Download presentation
Presentation is loading. Please wait.

1
Minimal invasive surgery for pancreatic insulinoma: Current evidence
Dr. HO Man-fung Prince of Wales Hospital

2
CURRENT TREATMENT

3
Medical therapy Dietary modification Diazoxide Somatostatin analogue
Minimal effect on disease progression (especially for non-responder) Pre-operative symptoms control 60% response rate only…
 Pre-operative symptoms control. 60% response rate only…")
4
Surgery Surgery is the Mainstay of treatment for insulinoma
Curative (local disease / limited liver metastasis) Symptomatic control in metastastic disease Enucleation Distal pancreatectomy +/- splenectomy Pancreaticoduodenectomy Central / total pancreatectomy Resection of liver metastasis
 Symptomatic control in metastastic disease. Enucleation. Distal pancreatectomy +/- splenectomy. Pancreaticoduodenectomy. Central / total pancreatectomy. Resection of liver metastasis.")
5
Special concerns of insulinoma
Small size < 2cm in ~ 80% Difficulty in localization 90% benign and solitary Resection strategy Room for minimal invasive surgery Overt symptoms, poorly controlled by drugs Pre-operative control of symptoms Even palliative resection in metastatic disease wound be beneficial

6
Surgical approach Pre-operative localization IOUS
Enucleation or Pancreatectomy ? Blind distal pancreatectomy

7
Lo et al. Surgical Endoscopy (2004) 18: 297-302
60% with CT, 80% with EUS, 100% with THPVS K. Ravi et al. Ann R Coll Surg Engl 2007; 89: 67% (incl. USG, CT, MRI, THPVS) Mehrdad Nikfarjam et al. Annals of Surgery • Volume 247, Number 1, January 2008 29-80% with non invasive investigation, % with invasive investigations
 Mehrdad Nikfarjam et al. Annals of Surgery • Volume 247, Number 1, January % with non invasive investigation, % with invasive investigations.")
8
Surgical approach Pre-operative localization IOUS
Enucleation or Pancreatectomy ? Blind distal pancreatectomy

9
IOUS being the most sensitive test among all investigations of choice
Ref: A Fuller Understanding of Pancreatic Neuroendocrine Tumours Combined with Aggressive Management Improves Outcome. S.L.Ong et al. Pancreatology 2009;9:583–600

10
Amelia C. Grover et al. A prospective evaluation of laparoscopic exploration with intraoperative ultrasound as a technique for localizing sporadic insulinomas. Surgery 2005; 138:1003-8

11
See the difficulties? Ref: The American association of endocrine surgeons.Pancreatic neuroendocrine tumors: insulinoma

12
Surgical approach Pre-operative localization IOUS
Enucleation or Pancreatectomy ? Blind distal pancreatectomy

13
Enucleation Pancreatectomy Solitary lesion Size < 2cm
Away from major vessels / pancreatic ducts Pancreatectomy Multifocal lesions Size > 2cm Close to major vessels / pancreatic ducts MEN 1

14
Ref: L. Fernandez-Cruz et al
Ref: L.Fernandez-Cruz et al. Is laparoscopic ressection adequate in patients with neuroendocrine pancreatic tumour. World Journal of Surgery (2008) 32:
 32:")
15
Surgical approach Pre-operative localization IOUS
Enucleation or Pancreatectomy ? Blind distal pancreatectomy

16
? Blind resection 4/61 persistent symptoms despite resection
Further resection jeopadized parachymal preservation (90% benign) Importance of pre-operative localization Portal venous sampling (~100% localization) Ref: Improved Contemporary Surgical Management of Insulinomas. A 25-year Experience at the Massachusetts General Hospital. Mehrdad Nikfarjam et al. Annals of Surgery • Volume 247, Number 1, January 2008
 Importance of pre-operative localization. Portal venous sampling (~100% localization) Ref: Improved Contemporary Surgical Management of Insulinomas. A 25-year Experience at the Massachusetts General Hospital. Mehrdad Nikfarjam et al. Annals of Surgery • Volume 247, Number 1, January")
17
K. Ravi et al. Ann R Coll Surg Engl 2007; 89: 212-217.

