Download presentation
Presentation is loading. Please wait.

2
Soft Tissue Tumors By: Dr. Zahra Meghdadi

3
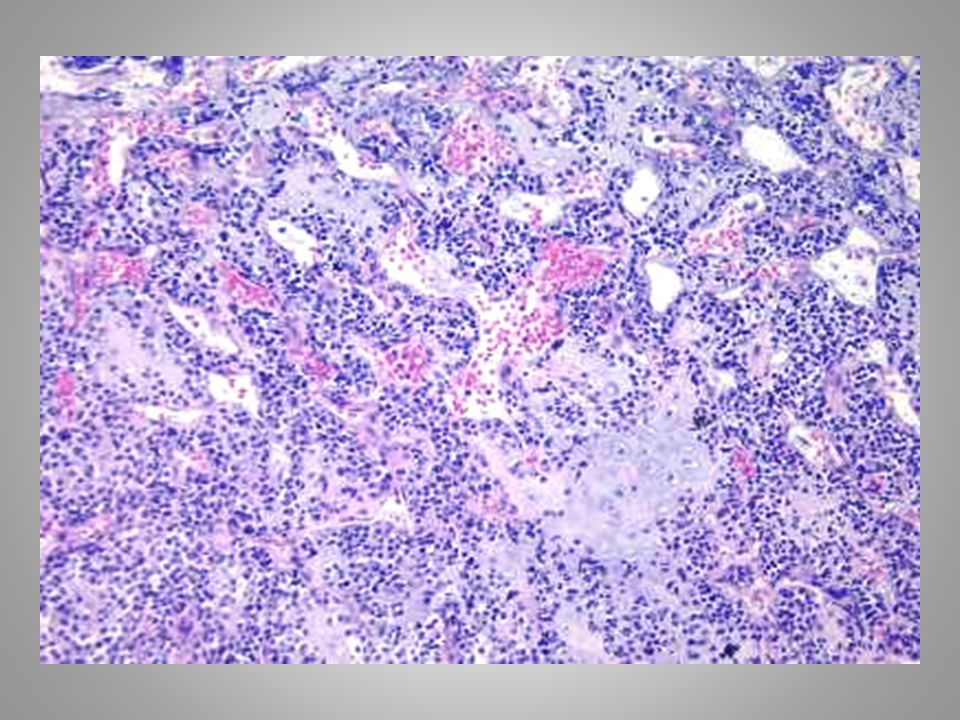
49 year old male with forearm mass
Case 1 49 year old male with forearm mass

