Download presentation
Presentation is loading. Please wait.

1
John F Eidt MD University of Arkansas for Medical Sciences
Thrombophilia John F Eidt MD University of Arkansas for Medical Sciences

2
Thrombophilia Acquired or inherited tendency toward accelerated thrombosis

3
THROMBOPHILIAC? Hemophilia is to Hemophiliac as
Thrombophilia is to ………? THROMBOPHILIAC?

4
Classification of thrombophilia
1. Qualitative/quantitative defect of coagulation factor inhibitors a) Antithrombin deficiency b) Protein C deficiency c) Protein S deficiency d) Heparin cofactor II deficiency e) Tissue factor pathway inhibitor deficiency f) Thrombomodulin deficiency 2. Increased levels/function of coagulation factors a) Activated protein C resistance and factor V Leiden b) Prothrombin gene mutation (G20210A) c) Dysfibrinogenemia and hyperfibrinogenemia d) Elevated levels of clotting factors VII, VIII, IX, XI, and XII 3. Hyperhomocysteinemia 4. Defects of the fibrinolytic system a) Plasminogen b) Tissue plasminogen activator c) Thrombin-activatable fibrinolysis inhibitor d) Factor XIII e) Lipoprotein (a) 5. Altered platelet function a) Platelet glycoprotein GPIb-IX b) GPIa-IIa c) GPIIb-IIIa
 Antithrombin deficiency. b) Protein C deficiency. c) Protein S deficiency. d) Heparin cofactor II deficiency. e) Tissue factor pathway inhibitor deficiency. f) Thrombomodulin deficiency. 2. Increased levels/function of coagulation factors. a) Activated protein C resistance and factor V Leiden. b) Prothrombin gene mutation (G20210A) c) Dysfibrinogenemia and hyperfibrinogenemia. d) Elevated levels of clotting factors VII, VIII, IX, XI, and XII. 3. Hyperhomocysteinemia. 4. Defects of the fibrinolytic system. a) Plasminogen. b) Tissue plasminogen activator. c) Thrombin-activatable fibrinolysis inhibitor. d) Factor XIII. e) Lipoprotein (a) 5. Altered platelet function. a) Platelet glycoprotein GPIb-IX. b) GPIa-IIa. c) GPIIb-IIIa.")
5
Prevalence of thrombophilia

6
Relative risk of first episode DVT
APLA Antithrombin deficiency 20 Protein C deficiency (Hetero) 10 Protein S deficiency 10 Homozygous Factor V Leiden 80 Heterozygous Factor V Leiden 7 Elevated FVIII 5 Prothrombin gene mutation Homocystenemia 3 OBCP OBCP and heterozygous Factor V 35
 10. Protein S deficiency 10. Homozygous Factor V Leiden 80. Heterozygous Factor V Leiden 7. Elevated FVIII 5. Prothrombin gene mutation Homocystenemia 3. OBCP 4. OBCP and heterozygous Factor V 35.")
7
? XII XIIa