18
Management of liver metastasis
Resection Transarterial chemoembolization Ablation Systemic chemotherapy Targeted therapy(e.g. Sunitinib, everolimus) Liver transplantation
 Liver transplantation.")
19
MINIMAL INVASIVE SURGERY
Inapproapiate large wound for small benign tumours Going through evidence of lapasroscopic treatment. Lack of RCT due to scarcity of case MINIMAL INVASIVE SURGERY

20
Lapasroscpic pancreatic resection
1st laparoscopic pancreatic resection -1992 Gagner M et al (1996). J Gastrointest Surg 1: 20-26 Cushieri A. et al (1996). Ann Surg 223: 1st laparoscopic resection of insulinoma – 1992 Low incidence and difficult anatomical location, laparoscopic experience published relatively late compared to other laparoscopic surgery
. J Gastrointest Surg 1: Cushieri A. et al (1996). Ann Surg 223: st laparoscopic resection of insulinoma – Low incidence and difficult anatomical location, laparoscopic experience published relatively late compared to other laparoscopic surgery.")
21
2 enucleations and 2 distal pancreatectomies done laparoscopically
100% pre-operative localization Only for lesions over body and tail 1 patient with post operative pancreatic leakage Pancreatic head tumour were traeted with open surgeries. 2004

22
1st comparative study of laparoscopic vs open approach (12 vs 9)
Comparison with historical cohort No significant difference in morbidty, mortality, intraoperative variables Only 1 patient used intra-operative USG Denied use of intra-operative USG to be necessary 2007

23
Laparoscopic USG Only way to replace palpation in laparoscopic surgery
Localization of lesion(s) Sensitivity 83-98%a Comparable to THPVS b Define anatomical relationship with major vessels, main pancreatic duct a) Mehrdad Nikfarjam et al . Improved Contemporary Surgical Management of Insulinomas. A 25-year Experience at the Massachusetts General Hospital.. Annals of Surgery • Volume 247, Number 1, January 2008 Amelia C. Grover et al. A prospective evaluation of laparoscopic exploration with intraoperative ultrasound as a technique for localizing sporadic insulinomas. Surgery 2005; 138:1003-8
 Sensitivity 83-98%a. Comparable to THPVS b. Define anatomical relationship with major vessels, main pancreatic duct. a) Mehrdad Nikfarjam et al . Improved Contemporary Surgical Management of Insulinomas. A 25-year Experience at the Massachusetts General Hospital.. Annals of Surgery • Volume 247, Number 1, January Amelia C. Grover et al. A prospective evaluation of laparoscopic exploration with intraoperative ultrasound as a technique for localizing sporadic insulinomas. Surgery 2005; 138:")
24
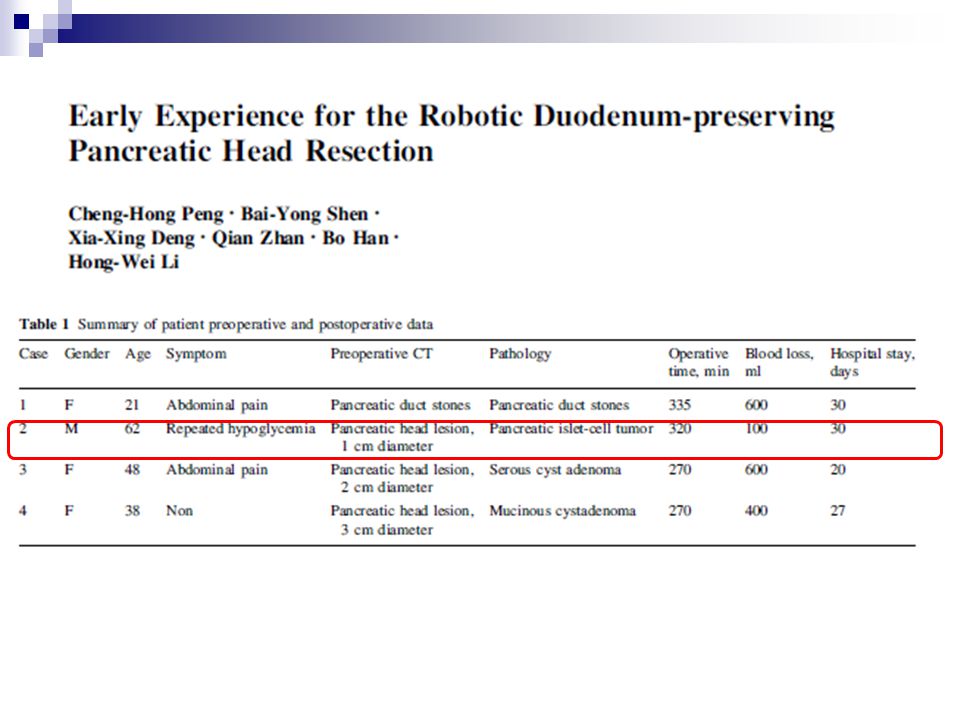
pNETs with pancreatic resection, 20 patients with insulinoma
Pre-op localization 100% 1/20 conversion to open Mean follow up of 36 months, no recurrence Significant less blood loss and operative time for laparoscopic enucleation Published in 2008: from Concerning the result of insulinoma only Converted to open due to failure to identify the lesion

