therapy.
 coverage, synergy with beta-lactams against S.aureus and Enterococcus. Nephrotoxicity, ototoxicity. Ciprofloxacin. Gram(-) and atypical bacterial coverage. No anaerobic coverage, less gram(+) activity than other options. Good clinical studies as empirical PO or IV therapy. Avoid in patients recently treated with quinolone prophylaxis. Levofloxacin: better gram (+) coverage but limited studies available for use as empiric therapy.")
27
Vancomycin Vancomycin not routinely recommended
Use should be limited to specific indications: clinically suspected serious catheter-related infection known colonization with MRSA or pcn/ceph-resistant pneumococci gram-positive bacteremia hypotension soft-tissue infection severe mucositis Reassess Vancomycin after hours

28
Antifungals as Empiric Therapy?
High risk patients with prolonged neutropenia and site-specific symptoms: Oral thrush: Mucositis mouthwash, Fluconazole Esophageal lesions: Fluconazole Sinus/nasal symptoms and suspicious CT/MRI: Amphotericin B Pneumonia: voriconazole, amphotericin B Empiric treatment required based on H&P as positive cultures can take several days.

29
Antifungals Added Later?
IDSA recommends consider antifungal if febrile after 3-5 days and remains neutropenic Amphotericin B is preferred Fluconazole may be acceptable at institutions with low rates of mold infections or drug-resistant Candida species

30
Antifungals Added Later?
NCCN recommends: Add fluconazole if no prior azole antifungal prophylaxis, low risk for invasive aspergillosis and low rates of azole-resistant Candida. Dosing: 150 mg PO x1 dose for vaginal candidiasis 200 mg PO daily x14 days for candidal pyelonephritis 800 mg x1 then 400 mg daily x14 days from first negative culture for candidiasis (not recommended if received prophylaxis) 400 mg PO daily prophylaxis for neutropenic patients
 400 mg PO daily prophylaxis for neutropenic patients.")
31
Antifungals Added Later?
NCCN Recommends Add voriconazole, liposomal amphotericin B or an echinocandin if already exposed to an azole or known to be colonized with non-albicans Candida. Voriconazole 6 mg/kg IV q12h x2 doses then 4 mg/kg IV/PO q12h Amphotericin B 3-5 mg/kg IV daily Caspofungin 70 mg IV x1 then 50 mg IV daily; 70 mg IV daily for aspergillosis Continue until neutropenia has resolved, or for at least 14 days in patients with a demonstrated fungal infection.

32
When to Add Antiviral Therapy
Oral vesicular lesions: HSV Esophageal lesions: HSV, CMV Skin lesions: VZV Pneumonia: Influenza CNS symptoms: HSV

33
Antiviral Doses Acyclovir: Valacyclovir: Ganciclovir: Foscarnet:
Mucocutaneous HSV: 5 mg/kg IV Q8h Single dermatomal VZV: 800 mg PO 5x/day or 5 mg/kg IV Q8h Disseminated VZV or HSV: 10 mg/kg IV Q8h Valacyclovir: HSV or VZV treatment: 1g PO Q8h Ganciclovir: CMV treatment: 5 mg/kg IV Q12h x2 weeks then 5 mg/kg IV Q24h x2-4 weeks Foscarnet: Acyclovir-resistant HSV: 40 mg/kg IV Q8h CMV treatment: 90 mg/kg IV Q12h x2 weeks then 120 mg/kg IV Q24h x2-4 weeks Oseltamivir: Influenza: 75 mg PO Q12h (reduced doses required in renal impairment)
")
34
Assessment of Response
Daily assessment until afebrile and ANC 0.5: Fever CBC Renal function Clinical Symptoms

35
Duration of Therapy Afebrile and ANC 0.5 x48 hrs:
Low risk patients, no source of infection identified: can discontinue abx High risk patients or with documented infection: continue tailored therapy 7 days Afebrile but ANC <0.5 after 5-7 days: low risk: can discontinue abx high risk: continue abx until ANC 0.5 or 14 days in pts not expecting ANC recovery. Febrile: Neutropenic: continue abx at least 14 days, reassess for non-response Non-neutropenic: discontinue abx 4-5 days after ANC >0.5 if no source of infection identified IDSA: Time to devervescence: 2-7 days, Median time to clinical response: 5-7 days IDSA 2002 Guidelines for the Use of Antimicrobial Agents in Neutropenic Patients with Cancer

36
Follow up for Non-Responsive Patients
Febrile but otherwise stable If non-neutropenic consider stop abx 4-5 days after ANC >0.5 Consider antifungal therapy with activity against mold if fever continuing ≥4-5 days. Febrile and clinically unstable Broaden coverage to include anaerobes, resistant gram negative, resistant gram positive organisms Ensure coverage of Candida Consider antifungal therapy with activity against mold if fever continuing ≥4 days of therapy ID consult

37
Duration of Therapy for Documented Infection
Skin/soft tissue: 7-14 days Sinusitis: days Bacterial pneumonia: days

38
Duration of Therapy for Documented Infection
Uncomplicated bacteremia: Gram negative: days Gram positive: 7-14 days S.aureus: at least 2 weeks after first negative blood culture and normal TEE Yeast: ≥2 weeks after first negative blood culture

39
Duration of Therapy for Documented Infection
Aspergillus min 12 weeks Viral: HSV/VZV: 7-10 days Influenza: ≥5 days.

40
Future directions Compare the role of oral therapy and IV monotherapy
Antibiotic lock solutions for CVADs New role for new CSFs ?

42
Pneumonia Additional Tests: If high risk consider adding
sputum cultures Nasal wash for respiratory viruses Legionella urine antigen test Consider BAL If high risk consider adding CT chest to define infiltrates ID Consult Include coverage for: atypical bacteria with azithromycin P.jirovecii with Septra MRSA with vancomycin or linezolid adding antiviral therapy (influenza outbreak) mold-active antifungal (voriconazole or liposomal amphotericin B) if high risk
 mold-active antifungal (voriconazole or liposomal amphotericin B) if high risk.")
43
Gastrointestinal Symptoms
Abdominal pain Abdominal CT or ultrasound ALP, transaminases, bilirubin, amylase, lipase Ensure anaerobic coverage Diarrhea C.difficile assay, (rotavirus & norovirus?) Consider stool bacterial cultures +/- parasite exam Metronidazole if C.difficile suspected
 Consider stool bacterial cultures +/- parasite exam. Metronidazole if C.difficile suspected.")
44
Urinary tract symptoms
Urine culture Urinalysis No additional therapy until pathogen identified

45
CNS Symptoms ID consult Neurology consult CT +/- MRI LP recommended
Empiric therapy: Anti-pseudomonal penicillin that enters CSF (ceftazidime, meropenem) Vancomycin Ampicillin unless using meropenem For encephalitis add high dose acyclovir
 Vancomycin. Ampicillin unless using meropenem. For encephalitis add high dose acyclovir.")
Similar presentations







:e56-e93.>")
















