Download presentation
Presentation is loading. Please wait.

1
Public health basis of screening
Anuj Mundra

2
Framework Definition Difference between screening and diagnosis.
Aims of screening Criteria for screening Types of screening Bias in screening Designing and evaluating a screening programme.

3
Definition Presumptive identification of unrecognized disease or defect by application of tests, examinations, or other procedures that can be applied rapidly. (U.S. Commission on chronic illness, 1957) A preventive care function (secondary prevention) It however differs from periodic health examination in the following respects- Wider application, Relatively inexpensive,
 A preventive care function (secondary prevention) It however differs from periodic health examination in the following respects- Wider application, Relatively inexpensive,")
4
What is screening

5
Difference between screening and diagnostic tests:
Screening tests Diagnostic tests 1. Done on apparently healthy population to detect potential cases or indicators. Done on those with signs of a disease to establish presence or absence of disease. 2. Applied to a community or group of people Applied to individuals 3. Based on one criterion or cut-off point Based on evaluation of a number of evidences like symptoms, signs, and investigations. 4. Generally less accurate and relatively less expensive More accurate but also more expensive 5. Not a basis of treatment Forms a basis to initiate treatment 6. Initiative comes from the investigator Initiative comes from a patient. 7. Simple, acceptable to patients and staff May be invasive and cumbersome 8. Generally chosen towards high sensitivity not to miss potential disease Chosen towards high specificity

6
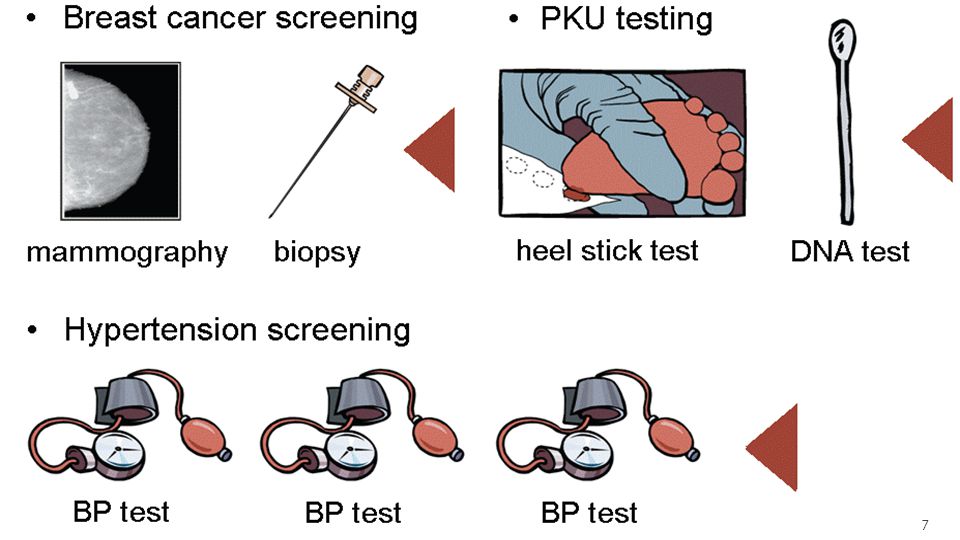
Aim of screening To sort out those with disease or at risk of having one from an apparently healthy population and bring them under medical supervision and treatment, thus helping in controlling the disease Screening can also be done for risk factors e.g. Screening for high BP as a risk for stroke Screening for cholesterol levels as a risk factor for cardiovascular diseases. Technical procedure like radio diagnosis or lab tests not necessary always, but simple procedures like BP assessment and certain criteria like MAST or CAGE can be also be successfully used for screening

8
Conceptual framework relating screening at individual setting and community levels

9
Criteria for screening:
Wilson and Jungner classic screening criteria, WHO 1968 The condition should be an important health problem There should be an accepted treatment for patients with recognized disease. Facilities for diagnosis and treatment should be available. There should be a recognisable latent or early symptomatic stage. There should be a suitable test or examination. The test should be acceptable to the population. The natural history of the condition, including development from latent to declared disease, should be adequately understood. There should be an agreed policy on whom to treat as patients. The cost of case-finding (including diagnosis and treatment) should be balanced in relation to possible expenditure on medical care as a whole. Case-finding should be a continuing process and not a 'once and for all' project.
 should be balanced in relation to possible expenditure on medical care as a whole. Case-finding should be a continuing process and not a once and for all project.")
10
Additional emerging screening criteria proposed over the past years
The screening programme should respond to a recognized need. The objectives of screening should be defined at the outset. There should be a defined target population. There should be scientific evidence of screening programme effectiveness. The programme should integrate education, testing, clinical services and programme management. There should be quality assurance, with mechanisms to minimize potential risks. The programme should ensure informed choice, confidentiality and respect for autonomy. The programme should promote equity and access to screening for the entire target population. Programme evaluation should be planned from the outset. The overall benefits of screening should outweigh the harm.