8
XII XIIa XI XIa

9
XII XIIa XI XIa IX IXa

10
XII XIIa TENASE Complex XI XIa IX IXa Ca++ VIIIa PL VIII X Xa

11
XII XIIa XI XIa Tissue Factor VIIa VII IX IXa X Xa

12
XII XIIa XI XIa IX IXa X Xa

13
PROTHROMBINASE Complex
XII XIIa XI XIa PROTHROMBINASE Complex IX IXa X Xa Ca++ Va PL Va II IIa (Thrombin)
")
14
Thrombin is the central bioregulatory enzyme in hemostasis
XII XIIa XI XIa Thrombin is the central bioregulatory enzyme in hemostasis IX IXa X Xa Ca++ Va PL Va II IIa (Thrombin)
")
15
Pro-thrombotic actions of THROMBIN
vWF(ADAMST13) XII XIIa Platelets PARS 1 &4 XI XIa IX IXa X Xa VIIIa II IIa (Thrombin) Va I Ia (Fibrin) XIIIa XIII TAFI Cross-linked Ia (Fibrin) Pro-thrombotic actions of THROMBIN
 XII. XIIa. Platelets. PARS 1 &4. XI. XIa. IX. IXa. X. Xa. VIIIa. II. IIa (Thrombin) Va. I. Ia (Fibrin) XIIIa. XIII. TAFI. Cross-linked Ia (Fibrin) Pro-thrombotic actions of THROMBIN.")
16
XII XIIa XI XIa Tissue Factor VIIa VII IX IXa X Xa VIII VIIIa II IIa (Thrombin) V Va I Ia (Fibrin) XIIIa XIII Cross-linked Ia (Fibrin)
 XIIIa. XIII. Cross-linked Ia (Fibrin)")
17
Anti-thrombotic actions of ECs
Binding of thrombin to thrombomodulin Activation of protein C Release of tPA Prostacyclin

18
Activated Protein C Thrombin Protein C TM ECPR

19
(PS and FV are cofactors for aPC)
XII XIIa XI XIa Tissue Factor VIIa VII IX IXa aPC Vac X Xa aPC VIII VIIIa aPC II IIa (Thrombin) V Va I Ia (Fibrin) (PS and FV are cofactors for aPC)
 V. Va. I. Ia (Fibrin) (PS and FV are cofactors for aPC)")
20
aPC XII XIIa XI XIa Tissue Factor VIIa VII IX IXa X Xa aPC VIII VIIIa
IIa (Thrombin) V Va I Ia (Fibrin) Plasmin Plasminogen tPA EC PAR1
 V. Va. I. Ia (Fibrin) Plasmin. Plasminogen. tPA. EC PAR1.")
21
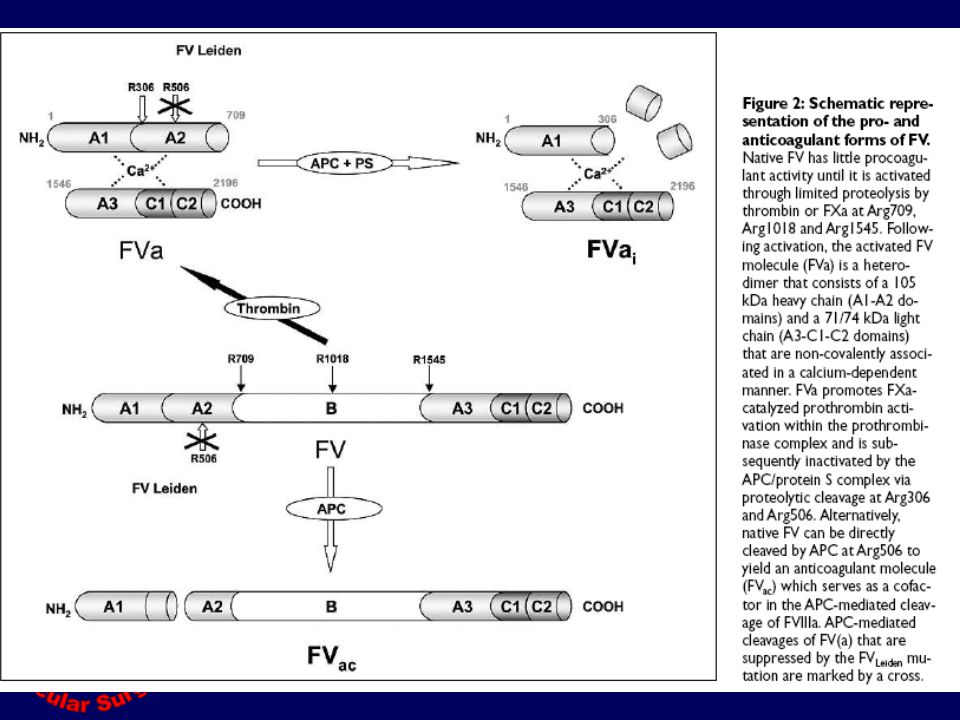
XII XIIa Tissue Factor XI XIa VIIa VII IX IXa aPC X Xa VIII VIIIa II IIa (Thrombin) V LEIDEN Va I Ia (Fibrin) FV Leiden is NOT deactivated by APC and does not act as cofactor (FVac) for FVIIIa inactivation
 FV Leiden is NOT deactivated by APC and does not act as cofactor (FVac) for FVIIIa inactivation.")
22
XII XIIa Tissue Factor TFPI XI XIa VIIa VII IX IXa VIIa Inhibitor X Xa VIII VIIIa II IIa (Thrombin) V Va I Ia (Fibrin)
 V. Va. I. Ia (Fibrin)")
23
Antithrombin XII XIIa Tissue Factor XI XIa VIIa VII IX IXa X Xa VIII
VIIIa II IIa (Thrombin) V Va I Ia (Fibrin)
 V. Va. I. Ia (Fibrin)")
24
XII XIIa Tissue Factor XI XIa VIIa VII IX IXa Heparin X Xa Antithrombin VIII VIIIa II IIa (Thrombin) V Va I Ia (Fibrin)
 V. Va. I. Ia (Fibrin)")
26
Antithrombin deficiency
Auto dom (males=females) 1% of VTE Homozygous lethal in utero Heterozygous 40-70% of normal AT level Clinical presentation late teens and early adulthood 20-fold relative risk May be acquired – nephrotic syndrome
 1% of VTE. Homozygous lethal in utero. Heterozygous 40-70% of normal AT level. Clinical presentation late teens and early adulthood. 20-fold relative risk. May be acquired – nephrotic syndrome.")
27
Clinical detection Functional assay (HCII based)
Immunogenic assay for protein components One or both assays may be deficient

