Download presentation
Presentation is loading. Please wait.

1
The Spine Macaire Grobe, Katherine Callahan, Sophia Powell, Bin Chen, and Theo DiPauli

2
Evolution of the Human Spine
The structure of the spine has changed significantly over the course of millions of years of evolution. Notochords in the first vertebrae The development of the spinal cord Transition for humans to walk upright

3
Walking Upright Bone and Joint Adaptions: Spine Adaptions:
Ability to lock our legs Inward thigh bones Arched foot Gluteal Abductor Spine Adaptions: Curved structure of the spine Foramen Magnum

4
Embryonic Development
Spine starts to form during 4th week of embryonic development Notochord: Sclerotome have loosely and densely packed cells. Notochord expands to form the nucleus pulposus, which is later surrounded by circular fibers of the annulus fibrosis. Neural Tube: Mesenchymal cells here forms the vertebral arch. Body Wall: Mesenchymal Cells form the costal processes which develop into ribs in the thoracic region. Chondrification: The centers in the vertebral arches fuse with each other and the centrum The spinous and transverse processes develop from extensions of chondrification centers in the vertebral arch

5
Embryonic Development
Mesenchymal cells from the sclerotome of the somites start to form in three main areas: notochord, neural tube, and body wall In the 6th week, chondrification occurs

6
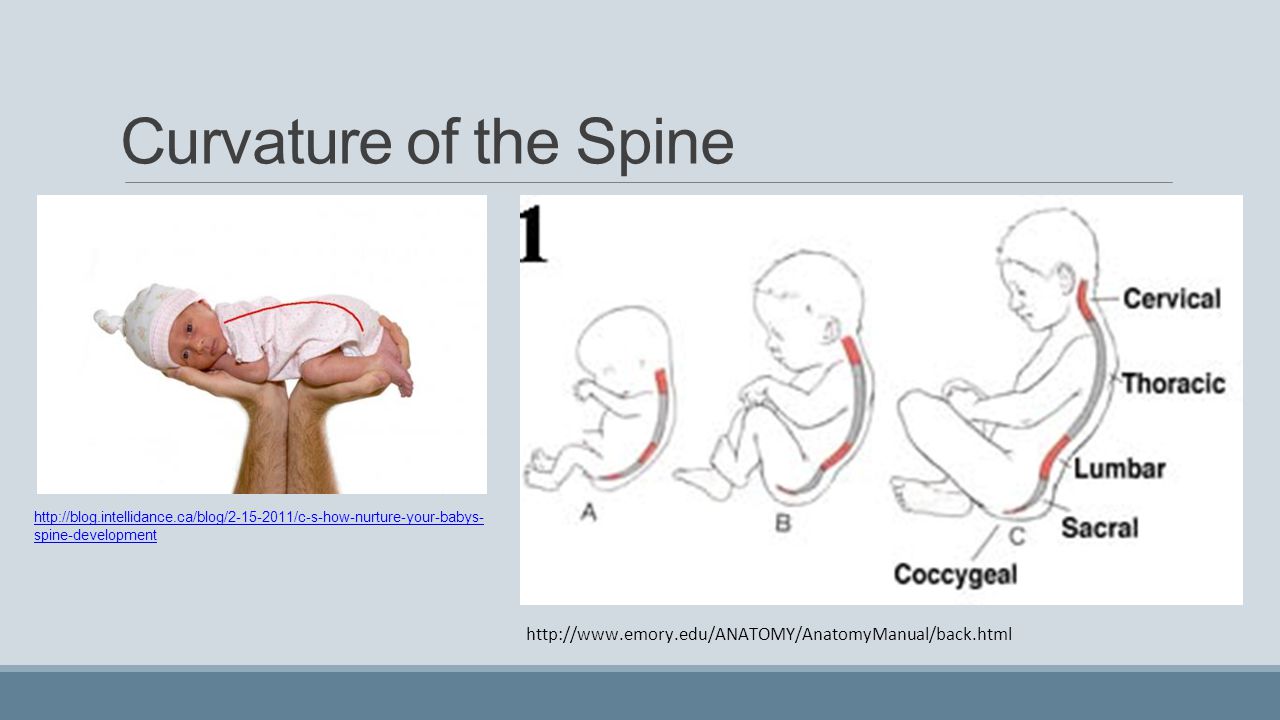
Curvature of the Spine Primary Curve: shaped like a C Secondary Curve: Cervical Spine develops Final Curve: lumbar spine develops
7
Biomechanics of Spinal Injuries
The spine shares a similar structure to a flexible segmented column. Offers strong support Prone to various kinds of injuries Fractures of the spine can be classified by: Causal Movement Location Shape Severity