11
Points to focus Is it an important health problem?
The disease Is it an important health problem? Is the natural history well understood? Is there a recognizable latent or early symptomatic stage? Does early intervention improve the clinical/ public health outcome? Screening test Is the test valid? Is the test simple, reliable and affordable? Is the test acceptable to the patient and staff? Diagnosis and treatment Are the diagnostic facilities easily accessible? Is the treatment accessible and effective ? Is the overall programme cost-effective and sustainable? Does the benefit outweigh the harms from the programme?

12
What makes a disease appropriate for screening?
Disease burden Should be significant in terms of prevalence, morbidity or mortality. A disease with less severe burden is likely to waste resources.

13
What makes a disease appropriate for screening?
2. Natural history of disease and detectable preclinical phase-

14
What makes a disease appropriate for screening?
2. Natural history of disease and detectable preclinical phase- Helps to decide precisely when a screening test should be applied. In its absence, the screening would not find many undiagnosed cases. If the detectable stage does not come early before the critical point the treatment would not offer much benefit. When untreated, the disease should progress to a clinical disease phase.

15
What makes a disease appropriate for screening?
3. Availability of diagnostic and treatment facilities Any screening should be followed by diagnostic tests. Mere diagnosis is likely to just increase distress. The disease should be treatable or modifiable by early intervention in terms of improved survival and fewer long term problems than late treatment. It should also be ensured that adequate facilities and access to further diagnosis and treatment is available.

16
What makes a test suitable for screening?
For a test to be suitable for screening, it should be Acceptable Reliable Valid Cost-effective Offer a good yield of cases. Safe Simple Provide rapid results

17
1. Acceptability Should not be painful or embarrassing e.g. PR exam, biopsy Should expose to minimum hazards like radiation. Impact of test results or even being labelled at risk for the disease e.g. stigma of HIV, fear of cancer

18
2. Reliability Ability of a test to produce consistent results when repeated on the same individual in similar conditions. Also called as repeatability/ precision/ reproducibility. Depends on- Observer variation: Common in interpretation of X-rays, ECG, BP etc. Can be minimized by standardization of procedures, intensive training, repeat measurements etc. These errors can however, not be eliminated completely. It is of 2 types Intra-observer variation Inter-observer variation : measured by agreement, Kappa statistics Biological variation: due to physiological alterations e.g. BP, RBS Technical errors: defective instruments, faulty calibrations or reagents etc.

19
Measuring inter-observer variation
Percent agreement: Percent agreement= (A+D)/(A+B+C+D) Clearly negative individuals are usually high, thus increasing the agreement. It may be affected by knowledge, practice, training , and chance. Observer 2 Observer 1 Positive Negative A B C D
/(A+B+C+D) Clearly negative individuals are usually high, thus increasing the agreement. It may be affected by knowledge, practice, training , and chance. Observer 2. Observer 1. Positive. Negative. A. B. C. D.")
20
Reliability The total variation in results is cumulative of all sources A test with a wide range of results is less reliable than a test with a narrow range of results.

