Download presentation
Presentation is loading. Please wait.

1
Tailoring Reduced-Intensity Conditioning:
Applying Emerging Evidence to Clinical Practice February 4, 2012 12:15-1:15 pm

2
Marcos J. de Lima, MD Professor of Medicine
Department of Stem Cell Transplantation and Cellular Therapy M.D. Anderson Cancer Center Houston, TX

3
Faculty Disclosures Marcos J. de Lima, MD Research Grant – Celgene
Professor of Medicine Department of Stem Cell Transplantation and Cellular Therapy M.D. Anderson Cancer Center Houston, TX Research Grant – Celgene Kaci Wilhelm, PharmD Clinical Pharmacy Specialist Blood and Marrow Transplant No relevant financial relationships to disclose

4
Agenda 12:15-12:45 p.m. 12:45-1:05 p.m. 1:05-1:15 p.m.
Critical Decisions: Pretransplant Conditioning - Marcos J. de Lima, MD 12:45-1:05 p.m. Putting the Evidence into Practice: Optimized Dosing and Administration of Reduced-Intensity Conditioning Regimens - Kaci Wilhelm, PharmD 1:05-1:15 p.m. Faculty Panel: Questions & Answers

5
Critical Decisions: Pretransplant Conditioning
Marcos J. de Lima, MD M.D. Anderson Cancer Center Houston, TX

6
Discussion Topics Historic perspective and definitions
Donor and recipient-related covariates that influence transplant outcomes and regimen choice Myeloablative versus reduced intensity regimens – can we really compare them ? Donor – recipient issues that influence regimen choice We may not need to reduce dose intensity for all patients in the 6th and 7th decade of life Conclusions

7
Goal of Preparative Regimen
Immunosuppression - adequate to prevent rejection Cytoreduction - eradicate or control malignancy (this element not needed if disease is controlled by prior therapy) Stem cell space (not myelosuppression) - allow donor cells to compete effectively
 Stem cell space (not myelosuppression) - allow donor cells to compete effectively.")
8
05/22/11 06/09/11 07/06/11 Probability of overall survival after transplantation with acute leukemia in relapse or primary induction failure according to risk score (ie, [A] acute myeloid leukemia score of 0, 1, 2, and ≥ 3; [B] acute lymphoblastic leukemia score of 0 and 1; 2; and ≥ 3).The 3-year survival rates and 95% CIs are indicated. 08/04/11
.The 3-year survival rates and 95% CIs are indicated. 08/04/11.")
9
How did we get here? 1922, Fabricious-Moeller
Shielding of legs of guinea pigs during TBI decreased myelosuppression. 1952, Jacobsen/Lorenz Protection of TBI aplasia by injection of spleen cells from syngeneic mice. 1956, Nowell/van Bekkum/Ford/Tausche Concept of radiation chimera.

10
Head of a Lion, the Mid-section of a Goat and
the Hindquarters of a Dragon 10

11
BMT Landmarks 1955, Barnes and Loutit 1958, Santos
Carcinoma bearing mice exposed to lethal TBI with syngeneic spleen cell transplantation had long lived protection, but 50% of mice receiving allogeneic spleen cells died before day 100 without tumors. GVL and GVHD. 1958, Santos Lymphocytes (T-cells) mediate GVHD, and target organs are lymphoid, skin, gut, and liver.
 mediate GVHD, and target organs are lymphoid, skin, gut, and liver.")
12
1996

13
Two-year Probability of Treatment-related Mortality
After Transplants for CML, 20 40 60 80 100 < 20 years 20 – 40 years > 40 years 62% 53% PROBABILITY, % 41% 38% 27% 17% 11% 11% 9% HLA-ident Sib Unrelated Auto Leukemia TOS00_13.ppt

14
1990’s: How to improve treatment-related mortality and morbidity?
Improvements in supportive care, antibiotics, blood support, etc. Decrease the dose ?

15
Graft-vs-Malignancy Allogeneic SCT
Much of the benefit of alloSCT is due to immune GVL effect; therefore maximally ablative therapy may not be needed. Lower dose nonmyeloablative preparative regimens may be sufficient to prevent rejection. It was hypothesized that a reduced intensity, nonmyeloablative allogeneic transplant could reduce toxicity and allow successful treatment of older patients and those with major comorbidities.