8
Classifications of Fractures:
Three Column Concept Major and Minor Fractures Stable vs. Unstable Specific Fracture Types: Compression Flexion Burst Dislocation Three Column Concept Major and Minor Fractures

9
Classifications of Fractures:
Stable vs. Unstable Specific Fracture Types

10
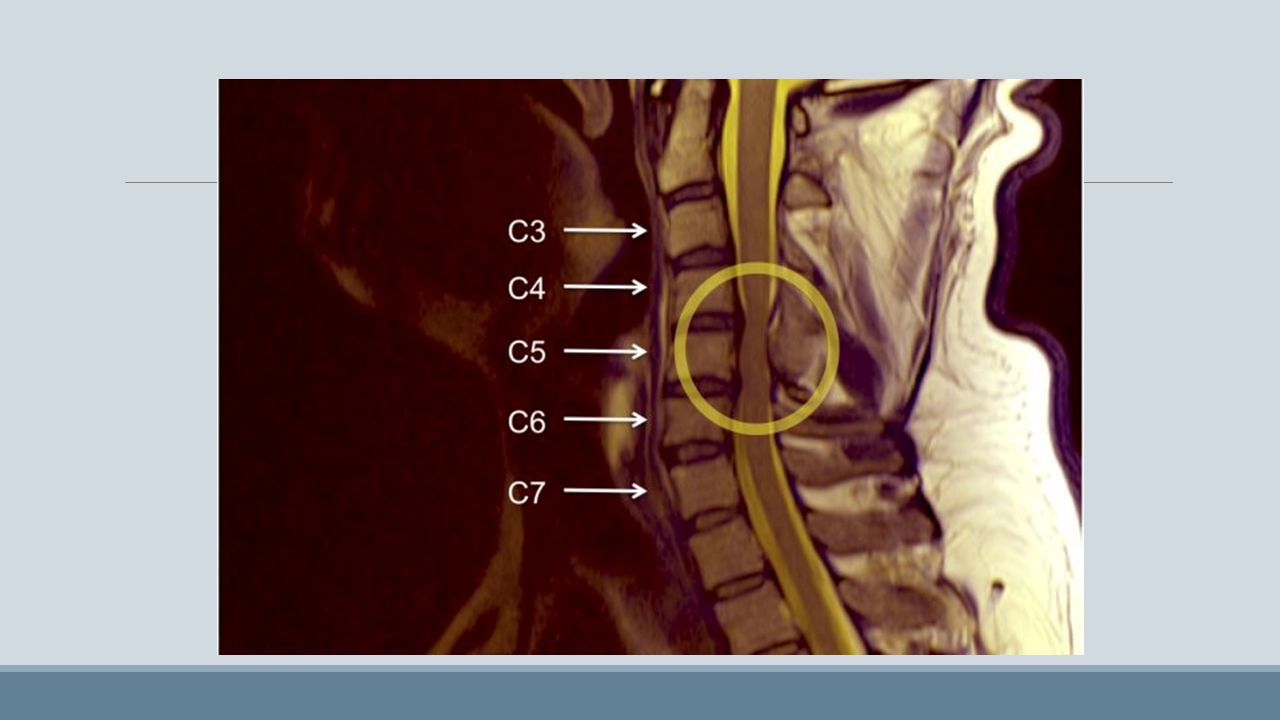
Spinal Cord Injury: What is spinal cord injury? Why is it significant?
A spinal cord injury occurs when there is damage to the spinal cord either from trauma, loss of its normal blood supply, or compression from tumor or infection. Why is it significant? The spinal cord is incapable of healing itself. Complete spinal cord injury: cannot send signals below the level of injury. Incomplete spinal cord injury: some movement and sensation below the injury.