21
3. Validity Closeness with which the measured value agrees with the true value. It is also called as Accuracy. Determines whether a test is good enough to be used in screening for a particular disease. Validity of a test is measured by its sensitivity and specificity. Disease No disease Test positive True positives (a) False positives (b) Test positives (a+b) PV+ = a/(a+b) Test negative False negatives (c) True negatives (d) Test negatives (c+d) PV- = d/(c+d) Total diseased (a+c) Non-diseased (b+d) Total screened (a+b+c+d) Sensitivity= a/(a+c) Specificity= d/(b+d)
 False positives (b) Test positives (a+b) PV+ = a/(a+b) Test negative. False negatives (c) True negatives (d) Test negatives (c+d) PV- = d/(c+d) Total diseased (a+c) Non-diseased (b+d) Total screened (a+b+c+d) Sensitivity= a/(a+c) Specificity= d/(b+d)")
23
Validity Sensitivity: Ability of a test to detect all those with the disease in the screened population. Sensitivity= true positives/ (true positives + false negatives) Specificity: Ability of a test to identify correctly those free of the disease in the screened population Specificity= true negatives/ (true negatives + false positives) Ideal screening test– 100% sensitivity and specificity. Generally a test with high sensitivity is chosen for screening. Both sensitivity and specificity are inherent properties of a test. Cut-off values of tests can affect sensitivity and specificity High cut-off – low sensitivity but high specificity Low cut-off – high sensitivity but low specificity
 Specificity: Ability of a test to identify correctly those free of the disease in the screened population. Specificity= true negatives/ (true negatives + false positives) Ideal screening test– 100% sensitivity and specificity. Generally a test with high sensitivity is chosen for screening. Both sensitivity and specificity are inherent properties of a test. Cut-off values of tests can affect sensitivity and specificity. High cut-off – low sensitivity but high specificity. Low cut-off – high sensitivity but low specificity.")
26
Receptor operator characteristic (ROC) curve:
Graphical display of the how the proportions of true positives and false positives change for each of the possible pre-determined value. Distance from diagonal and area under the curve (AUROC) determines accuracy. AUROC ranges from 0 to 1. 1= perfect test 0.5= no diagnostic capability Uses: Shows the trade off between sensitivity and specificity. To set a cut-off value for a test result. To compare the performance of different tests measuring the same outcome. Cannot be used for a dichotomous variable
 determines accuracy. AUROC ranges from 0 to 1. 1= perfect test. 0.5= no diagnostic capability. Uses: Shows the trade off between sensitivity and specificity. To set a cut-off value for a test result. To compare the performance of different tests measuring the same outcome. Cannot be used for a dichotomous variable.")
27
Receptor operator characteristic (ROC) curve:
Blood sugar level (mg/dl) Sensitivity (%) Specificity (%) 70 98.6 8.8 80 97.1 25.5 90 94.3 47.6 100 88.6 69.8 110 85.7 84.1 120 71.4 92.5 130 64.3 96.9 140 57.1 99.4 150 50.0 99.6 160 47.1 99.8 170 42.9 180 38.6 sensitivity
 Sensitivity (%) Specificity (%) sensitivity.")
28