16
ASH-Orlando 1996 MDACC Hadassah Seattle

17
Graft-Versus-Tumor Effect Graft-Versus-Host Disease

18
Graft-versus-Lymphoma Effect

19
Graft-versus-Leukemia Effect (GVL)
Intrinsic disease susceptibility is different. Some diseases need more chemo / radiation dose intensity than others.

20
Graft-versus-Leukemia Effect (GVL)
Low grade lymphomas, chronic myeloid and lymphocytic leukemias. + + Myelodysplastic syndrome and acute myelogenous leukemia. + Acute lymphocytic leukemia.

21
Histocompatibility Intensity

22
Review Question: Regarding the graft-versus-leukemia effect, it is true that:
Donor neutrophils are the effector cells. Chronic myelogenous leukemia is more sensitive to the graft-versus-leukemia effect than acute lymphoctye leukemia. It is not influenced by the use of systemic steroids. It is rarely associated with graft-versus-host disease.

23
Review Question: Regarding the graft-versus-leukemia effect, it is true that:
Donor neutrophils are the effector cells. Chronic myelogenous leukemia is more sensitive to the graft-versus-leukemia effect than acute lymphoctye leukemia. It is not influenced by the use of systemic steroids. It is rarely associated with graft-versus-host disease.

24
Definitions Myeloablative Profound pancytopenia within 1-3 weeks Irreversible myelosuppression Require stem cell support Reduced-Intensity Significant and prolonged cytopenias Reduction in alkylating agent or TBI dose Non-Myeloablative Minimal cytopenias Autologous recovery within 28 days Reduction is dose by about 30%. Bacigalupo A, et al. Biol Blood and Marrow Transplant 2009. 24

25
Myeloablative Dosing Thresholds
CIBMTR Operational Definitions TBI > 5Gy single dose TBI > 8Gy fractionated Busulfan > 9mg/kg PO Melphalan > 150mg/m2 Thiotepa > 10mg/kg Total dose per course 1mg/kg PO = 0.8mg/kg IV = 32mg/m2 IV Total dose per course Busulfan equivalent dosing: 7.2mg/kg IV or 288mg/m2 Giralt S, et al. Biol Blood Marrow Transplant 2009; Madden T, et al. Biol Blood Marrow Transplant 2007. 25

26
Graft-facilitating cells
Engraftment Graft Host Stem cell dose T-cell dose Graft-facilitating cells Stromal stem cells? Immunosuppression Preparative Regimen Post transplant Rx Disease effects Sensitization Histocompatibility

27
Patient-related Variables
Age Comorbidities Performance Status CMV Status Other Infections

28
Hematopoietic Cell Transplantation-Comorbidity Index (HCT-CI) for Non-Relapse Mortality (NRM) and Survival after Allogeneic HCT Sorror M and Collaborators Fred Hutchinson Cancer Research Center, Seattle, WA and MD Anderson Cancer Center, Houston, TX

29
Diagnosis is AML in First Remission - Individual Comorbidities
% of patients Lung Liver Cancer Cardiac Obesity Infection DM Psych Rheum

30
2-year NRM Stratified by HCT-CI Scores
FHCRC MDACC Percent NRM 37 19 27 7 21 7 Years after HCT

31
Two-year Survival Stratified by HCT-CI Scores
FHCRC MDACC Percent survival Years after HCT

32
• Genetics • Social economic issues • Access to treatment
Race • Genetics • Social economic issues • Access to treatment

33
Disease-related Variables

35
Disease-related Variables
Previous treatment(s) Marrow microenvironment Susceptibility to the GVL effect Disease tempo
 Marrow microenvironment. Susceptibility to the GVL effect. Disease tempo.")
36
Donor-related Variables

37
Donor-related Variables
- Donor-recipient ABO compatibility - CMV - Parity - Age (??) - Availability - Co-morbid conditions
 - Availability - Co-morbid conditions.")
38
The Graft

39
Graft Several institutional and/or investigator biases.
Donor choice (marrow versus PBPC). PBPC may be a better choice with reduced intensity preparative regimens. De novo chronic GVHD with PBPC is a serious problem. ASH 2011: results of randomized PBPC versus marrow in unrelated donor transplants.
. PBPC may be a better choice with reduced intensity preparative regimens. De novo chronic GVHD with PBPC is a serious problem. ASH 2011: results of randomized PBPC versus marrow in unrelated donor transplants.")
40
Donor Type Matched Sibling versus Unrelated

41
Donor Type Cord Blood versus Unrelated Marrow or Peripheral Blood Stem Cell

42
Effect of Graft Source on Unrelated Donor
Haemopoietic Stem-Cell Transplantation in Adults with Acute Leukemia: A Retrospective Analysis N= transplanted between 2002 – 2006 UCB = 165 PBPC = 888 Bone marrow = 472 All myeloablative Diagnoses: AML and ALL Eapen et al. Lancet Oncol 2010.