11
Spinal Cord Injury: Causes:
The most common cause of spinal cord injury is trauma. Types of trauma include: falls from heights, violence (stabbing or gunshot wounds to the spine), or sporting injuries (diving, football, rugby, equestrian, etc.) Spinal cord injury can also be caused by compression of the cord by a tumor, infection, or inflammation. Spinal stenosis Types of trauma include: falls from heights, violence (stabbing or gunshot wounds to the spine), or sporting injuries (diving, football, rugby, equestrian, etc.)
, or sporting injuries (diving, football, rugby, equestrian, etc.) Spinal cord injury can also be caused by compression of the cord by a tumor, infection, or inflammation. Spinal stenosis. Types of trauma include: falls from heights, violence (stabbing or gunshot wounds to the spine), or sporting injuries (diving, football, rugby, equestrian, etc.)")
12
Conditions that affect the spinal cord:
Tumors Infections such as meningitis and polio Inflammatory diseases Autoimmune diseases Degenerative diseases such as amyotrophic lateral sclerosis and spinal muscular atrophy

13
Diseases of the Spinal Cord:
Meningitis Polio Amyotrophic lateral sclerosis (ALS) Spinal muscular atrophy (SMA)
 Spinal muscular atrophy (SMA)")
14
Spine Treatment Level 1: Mobilization and Physical Therapy
Level 2: Immobilization, Braces Level 3: Spinal Surgery; Fusion, Disk Implants

15
Level 1: Mobilization and Physical Therapy
Two components: Passive physical therapy (heat/ice packs, ultrasound) Active Exercises (stretching) Manual physical therapy: Restore mobility Reduce muscle tension
 Active Exercises (stretching) Manual physical therapy: Restore mobility. Reduce muscle tension.")
16
Level 2: Immobilization, Braces
Spinal bracing used for treatment of: low back pain trauma infections muscle weakness neck conditions osteoporosis

17
Cervical Braces Soft and hard collars Philadelphia collar
Sterno-occipital-mandibular immobilization device (SOMI) Halo
 Halo.")
18
Back Braces Two types of back braces commonly used: Rigid braces
Corset (elastic braces)
")
19
Level 3: Spinal Surgery; Fusion, Disk Implants
Spinal Fusion Artificial Disk Replacement (ADR)
")
20
Fusion Involves forming direct connection between vertebrae surrounding the painful disc(s) Pain relief occurs by stopping the motion of the painful disc(s).
.")
21
Fusion

22
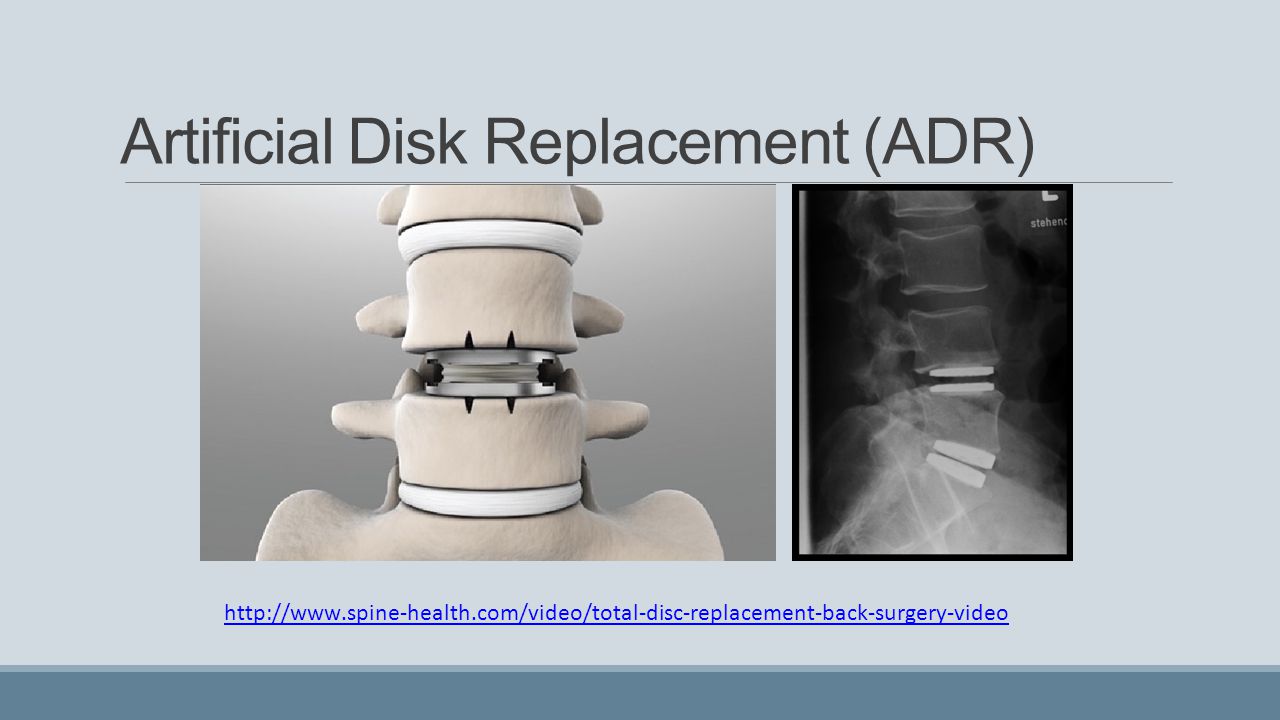
Artificial Disk Replacement (ADR)
Alternative to spinal fusion replaces damaged or worn out spinal disc with an artificial disc The Charité artificial disc is made of two metallic endplates and a plastic center