28
Clinical subtypes Type I - Decreased functional activity and decreased levels of normal protein Type II - Decreased functional activity and normal protein level Abnormalities in thrombin binding site Abnormalities in heparin binding site (lower risk)
")
29
Protein C deficiency Auto Dom Vit K dependent (II, VII, IX, X, C & S)
aPC inactivates Va and VIIIa 3-5% of pts with VTE 10 fold relative risk Both functional and immunogenic deficiencies have been described Warfarin-induced skin necrosis Homozygous neonatal purpura fulminans

30
Protein S Deficiency Auto Dom
Co-factor for aPC inactivation of Va and VIIIa Low level direct (aPC independent) inactivation of Va and VIIIa Produced by liver (vit K dependent), ECs and megakaryocytes Free (40%) and bound (60%) to C4bBP C4bBP increased in pregnancy, OBCP, inflammation and acute thrombosis results in decreased free S Warfarin-induced skin necrosis Homozygous neonatal purpura fulminans
 inactivation of Va and VIIIa. Produced by liver (vit K dependent), ECs and megakaryocytes. Free (40%) and bound (60%) to C4bBP. C4bBP increased in pregnancy, OBCP, inflammation and acute thrombosis results in decreased free S. Warfarin-induced skin necrosis. Homozygous neonatal purpura fulminans.")
31
Heparin Cofactor II Deficiency
Direct thrombin inhibitor – accelerated by heparin, glycosoaminoglycans Uncommon Low risk of thrombosis Esp in association with another thrombotic factor

32
TFPI Tissue Factor Pathway Inhibitor
Inhibits activation of factor X by tissue factor/VIIa pathway Clinical relevance is uncertain

33
Thrombomodulin deficiency
ARIC inverse relationship between TM levels of and risk of CHD Clinical implications unknown Recombinant TM has been developed as novel anticoagulant with no hemorrhagic risk

34
Prothrombin Gene g20210a 2-5% in healthy population
7-18% in VTE patients Mutation in non-transcribed portion of prothrombin gene resulting in elevated levels of prothrombin Common in association with FV Leiden May have higher risk of PE than FV Leiden 1-3 fold increased risk of first VTE