43
Probability of Leukemia-Free Survival for Patients
IN REMISSION NOT IN REMISSION Eapen et al. Lancet Oncol 2010.

44
Donor-recipient Variables

45
65-year Old Patient with AML

46
Donor Recipient HLA-A* 02:01:01 03:01:01g HLA-B* 35:03:01 51:08
HLA-Cw* 04:CXBM 16:02 HLA-DRB1* 11:01 13:02:01 HLA-DRB3* 02:02:01 03:01 HLA-DQB1* 03:01:01 06:04:01 (03:22, 06:39) HLA-DPB1* 02:01:02 09:01 01:01:01g 02:01:01 35:03:01 51:08 04:CXBM 16:02 11:01 13:02:01 02:02:01 03:01 03:01:01 06:04:01 (03:22, 06:39) 02:01:02 04:01:01
 HLA-DPB1* 02:01:02. 09:01. 01:01:01g. 02:01:01. 35:03:01. 51:08. 04:CXBM. 16:02. 11:01. 13:02:01. 02:02:01. 03:01. 03:01:01. 06:04:01. (03:22, 06:39) 02:01:02. 04:01:01.")
47
Anti HLA Antibodies Anti B13, B27, B38, B39, B41, B45, B49, B50,
DR7, DR9, DR53, DQ2, DQ8, DP1, DP11, DP13, DP15, DP17, DPB1*02:02 The patient's serum has reactivity against HLA-DPB1*09:01 (827 MFI).
.")
49
Are we transplanting older patients ?

50
Unrelated Donor Transplants at MDACC
Are we there yet? NO!! Median age of AML Patients: mid 60’s. MDS: mid 70 - late 70’s

51
Trends in Allogeneic Transplantation by Recipient Age,* 1987-2007
Transplants, percent Slides 5 & 6: The numbers of autologous and allogeneic HCTs for treatment of the most common malignant disease indications in patients older than 60 continue to increase. Thirty-two percent of autograft recipients and 10% of allograft recipients in were older than 60 years of age. The majority of autograft recipients (65%) are older than 50 years in this later period. * Transplants for AML, ALL, CML, MM, NHL, CLL, MDS
 are older than 50 years in this later period. * Transplants for AML, ALL, CML, MM, NHL, CLL, MDS.")
52
Reduced Intensity (RIC) or Non-Myeloablative (NMA) HCT CIBMTR Data
Years ≥ 40 years old or greater Matched related or unrelated donor MDS or AML in CR1 1,080 cases 545 AML CR1 535 MDS Data from 148 centers McClune, et al. Blood 2008;112 (11):135a (Abstract #346)
:135a (Abstract #346)")
53
TRM and Relapse of Patients 40+ Years Receiving Nonmyeloablative Allogeneic HSCT for AML and MDS, , by Age 1 3 4 100 20 40 60 80 90 10 30 50 70 2 Years 1 3 4 100 20 40 60 80 90 10 30 50 70 2 TRM Relapse 65+ yrs 60-64 yrs 55-59 yrs 40-54 yrs 60-64 yrs 55-59 yrs 40-54 yrs 65+ yrs p=0.66 p=0.87 Years McClune, et al. Blood 2008;112 (11):135a (Abstract #346) Tp08_10.ppt
:135a (Abstract #346) Tp08_10.ppt.")
54
Does the intensity of the preparative regimen matter?
It does – however, it is not the same for all diseases. It depends on the diagnosis and the sensitivity to the graft versus malignancy effect

55
Are there diseases in which reducing the intensity may be worse than otherwise? A cautionary tale in AML and MDS. It is not only the regimen: stem cell source etc etc.