Predictive values Proportion of individuals having the disease or free of it from those detected as positive or negative by the test respectively. Does not affect the validity of test rather depends on its sensitivity and specificity. Not an inherent property as depends on the prevalence of disease in the screened population. Helps in determining the population to be screened, test to be utilized and cost-effectiveness. It is of 2 types: Predictive value of a positive test (PPV) Predictive value of a negative test (NPV)
 Predictive value of a negative test (NPV)")
29
Predictive value of a positive test
Also called as positive predictive value (PPV). Proportion of people actually having the disease among all those who have tested positive on the test i.e. “If one tests positive on screening, what are the chances that he really has the disease?” PPV= true positives/ (true positives + false positives) also, 𝑃𝑃𝑉= 𝑆𝑒𝑛𝑠𝑖𝑡𝑖𝑣𝑖𝑡𝑦 ∗ 𝑃𝑟𝑒𝑣𝑎𝑙𝑒𝑛𝑐𝑒 𝑆𝑒𝑛𝑠𝑖𝑡𝑖𝑣𝑖𝑡𝑦∗𝑃𝑟𝑒𝑣𝑎𝑙𝑒𝑛𝑐𝑒 + 1−𝑆𝑝𝑒𝑐𝑖𝑓𝑖𝑐𝑖𝑡𝑦 (1−𝑃𝑟𝑒𝑣𝑎𝑙𝑒𝑛𝑐𝑒) PPV cost-effectiveness Bayems theorem of conditional probability
. Proportion of people actually having the disease among all those who have tested positive on the test i.e. If one tests positive on screening, what are the chances that he really has the disease PPV= true positives/ (true positives + false positives) also, 𝑃𝑃𝑉= 𝑆𝑒𝑛𝑠𝑖𝑡𝑖𝑣𝑖𝑡𝑦 ∗ 𝑃𝑟𝑒𝑣𝑎𝑙𝑒𝑛𝑐𝑒 𝑆𝑒𝑛𝑠𝑖𝑡𝑖𝑣𝑖𝑡𝑦∗𝑃𝑟𝑒𝑣𝑎𝑙𝑒𝑛𝑐𝑒 + 1−𝑆𝑝𝑒𝑐𝑖𝑓𝑖𝑐𝑖𝑡𝑦 (1−𝑃𝑟𝑒𝑣𝑎𝑙𝑒𝑛𝑐𝑒) PPV cost-effectiveness. Bayems theorem of conditional probability.")
30
Predictive value of a negative test
Proportion of people free of disease among all those who have tested negative on the test i.e. “If one tests negative on screening, what are the chances that he is actually free of disease?” NPV= true negatives/ (true negatives+ false negatives) also, N𝑃𝑉= 𝑆𝑝𝑒𝑐𝑖𝑓𝑖𝑐𝑖𝑡𝑦 ∗ 1−𝑃𝑟𝑒𝑣𝑎𝑙𝑒𝑛𝑐𝑒 𝑆𝑝𝑒𝑐𝑖𝑓𝑖𝑐𝑖𝑡𝑦 1−𝑃𝑟𝑒𝑣𝑎𝑙𝑒𝑛𝑐𝑒 +(1−𝑆𝑒𝑛𝑠𝑖𝑡𝑖𝑣𝑖𝑡𝑦)𝑃𝑟𝑒𝑣𝑎𝑙𝑒𝑛𝑐𝑒 Makes people understand that negative test does not guarantee disease free condition. Limited role in decision making.
 also, N𝑃𝑉= 𝑆𝑝𝑒𝑐𝑖𝑓𝑖𝑐𝑖𝑡𝑦 ∗ 1−𝑃𝑟𝑒𝑣𝑎𝑙𝑒𝑛𝑐𝑒 𝑆𝑝𝑒𝑐𝑖𝑓𝑖𝑐𝑖𝑡𝑦 1−𝑃𝑟𝑒𝑣𝑎𝑙𝑒𝑛𝑐𝑒 +(1−𝑆𝑒𝑛𝑠𝑖𝑡𝑖𝑣𝑖𝑡𝑦)𝑃𝑟𝑒𝑣𝑎𝑙𝑒𝑛𝑐𝑒. Makes people understand that negative test does not guarantee disease free condition. Limited role in decision making.")
31
Likelihood ratios How much a test result will change the odds of having the disease. Used to describe the performance of a test. LR+ infers how much the odds of disease increase when a test is +ve LR+ = TP/FP or sensitivity/ (1-specificity) LR– infers how much the odds of disease decrease when a test is -ve LR- = FN/ TN or (1-sensitivity)/ specificity Pre-test odds = prevalence / (1-prevalence) Pre-test odds x likelihood ratio = post-test odds Post-test probability = post-test odds/(1+post-test odds)
 LR– infers how much the odds of disease decrease when a test is -ve. LR- = FN/ TN or (1-sensitivity)/ specificity. Pre-test odds = prevalence / (1-prevalence) Pre-test odds x likelihood ratio = post-test odds. Post-test probability = post-test odds/(1+post-test odds)")
32
Likelihood ratios Interpretation: the further away from 1, the stronger the evidence for presence or absence of a disease. LR > 1 – associated with presence of a disease LR < 1 – associated with absence of a disease. Represents results of a test as degree of abnormality rather than mere presence or absence Difficult to calculate as it requires conversion from probability to odds and back.