35
Prothrombin G20210A (carrier) effect on recurrent VTE
Haematologica/the hematology journal | 2007; 92(08) | 1107
 |")
36
Factor V Single chain 330kda glycoprotein
25% of FV is stored in platelet alpha granules Essential co-factor for Xa activation of prothrombin Also acts as co-factor for aPC inactivation of VIIIa

37
Factor V Leiden Arg506gln Most common inherited thrombophilia
2-10% of healthy population 20-50% of first-time VTE Common in Caucasians, but not found in other ethnic groups such as African, Chinese or Japanese A single mutational event occurred approximately 21,000 years ago 5-10 fold increased risk of first VTE Gene assay

38
APC resistance Addition of aPC does not prolong routine clotting assays (aPTT) 90% - due to FV Leiden (point mutation preventing Va inactivation by APC) 10% - due to increased plasma levels of factor VIII, the presence of antiphospholipid antibodies, older age, pregnancy, and the use of estrogens
 10% - due to increased plasma levels of factor VIII, the presence of antiphospholipid antibodies, older age, pregnancy, and the use of estrogens.")
40
Factor V Leiden (carrier) on risk of recurrent VTE
haematologica/the hematology journal | 2007; 92(08) | 1107
 |")
41
Factor elevations (VII, VIII, IX, XI)
FVIII elevation has been associated with 6-10 fold increased risk of VTE Some believe it should be included in thrombophilia workup Elevations of FVII, IX and XI of uncertain clinical relevance

42
Dysfibrinogenemia Variable susceptibility to degradation by plasmin
Over 250 fibrinogen mutations have been described

43
Hyperhomocysteinemia
Produced in metabolism of methionine Associated with arterial disease and venous thrombosis Acquired due to vitamin deficiency (B6, B12 and folate) or genetic (MTHFR or CBS)
 or genetic (MTHFR or CBS)")
44
Lupus anticoagulant First detected prolongation of PT in a patient with SLE Most result in prolongation of aPTT Not an anticoagulant Not only in SLE

45
APLA Syndrome LA and/or APLA Arterial or venous thrombosis
Thrombocytopenia Recurrent fetal loss

46
Sapporo Criteria

47
APLA and Risk of Recurrent VTE
Marked elevation in the risk of recurrent thrombosis –20 fold With anti-coagulants 3 – 10% risk at 3 years Without anti-coagulants 10 -29% risk at 3 years

48
How do APLAs lead to thrombosis?
Inhibition of prostacyclin (PGI2) Inhibition of PC activation Increase PAIs Direct platelet activation Activation of endothelial cells Increased TF expression on monocytes
 Inhibition of PC activation. Increase PAIs. Direct platelet activation. Activation of endothelial cells. Increased TF expression on monocytes.")
49
Testing Lupus anticoagulant (prolonged aPTT)
PL CA++ Contact factor activator (a) Antiphospholipid antibodies
 Antiphospholipid antibodies.")
50
Common APLA immunoassays
Anticardiolipin (not physiological) Anti-prothrombin Anti-beta-2-glycoprotein I Anti-phosphatidyl-serine Anti-phosphatidyl-ethanolamine Anti-phosphatidyl-choline Anti-phosophatidyl-inositol
 Anti-prothrombin. Anti-beta-2-glycoprotein I. Anti-phosphatidyl-serine. Anti-phosphatidyl-ethanolamine. Anti-phosphatidyl-choline. Anti-phosophatidyl-inositol.")
51
What is cardiolipin and why test for an antibody to it?
Cardiolipin is not physiologically relevant It is a widely available laboratory reagent It is used in the test for syphilis

52
APLA and VTE Anticoagulation for duration of positive APLA
INR 2.0 – 3.0 (contrary to previous recs) Check APLA Q 6-12 mos Discontinue anticoagulant if APLA negative x2
 Check APLA Q 6-12 mos. Discontinue anticoagulant if APLA negative x2.")
53
Asymptomatic APLA Antiplatelet agents widely recommended but no proven benefit No role for therapeutic “prophylactic” anticoagulation Prophylaxis indicated for high risk events (long distance travel, surgery, immobilzation) Role of HRT and OBCP uncertain Patient education - should be informed of presence of APLAs and symptoms of VTE
 Role of HRT and OBCP uncertain. Patient education - should be informed of presence of APLAs and symptoms of VTE.")
54
APLA and arterial thrombosis
Antiplatelet agents - ASA No clear evidence of benefit Most authors do not recommend anticoagulants