56
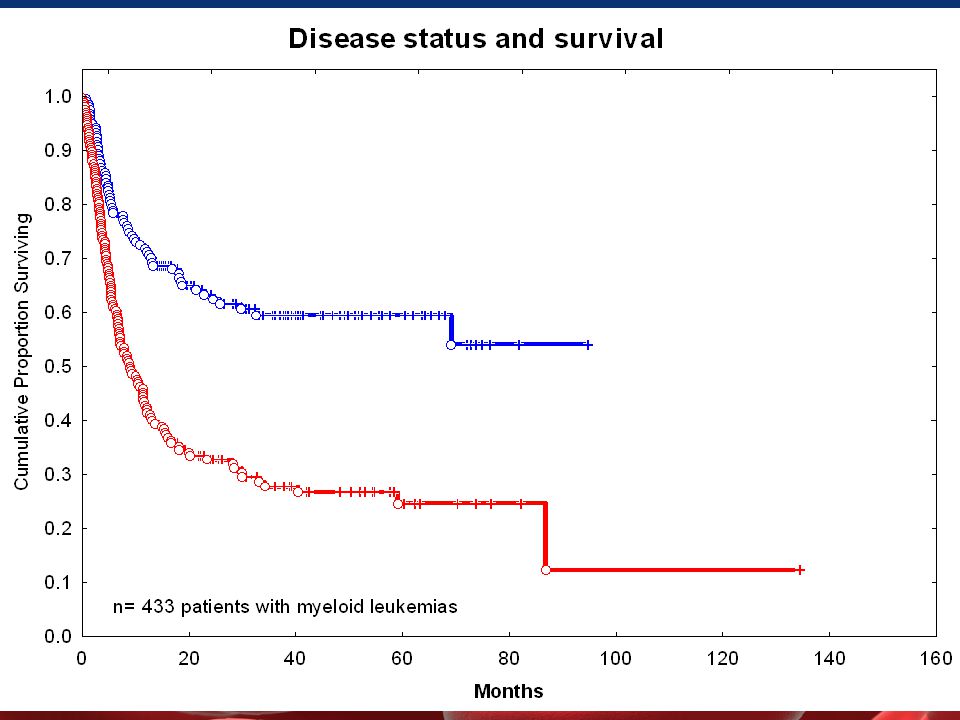
Effect of Regimen Intensity on Transplant Outcome for AML/MDS
FAI - relapse FAI - toxicity De Lima et al Blood 2004

57
Comparing RIC vs MA Caveats
Notable absence of prospective RIC vs MA conditioning studies…. Level of evidence is not the highest Retrospective & Registry Studies Selection Bias RIC (vs MA) Graft Source More likely PBSC GVHD prophylaxis More likely CNI + MMF Co-morbidity Score Worse Previous Transplant More likely Baseline different when you compare PARAMESWARAN HARI
 Graft Source More likely PBSC. GVHD prophylaxis More likely CNI + MMF. Co-morbidity Score Worse. Previous Transplant More likely. Baseline different when you compare. PARAMESWARAN HARI.")
58
Review Question: Which of the following statements is true?
Aging does not influence results of allogeneic stem cell transplantation. Remission status at transplant influences treatment-related mortality. There is extensive literature comparing outcomes of myeloablative and reduced-intensity preparative regimens in a randomized fashion. Most patients with myelodysplastic syndrome receive allogeneic transplants.

59
Review Question: Which of the following statements is true?
Aging does not influence results of allogeneic stem cell transplantation. Remission status at transplant influences treatment-related mortality. There is extensive literature comparing outcomes of myeloablative and reduced-intensity preparative regimens in a randomized fashion. Most patients with myelodysplastic syndrome receive allogeneic transplants.

60
100-day Mortality after Allogeneic Transplantation, 1998-2008 - by conditioning intensity -
NO Slides 5 & 6: The numbers of autologous and allogeneic HCTs in patients older than 50 continue to increase. Sixty-two percent of autograft recipients and 35% of allograft recipients in were older than 50 years of age. Early mortality has improved for allogeneic transplants in general. Patient selection is key !!

61
Adjusted Probability of Overall Survival
100 20 40 60 80 90 10 30 50 70 NST vs Myeloablative, p<0.01 NST vs RIC PB, p=0.02 RIC PB (N = 768) Adjusted Probability, % Myeloablative (N = 3,731) NST (N = 407) RIC BM (N = 273) 1 2 3 4 5 Years Wsp08_18.ppt 61
 Adjusted Probability, % Myeloablative (N = 3,731) NST (N = 407) RIC BM (N = 273) Years. Wsp08_18.ppt. 61.")
62
Are there situations in which reduced-intensity transplants have changed the standard of care for transplant?