23
Artificial Disk Replacement (ADR)
24
Christopher Reeve In 1995, famous actor Christopher Reeve broke his neck in a horseback riding incident. Paralyzed from neck down and unable to breathe

25
Background on the injury
Second vertebrate (C2) causes instant death if displaced laterally by 5mm Fracture in any cervical vertebrate causes quadriplegia Spinal cord injuries breaks nerve fibers Destroys possible muscle movement in distal direction
 causes instant death if displaced laterally by 5mm. Fracture in any cervical vertebrate causes quadriplegia. Spinal cord injuries breaks nerve fibers. Destroys possible muscle movement in distal direction.")
26
Survived instant death
Survived 60-70% chance mortality rate over the following week No recovery within 48 hours usually means no recovery

27
Spinal Cord Concussion
Cervical Cord neurapraxia (CNN) Nerrowing of the spinal canal (stenosis) Torg or Pavlov ratios: Ratio of canal diamter to vertebral body 0.8< indicates significant for athletic Instantaneous loss of function of limbs but followed with complet recovery Most commonly occurs at the cervical vertabrates
 Nerrowing of the spinal canal (stenosis) Torg or Pavlov ratios: Ratio of canal diamter to vertebral body. 0.8< indicates significant for athletic. Instantaneous loss of function of limbs but followed with complet recovery. Most commonly occurs at the cervical vertabrates.")
29
Torg. J. et al, 1997

30
Both techniques share the same level of reoccurrence
Torg. J. et al, 1997

31
How does it happen? Hyperextension, hyperflexion, axial load mechanisms on neck Spear tackle Occur in 7 out of 10,000 players per year (1.8 million people) and rising
 and rising. v=UpdrHe31J-8.")
32
Why the rise? Helmets are too safe!

33
Long term effects Symptoms subside usually after 24 hours
56% chance of reoccurrence Repeat episode is directly proportional to diameter of player’s cervical spine canal If neurologic symptoms persist surgery Second episode termination of sport

34
Torg. J. et al, 1997

35
Case compilation of different CNN outcomes of athletes

36
Case Study Example 20 year old college defensive back
5 minutes of transient paralysis C-3, 5 narrowing of 0.66 C-4 narrowing of 0.62 Minimal anterior subluxation Returned to play after recovery

37
Minimal Flexion

38
… Fourteen months later
Contact is made with head Classic spear tackle Axial load Fracture in the C4-C6 vertebrate

39
*Unilateral facet dislocation at C4-5 (C4 displaced anteriorly 25%) in sagittal plane
*Oblique fracture *Three-part-two-plane fracture with small anterior fracture fragment *Non-displaced sagittal fracture through the vertebral body and partial fracture of the right lamina

40
Help efforts Christopher and Dana Reeve Paralysis Resource Center
Located in New Jersey Funds for research, treatments/cures, for CNS disorders Advocate improvement of quality of life post-injury 22M to neuroscientist research

41
References [1] [2] [3] [4] [5] [6]
![References [1] [2]](http://slideplayer.com/slide/4316211/14/images/41/References+%5B1%5D+++%5B2%5D.jpg "[3] [4] [5] [6]")
Similar presentations