7
What’s your diagnosis?

8
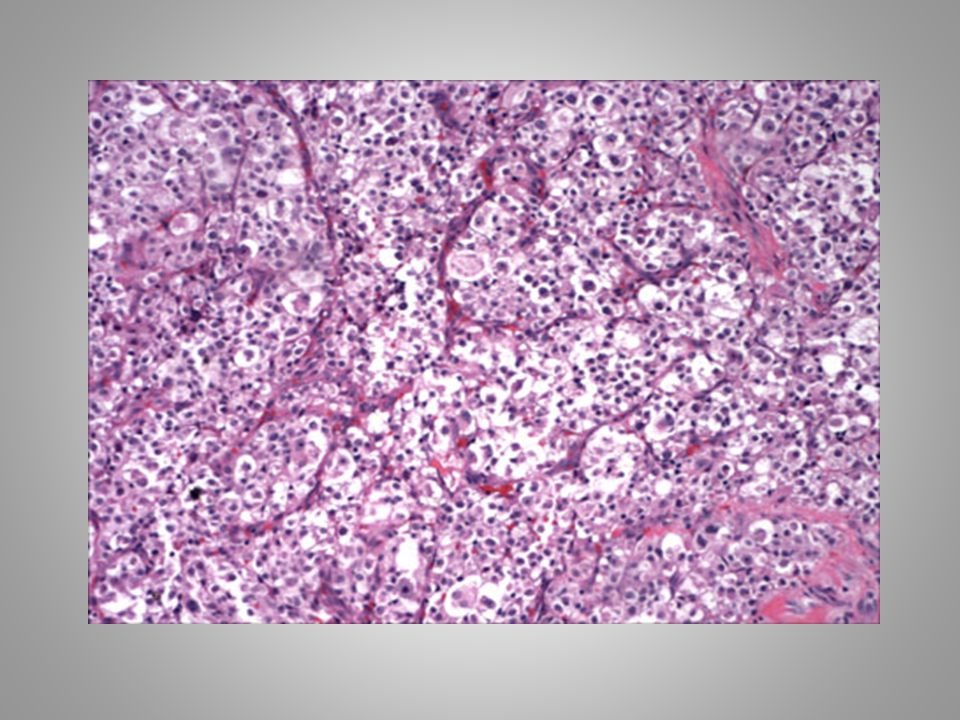
Alveolar Soft Part Sarcoma

9
Alveolar Soft part Sarcoma
The most common sites:deep soft tissues of the thigh and leg. Most patients are young females. Gross:well circumscribed,usually large,moderately firm,gray or yellowish,area of necrosis and hemorrhage are common in larger tumors. This is a nested to alveolar proliferation of epithelioid cells which have eosinophilic granular cytoplasms. The nuclei are vesicular and show prominent nucleoli. Mitoses are exceptional. In children:more solid pattern of growth PAS positive-diastase resistant intracytoplasmic needle like structures IHC:PAX8 (-),TFE3(diffusely +)
,TFE3(diffusely +)")
10
Alveolar Soft Part Sarcoma Behavior & Prognosis:
Slow and indolent clinical course but highly malignant. Vein invasion is common. Blood borne metastases in the lung or… can be seen lately after tumor excision.

11
Alveolar soft part sarcoma Differential diagnosis:
Renal cell carcinoma The absence of PAX8 immunoreactivity argues against this diagnosis. Granular cell tumors label diffusely for S100 protein, and should not show staining for TFE3 in a strong fashion in the majority of cases. Paraganglioma would label for neuroendocrine markers, and should not label for TFE3

12
Mass of the foot (2.5 cm) in a 25 year old man.
Case 2 Mass of the foot (2.5 cm) in a 25 year old man. S100 stain was reactive
 in a 25 year old man. S100 stain was reactive.")
16
What’s your diagnosis?

17
Clear cell sarcoma

18
Clear cell sarcoma Intimately associated with a tendon/aponeurosis .
The most common site:feet Most of the patients are young adults,M>F Gross:well crcumscribed,firm,gray or white,gritty sensation in cut section Consists of highly uniform cells arranged in nests and packets, punctuated by scattered giant cells. Most cells contain uniform enlarged nucleoli. Abundant extracellular and intracellular iron is present. Many tumor cells contain cytoplasmic melanin. IHC: The proliferating cells react with both S100 protein and HMB45 antibodies.

19
Clear cell sarcoma Clear cell sarcomas have been referred to as “malignant melanoma of soft parts” based on this immunophenotype. Differentiation from malignant melanoma: 1) They have a specific translocation (t(12;22); EWS and ATF-1 fusion gene, in contrast to melanomas which have variably abnormal cytogenetic profiles) 2) Their cytologic features are extremely monomorphic rather than pleomorphic 3) They have different survival characteristics
 They have a specific translocation (t(12;22); EWS and ATF-1 fusion gene, in contrast to melanomas which have variably abnormal cytogenetic profiles) 2) Their cytologic features are extremely monomorphic rather than pleomorphic. 3) They have different survival characteristics.")
20
Clear cell sarcoma Differential diagnosis:
1)Malignant melanoma 2) Tenosynovial giant cell tumor: . Tenosynovial giant cells occur in the fingers, typically, of middle-aged females Their proliferating cells lack the prominent nucleoli found in clear cell sarcomas. Pigment found in clear cell sarcomas is melanin whereas that in tenosynovial giant cell tumors is hemosiderin. Tenosynovial giant cell tumors lack S100 protein and do not stain with HMB45 but, desmin is sometimes found in them. 3) Schwannomas: Clear cell sarcomas express S100 protein, but the cells in schwannomas are more spindly and lack large nucleoli 4) Epithelioid sarcomas : Occur in association with aponeuroses and tendon sheaths but they typically feature abundant necrosis and lack nucleoli. They express keratins and CD34 but not S100 protein.
Malignant melanoma. 2) Tenosynovial giant cell tumor: . Tenosynovial giant cells occur in the fingers, typically, of middle-aged females. Their proliferating cells lack the prominent nucleoli found in clear cell sarcomas. Pigment found in clear cell sarcomas is melanin whereas that in tenosynovial giant cell tumors is hemosiderin. Tenosynovial giant cell tumors lack S100 protein and do not stain with HMB45 but, desmin is sometimes found in them. 3) Schwannomas: Clear cell sarcomas express S100 protein, but the cells in schwannomas are more spindly and lack large nucleoli. 4) Epithelioid sarcomas : Occur in association with aponeuroses and tendon sheaths but they typically feature abundant necrosis and lack nucleoli. They express keratins and CD34 but not S100 protein.")
21
Case 3 Posterior chest wall mass from a 87 year old man. There was no overlying ulcer.