33
4. Cost-effectiveness Includes cost of entire follow up process.
Includes financial and non-financial costs (time, labour, convenience) to the patients as well as health personnel. Improvement is subject to improving validity and predictive values thereby reducing overdiagnosis and overtreatment. Important in guiding policy decisions.
 to the patients as well as health personnel. Improvement is subject to improving validity and predictive values thereby reducing overdiagnosis and overtreatment. Important in guiding policy decisions.")
34
5. Yield Amount of previously unrecognized disease diagnosed by screening. Depends on sensitivity, specificity and prevalence. A screening in high risk population usually leads to a higher yield of cases.

35
6. Safe , simple and rapid A screening test should be safe and not expose individuals to any hazards e.g. radiation, toxic drugs. A test should be simple enough to be carried out with minimal resources, paramedical or if possible non-medical personnel e.g. rapid HIV tests, mental heath screening by teachers at school. A rapid test will enable us in wider coverage, better acceptance and early initiation of therapy.

36
Types of screening Mass screening High risk or selective screening
Screening of a whole population or community irrespective of the risk. Increases programme sensitivity but less cost-effective. High risk or selective screening Applied selectively to high risk groups. More cost-effective but decreases programme sensitivity. Has a higher PPV.

37
Types of screening 3. Multiphasic screening
Application of 2 or more tests in combination. May be of 2 types Parallel/ simultaneous testing: Individuals go through all the tests at the same time. Patient is considered to have diseased if any of the tests is positive. This approach increases the sensitivity of a screening programme. Serial/ sequential testing: Individuals undergo the first test and if positive, will undergo the other test. Patient is considered diseased if all test results are positive. This approach tends to increase the specificity. However, there is lack of evidence of multiphasic screening having any additional benefit compared to the increases the cost and time consumed.

39
Net specificity= ( ) / 9500 = 98%
 / 9500 = 98%")
40
Bias in screening Referral/ volunteer bias Type of selection bias
People who volunteer to participate are more health conscious and compliant to advice – better prognosis. In certain cases like Ca breast, Ca ovaries the patient volunteer due to +ve family history – poor prognosis. Difficult to determine the direction of bias.

41
Length bias Also a type of selection bias Depends on type of diseases.
Relates to concept that screening selectively identifies cases with better prognosis.

42
Lead time bias Time between the actual detection of the disease by screening and its usual time of diagnosis in its absence. Illusion of better survival only because of earlier detection.

43
Overdiagnosis bias Due to overenthusiasm of people, tendency to misclassify (overdiagnose) non diseased as positive. A disease which would never have progressed to clinical stage or very late to have any significant effect in the lifetime or may have regressed on its own. Highly sensitive test with low specificity – ‘Aggressive screening’ Falsely increases the burden without any benefit

44
Ethics in screening A screening programme should guarantee improvement of general health of community with minimum risks or disadvantage Judicious use of limited resources especially in developing countries so as not to compromise other health needs. Informed consent. Psychological harm from false positives and unwarranted reassurance from false-negatives results.

45
Evaluation of screening programme
Operational measures Outcome measures # people screened Mortality reduction Proportion of target screened and # times Case-fatality rate reduction Percentage increase in cases detected early Detected prevalence Total cost of programme Complication reduction Cost per case found Prevention or reduction in recurrence Proportion of positive screenees brought to final diagnosis & T/t Improvement in quality of life. Predictive value of the test