63
Ablative Allo-BMT in Indolent Lymphoma
Probability, % 5 4 3 2 1 20 40 60 80 100 6 Survival DFS Treatment-related mortality Relapse Years van Besien et al. Blood. 1998;92:

64
NON-MYELOABLATIVE ALLOGENEIC SCT
Conditioning Regimen Rituximab Fludarabine 30 mg/m2 Rituximab 375 mg/m2 Cyclophosphamide 750 mg/m mg/m2 ASCT Days ATG 15 mg/kg daily, was given days –5 to –3 for mismatched or unrelated SCT. Tacrolimus and methotrexate were used for GVHD prophylaxis.

65
FCR Allo SCT for Low Grade Lymphoma
Khouri et al Blood 2008

66
Conditioning Regimen Intensity by Histology Allogeneic Transplants for Lymphoma in North America
FOLLICULAR Transplants MANTLE HODGKIN Slides 5 & 6: The numbers of autologous and allogeneic HCTs in patients older than 50 continue to increase. Sixty-two percent of autograft recipients and 35% of allograft recipients in were older than 50 years of age. Graft vs. Lymphoma effect if any , varies by histology Armand et al. Biol BMT 2008;14:418-25

67
BMT CTN Clinical Trials of Reduced Intensity Allogeneic Transplantation
BMT CTN – Bone Marrow Transplant Clinical Trials Network Study # Disease Study Question BMT CTN 0102 Myeloma Tandem Auto vs. Auto -> Allo RIC HCT BMT CTN 0202 Foll. NHL Autologous vs. Matched Sib Allo RIC HCT BMT CTN 0502 AML CR1 RIC Allo HCT in pts 60 – 74 yrs BMT CTN 0601 Sickle Cell RIC URD HCT BMT CTN 0603 Many Haplo identical HCT with RIC BMT CTN 0604 Double Cord HCT with RIC BMT CTN 0701 Sibling or URD HCT with RIC BMT CTN 0901 MDS/AML Myeloablative vs. RIC Allogeneic HCT

68
Ablative Regimens Are Improving As Well!!

69
Intravenous Busulfan/Fludarabine
Day Bu 130 mg/m2 q d Flu * rest* rest* HSCT 40 mg/m2 q d GVHD prophylaxis: tacrolimus and “mini” methotrexate *day of ATG if MUD or one-antigen mismatched related donor Fludarabine is given as a 60 min infusion once daily for 4 days, each dose immediately followed by IV Busulfan 130 mg/m2 over 3 hours by pump. Borje Andersson

70
Myeloablative IV Busulfan and Fludarabine
for Patients Older Than 54 years Years n=74 Related or unrelated donors (50% / 50%) Age ≥ 55 years (median, 58 years; range, years) Cytogenetics : poor (27%); intermediate (68%); good (5%) Complete remission at transplant (54%) Diagnosis: AML (81%) / MDS (19%) Al-Atrash et al. Blood : Abstract 2999.
 Age ≥ 55 years (median, 58 years; range, years) Cytogenetics : poor (27%); intermediate (68%); good (5%) Complete remission at transplant (54%) Diagnosis: AML (81%) / MDS (19%) Al-Atrash et al. Blood : Abstract")
71
Myeloablative IV Busulfan and Fludarabine for Patients Older Than 54 Years
Cumulative Incidence Treatment-related Mortality Grade II-IV Acute GVHD Al-Atrash et al. Blood : Abstract 2999

72
Myeloablative IV Busulfan and Fludarabine
for Patients Older Than 54 Years Al-Atrash et al. Blood : Abstract 2999

73
Reduced-intensity Conditioning
Use has increased over the last decade. There are no randomized comparisons of regimen intensity - it is a matter of convictions, egos, tradition, careers, and institutional data and experience. Little controversy: older patients and patients with medical comorbidities.