26
What’s your diagnosis?

27
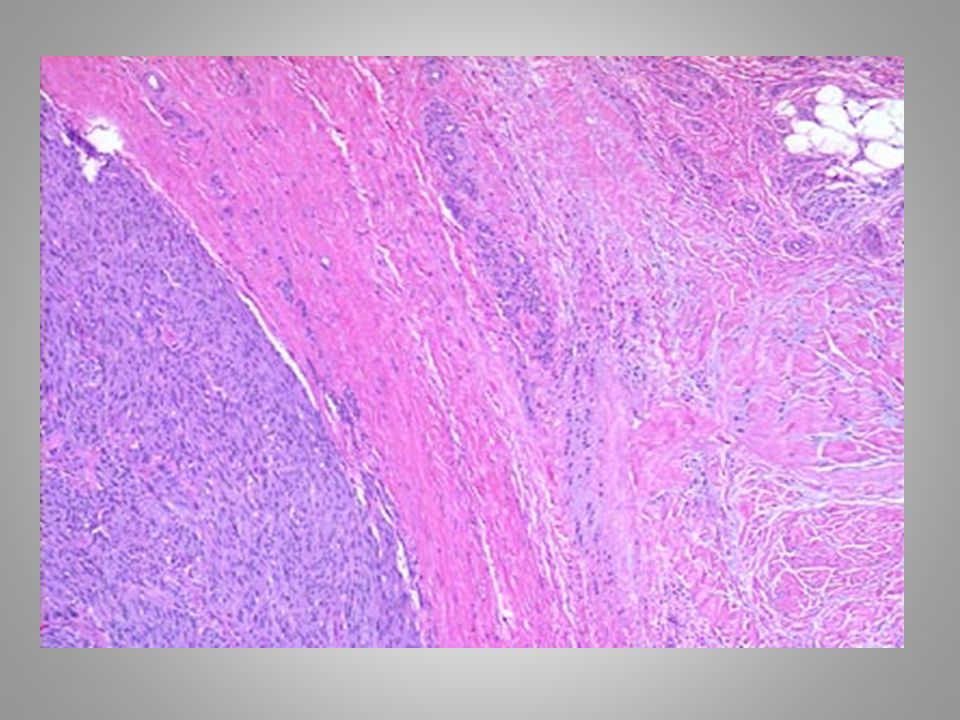
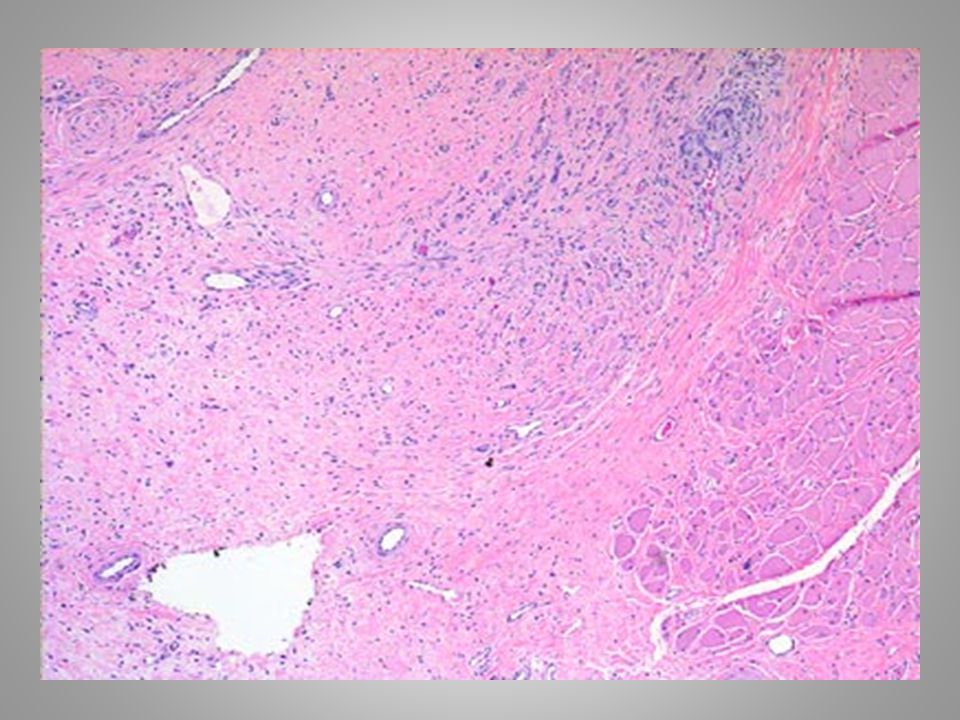
Atypical decubital fibroplasia/ishemic fasciitis