46
Summary: Designing a screening programme
Disease to be screened- Burden, diagnostic workup, treatment facility. Screening test- validity, reliability and applicability. Determining the threshold/cut-off value – Higher cut-off gives specific but less sensitive test Lower cut-off gives sensitive but less specific test Determining the population–Entire population (low risk) or selective (high risk) group is to be taken. Counselling opportunities. Arrangements for confirmatory test and treatment. Evaluation of screening programme – Because of the deep-rooted belief that 'early diagnosis' of disease is beneficial, many regard screening as bound to be effective. However, for some reasons this is not the case always, thus necessitating evaluation of any screening intervention. The best study design to evaluate a screening programme is RCT. Although non-randomized trials, case control and cohort studies can also be used. For better evaluation mortality should be used as endpoint rather than survival. Referral bias, length bias, lead-time bias, and overdiagnosis bias. Regular follow-up screening sessions.
 or selective (high risk) group is to be taken. Counselling opportunities. Arrangements for confirmatory test and treatment. Evaluation of screening programme – Because of the deep-rooted belief that early diagnosis of disease is beneficial, many regard screening as bound to be effective. However, for some reasons this is not the case always, thus necessitating evaluation of any screening intervention. The best study design to evaluate a screening programme is RCT. Although non-randomized trials, case control and cohort studies can also be used. For better evaluation mortality should be used as endpoint rather than survival. Referral bias, length bias, lead-time bias, and overdiagnosis bias. Regular follow-up screening sessions.")
47
Screening for breast cancer
The screening procedures for breast examination are- Breast examination – self, clinical Mammography Mammography has very less benefits over breast examination. 40-69 50-69 20% mortality reduction (only 1/1000 women more) 17% mortality reduction More screens with more false +ve Lesser screens with lesser false +ve Increasing screening to 79 yrs decreases deaths by 8% than till 69 Increasing screening to 79 yrs decreases deaths by 7% than till 69
 17% mortality reduction. More screens with more false +ve. Lesser screens with lesser false +ve. Increasing screening to 79 yrs decreases deaths by 8% than till 69. Increasing screening to 79 yrs decreases deaths by 7% than till 69.")
48
Screening for cervical cancer
Screening programmes in Europe and Canada recommend cervical cytology starting at 25 till 64yrs at 3yrs interval (13 tests overall) In some countries yearly cytology from 20 yrs (overall 45 tests), thus increasing the burden. reduction in cumulative incidence of invasive cervical cancer with different screening strategies Screening frequency Reduction in rate of invasive cancer (%) No. of tests required Yearly 61 30 2 yearly 15 3 yearly 60 10 5 yearly 55 6
 In some countries yearly cytology from 20 yrs (overall 45 tests), thus increasing the burden. reduction in cumulative incidence of invasive cervical cancer with different screening strategies. Screening frequency. Reduction in rate of invasive cancer (%) No. of tests required. Yearly yearly yearly yearly")
49
Screening for prostate cancer
Methods available: DRE (digital rectal examination) – less sensitive PSA (prostate specific examination) – very low specificity detecting many benign lesions. yearly screening for PSA- Risk of death without screening – 2.86% Risk of death with screening – 2.15% Risk of overdiagnosis – 3.3% Biennial screening- risk for death – 2.27% Overdiagnosis – 2.4%
 – less sensitive. PSA (prostate specific examination) – very low specificity detecting many benign lesions. yearly screening for PSA- Risk of death without screening – 2.86% Risk of death with screening – 2.15% Risk of overdiagnosis – 3.3% Biennial screening- risk for death – 2.27% Overdiagnosis – 2.4%")
50
References Gordis L. Gordis: Epidemiology. 4th ed. Philadelphia: Saunders Elsevier; 2008. K.park. Parks text book of preventive and social medicine. 22nd ed. Jabalpur: M/s Banarasidas Bhanot; 2013. Andermann A, Blancquaert I, Beauchamp S, Déry V. WHO | Revisiting Wilson and Jungner in the genomic age: a review of screening criteria over the past 40 years. Bull World Health Organ [Internet]. World Health Organization; 2008;86(4). Available from: Ruf M, Morgan O. Diagnosis and screening. Pubic health textbook. 1st ed. Public Health Action Support Team; 2011. Miller AB, Goel V. Screening. In: Detels R, McEwen J, Beaglehole R, Tanaka H, editors. Oxford Text Book of Public Health. 4th ed. Oxford University Press; 2002. Rothman KJ, Greenland S, Lash TL. Modern Epidemiology. 3rd ed. Philadelphia: Lippincott Williams & Wilkins; 2008. Wilson J, Jungner G. Principles and practice of screening for disease. Geneva: World Health Organization; 1968. Fletcher RH, Fletcher SW, Wagner EH. Clinical Epidemiology: The Essentials. 3rd ed. Satterfield TS, editor. Pennsylvania: Williams & Wilkins; 1996. Mandelblatt JS, Cronin KA, Bailey S, Berry DA, de Koning HJ, Draisma G, et al. Effects of mammography screening under different screening schedules: model estimates of potential benefits and harms. Ann Intern Med Nov 17;151(10):738–47. Gulati R, Gore JL, Etzioni R. Comparative effectiveness of alternative prostate-specific antigen--based prostate cancer screening strategies: model estimates of potential benefits and harms. Ann Intern Med Feb 5;158(3):145–53.
. Available from: Ruf M, Morgan O. Diagnosis and screening. Pubic health textbook. 1st ed. Public Health Action Support Team; Miller AB, Goel V. Screening. In: Detels R, McEwen J, Beaglehole R, Tanaka H, editors. Oxford Text Book of Public Health. 4th ed. Oxford University Press; Rothman KJ, Greenland S, Lash TL. Modern Epidemiology. 3rd ed. Philadelphia: Lippincott Williams & Wilkins; Wilson J, Jungner G. Principles and practice of screening for disease. Geneva: World Health Organization; Fletcher RH, Fletcher SW, Wagner EH. Clinical Epidemiology: The Essentials. 3rd ed. Satterfield TS, editor. Pennsylvania: Williams & Wilkins; Mandelblatt JS, Cronin KA, Bailey S, Berry DA, de Koning HJ, Draisma G, et al. Effects of mammography screening under different screening schedules: model estimates of potential benefits and harms. Ann Intern Med Nov 17;151(10):738–47. Gulati R, Gore JL, Etzioni R. Comparative effectiveness of alternative prostate-specific antigen--based prostate cancer screening strategies: model estimates of potential benefits and harms. Ann Intern Med Feb 5;158(3):145–53.")
Similar presentations




, and the other of people with the same general characteristics.>")


 بسم الله الرحمن الرحيم.>")






, MPH(BPKIHS)>")