55
High risk for thrombosis: Prolonged duration of anticoagulation
Antiphospholipid syndrome More than one thrombophilic defect (e.g. FV Leiden and Prothrombin gene mutation)) Previous VTE at unusual site Strong family history of thrombosis
) Previous VTE at unusual site. Strong family history of thrombosis.")
56
Treatment (1) First time VTE with transient risk factor 3 months VKA
E.g. surgery, immobilization 3 months VKA

57
Treatment (2) First time IDIOPATHIC VTE Recommend – 6-12 months VKA
Suggest – indefinite (esp PE) Reliable patient Risk factors for bleeding
 Reliable patient. Risk factors for bleeding.")
58
Treatment (3) First time VTE and cancer Recommend – 3-6 months LMWH
Then indefinite VKA CLOT - Fragmin study LEE LITE - Hull

59
Treatment (4) First time VTE Recommend 12 months vs indefinite APLA
Combined (e.g. FV Leiden and PG20210) Single factor and STRONG Family history Recommend 12 months vs indefinite
 Single factor and STRONG Family history. Recommend 12 months vs indefinite.")
60
Treatment (5) First time VTE Recommend 6-12 months
ATIII deficiency PC deficiency PS deficiency FV Leiden Prothrombin gene 20210 Homocysteine Elevated FVIII Recommend 6-12 months Prevent Low dose warfarin

61
Treatment (6) Recurrent VTE Recommend indefinite VKA
 Recurrent VTE Recommend indefinite VKA")
62
Pregnancy and venous thromboembolism
Pregnancy is a hypercoagulable state No recommendations for widespread screening No prophylaxis for prior VTE and transient risk factor Prophylaxis with LMWH for pregnancy and thrombophilia (prior VTE or strong family history) Post partum anticoagulation for all with prior VTE - 6 weeks
 Post partum anticoagulation for all with prior VTE - 6 weeks.")
63
Screening for thrombophilia
The main argument in favor of screening asymptomatic relatives of patients with thrombophilia is the possibility of giving advice for primary antithrombotic prevention during circumstances potentially leading to VTE but not usually covered with prophylaxis in normal individuals (e.g. low-risk surgery or pregnancy and pueperium)
")
64
Against screening Expensive Does not alter treatment
Stigmatizes patient/anxiety May have insurance/employer ramifications

65
Screening SOMMA J, SUSSMAN II , RAND JH. An evaluation of thrombophilia screening in an urban tertiary care medical center: a ‘‘real world’’ experience. Am J Clin Pathol 2006 July;126(1):120e127.
:120e127.")
66
Does a positive family history increase the likelihood of detecting inherited thrombophilia?
N=314 pts with VTE Prevalence of thrombophilia Overall 35% Positive FH (at least 1 first deg rel) - 42% Strong FH (at least 2 first deg rel) - 46% Family history and inherited thrombophilia Journal of Thrombosis and Haemostasis 4: 2182–
 - 42% Strong FH (at least 2 first deg rel) - 46% Family history and inherited thrombophilia Journal of Thrombosis and Haemostasis 4: 2182–")
67
Who should be tested for inherited thrombophilia?
No one

68
Who should be tested for inherited thrombophilia?
Idiopathic first time VTE Recurrent VTE Venous thromboembolism at early age Thrombosis in an unusual site, eg mesenteric vein, cerebral vein etc Unexplained neonatal thrombosis Skin necrosis, particularly if on VKA Arterial thrombosis before the age 30 years Unexplained prolonged activated partial thromboplastin time Patients with recurrent fetal loss Relatives of patients with thrombophilic abnormality – very controversial

Similar presentations


 is produced by a shift in the balance between.>")
















>")