28
Atypical decubital fibroplasia/ishemic fasciitis
This lesion is ill-defined Zones of fibrinoid necrosis within fat lobules into which there is ingrowth of fibroblasts characterized by enlarged nuclei and macronucleoli, smudging of nuclear chromatin, and occasional mitoses. The overall cellularity is low. The proliferating nuclei are quite similar to those encountered in proliferative fasciitis (ganglion-like) but the overall lesion differs by having abundant necrosis
 but the overall lesion differs by having abundant necrosis.")
29
Atypical decubital fibroplasia/ishemic fasciitis
Occurs over bony prominences in bed-ridden (typically elderly) patients Characterized by tumefaction rather than ulceration . It is a benign presumably reactive lesions, although recurrences occasionally occur.
 patients. Characterized by tumefaction rather than ulceration . It is a benign presumably reactive lesions, although recurrences occasionally occur.")
30
Atypical decubital fibroplasia/ishemic fasciitis Differential diagnosis:
1)Well-differentiated liposarcoma: Atypical cells within fat but differs by having a zonated pattern, necrosis, and smudged degenerate nuclei rather than well-preserved malignant ones. 2) Malignant fibrous histiocytoma:Differs by its overall low cellularity and zonation.
Well-differentiated liposarcoma: Atypical cells within fat but differs by having a zonated pattern, necrosis, and smudged degenerate nuclei rather than well-preserved malignant ones. 2) Malignant fibrous histiocytoma:Differs by its overall low cellularity and zonation.")
31
Case 4 Biopsy from a 3 cm paratesticular mass in a 3 year old boy. The lesion, at operation, was poorly marginated