74
Conditioning Regimen Intensity: (some) Take Home Messages
Age does not influence outcomes with RIC/NMA for AML, up to age 65 (+/-!!). HCT with RIC/NMA offers a possibility to cure AML in the elderly in up to % of patients (you can’t myeloablate most patients in the late 60’s and early 70’s!!). Usual prognostic factors do apply (ie cytogenetics etc). Disease status at transplant is the most important predictor for post transplant outcome.
. HCT with RIC/NMA offers a possibility to cure AML in the elderly in up to % of patients (you can’t myeloablate most patients in the late 60’s and early 70’s!!). Usual prognostic factors do apply (ie cytogenetics etc). Disease status at transplant is the most important predictor for post transplant outcome.")
75
Review Question: Given that reduced-intensity regimens are usually associated with lower treatment-related mortality, it is true that: All patients with acute myelogenous leukemia should receive this type of regimen. All patients with myelodysplastic syndrome should receive this type of regimen. There is frequently a tradeoff between less treatment-related mortality and higher relapse rate. Disease susceptibility to the graft-versus-leukemia is the same for all hematologic malignancies.

76
Review Question: Given that reduced-intensity regimens are usually associated with lower treatment-related mortality, it is true that: All patients with acute myelogenous leukemia should receive this type of regimen. All patients with myelodysplastic syndrome should receive this type of regimen. There is frequently a tradeoff between less treatment-related mortality and higher relapse rate. Disease susceptibility to the graft-versus-leukemia is the same for all hematologic malignancies.

77
To Ablate or Not… Patients with some indolent diseases have more to lose with a high-risk approach upfront (especially now with new medications!): - CML in chronic phase that is refractory to imatinib and other TKI but remain in chronic phase. - Low grade lymphoma. - CLL. - Low grade MDS. - Multiple myeloma
: - CML in chronic phase that is refractory to imatinib and other TKI but remain in chronic phase. - Low grade lymphoma. - CLL. - Low grade MDS. - Multiple myeloma.")
78
To Ablate or Not… In the absence of controlled trials RIC regimens should be considered standard for: Hodgkin’s Disease Myeloma Older patients Heavily pretreated patients or those with significant co-morbidities Most patients with CLL and NHL

79
Future Directions Better definition of risk for treatment-related mortality. Incorporation of new agents. Better integration with standard treatment. Conjugation with graft engineering and post transplant pharmacologic and immunologic manipulations.

80
Conclusions The major contribution is the realization that patients in the 7th and 8th decades of life can have allogeneic transplants. Major obstacles to cure are delayed or poor immune recovery, graft-versus-host disease and disease relapse. Relapse rates are higher than in myeloablative transplants for certain diseases.

81
To ablate or Not, That Is the Question…
Controlled trials are needed to establish whether RIC is superior to conventional allografting or standard therapy in most hematologic malignancies. These trials will need to be performed in single diseases and selected disease stages to be clinically informative. The issue of preparative regimen of choice is unresolved.

82
Acknowledgments Edwin P. Alyea III, MD Dana Farber Institute
Brenda Sandmaier, MD Fred Hutch – Seattle Marcelo Pasquini, MD Parameswaran Hari, MD CIBMTR Sergio Giralt, MD - NY

83
Department of Stem Cell Transplantation M D Anderson Cancer Center
Richard Champlin Borje Andersson Elizabeth Shpall Roy Jones Stefan Ciurea Simrit Parmar Jeffrey Molldrem Uday Popat Paolo Anderlini Partow Kebriaei Yago Nieto Issa Khouri Chitra Hosing Martin Korbling Michael Andreef Qaiser Bashir Image Credit: NASA/JPL/Space Science Institute

Similar presentations


 Overview Willis H Navarro, MD Medical Director, Transplant Services, NMDP Associate Clinical Professor,>")


 Medical Director Cancer Transplant Institute Virginia G. Piper Cancer Center Everything You Ever Wanted to Know About Transplant.>")




 Covenant Health System HSCT Program Lubbock, Texas April 4, 2007.>")

 in Patients with Secondary Myelodysplastic Syndromes (sMDS) Enrolled in the AVIDA Registry 1 Prospective Trial.>")


 ◦ Greenberg P et al. International scoring system for evaluating prognosis in myelodysplastic.>")



![5-Azacitidine For Myelodysplasia Before Allogeneic Hematopoietic Cell Transplantation Field T et al. Bone Marrow Transplant 2009:[Epub ahead of print].](/33/8174862/big_thumb.jpg "5-Azacitidine For Myelodysplasia Before Allogeneic Hematopoietic Cell Transplantation Field T et al. Bone Marrow Transplant 2009:[Epub ahead of print].>")