35
What’s your diagnosis?

36
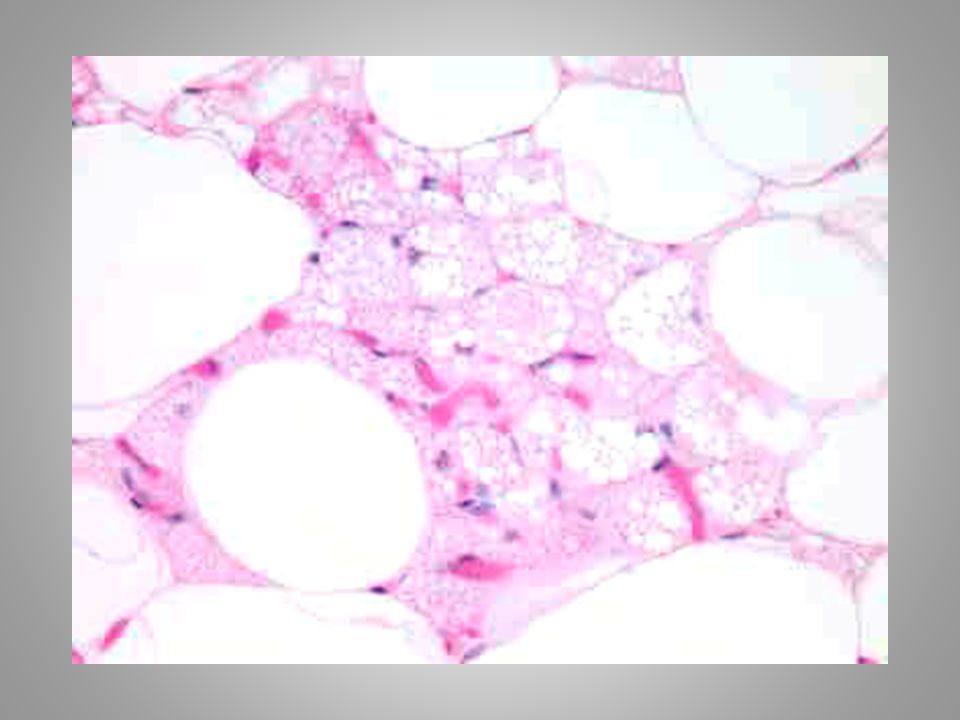
Fibrous hamartoma of infancy

37
Fibrous hamartoma of infancy
A tumorlike condition occure almost exclusively during the first 2 years of life M>F The most common sites:shoulder,axilla,upper arm The"common less common" site is the genital region, resulting in a clinical impression of lymphadenopathy or rhabdomyosarcoma Almost always solitary Gross:poorly circumscribed,whitish tissue of fibrous appearance with islands of fat

38
Fibrous hamartoma of infancy
Displays three components: A) Adipose tissue, some of which has tiny cytoplasmic droplets in keeping with brown fat. B)Haphazardly placed paucicellular fascicles of spindle cells with abundant collagen. C)Primitive-appearing rounded to spindled cells set in pale amphophilic stroma. There is no necrosis and mitoses are not identified.
 Adipose tissue, some of which has tiny cytoplasmic droplets in keeping with brown fat. B)Haphazardly placed paucicellular fascicles of spindle cells with abundant collagen. C)Primitive-appearing rounded to spindled cells set in pale amphophilic stroma. There is no necrosis and mitoses are not identified.")
39
Fibrous hamartoma of infancy Differential diagnosis:
1)Rhabdomyosarcoma: Rhabdomyosarcomas are not triphhasic and feature mitotic activity and more impressive cytologic atypia. IHC of fibrous hamartoma of infancy:the paucicellular bands are actin(+),desmin(-). The primitive-appearing cells are immunohistochemically "inert" with muscle marker. IHC of Rhabdomyosarcomas :focal desmin(+) and MyoD1 or myogenin(nuclear +), although the latter has been reported in some myofibroblastic lesions in abstract form 2) dedifferentiated liposarcoma :these are high grade sarcomas, usually of the retroperitoneum of older adults, featuring well-differentiated liposarcoma and juxtaposed high grade pleomorphic sarcoma
Rhabdomyosarcoma: Rhabdomyosarcomas are not triphhasic and feature mitotic activity and more impressive cytologic atypia. IHC of fibrous hamartoma of infancy:the paucicellular bands are actin(+),desmin(-). The primitive-appearing cells are immunohistochemically inert with muscle marker. IHC of Rhabdomyosarcomas :focal desmin(+) and MyoD1 or myogenin(nuclear +), although the latter has been reported in some myofibroblastic lesions in abstract form. 2) dedifferentiated liposarcoma :these are high grade sarcomas, usually of the retroperitoneum of older adults, featuring well-differentiated liposarcoma and juxtaposed high grade pleomorphic sarcoma.")
40
23 year old man with thigh mass
Case 5 23 year old man with thigh mass

45
What’s your diagnosis?

46
Mesenchymal chondrosarcoma

47
Mesenchymal chondrosarcoma
About two thirds arise in bone and the remainder in soft tissue. In skeletal sites, the mandible, rib, pelvic bones, and femur are the most common sites The extraskeletal examples presented in lower extremities followed by the meninges. Most lesions present in the second and third decades of life.

48
Mesenchymal chondrosarcoma
Histologic features :"small round cells" with scant cytoplasm arranged around hemangiopericytoma-like vasculature and punctuated by islands of mature-appearing cartilage. Reticulin staining encloses small groups of cells IHC:CD99(in the small cell component),S100(in the cartilaginous component),focal positivity for Actin,Desmin,Myogenin,NSE The extracellular matrix contains type II Collagen(diagnostic)
,S100(in the cartilaginous component),focal positivity for Actin,Desmin,Myogenin,NSE. The extracellular matrix contains type II Collagen(diagnostic)")
49
THE END

50
THANKS FOR YOUR ATTENTION

Similar presentations




















>")






>")