25
Pre-operative localization - unknown 1/21 converted open
21 patients Pre-operative localization - unknown 1/21 converted open IOUS: localization, intraoperative decision, marking of transection line 3 patients with pancreatic fistula All except 1 discharged in 1 week No recurrence Convert due to previous pancreatitis resulted un dense adhesion 1 grade B fistula stayed 60 days

26
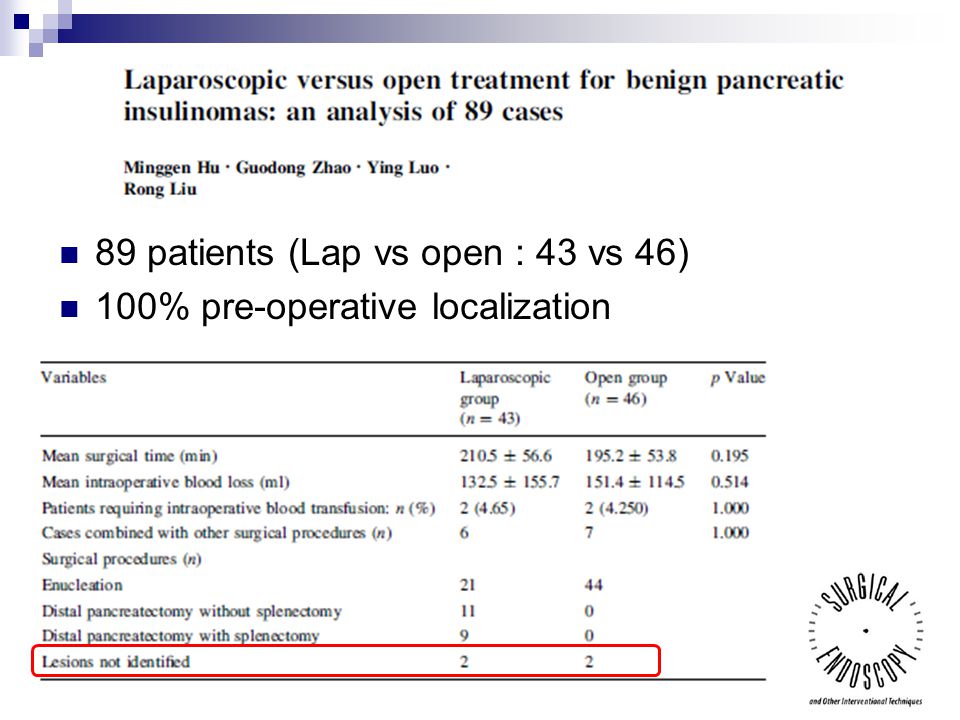
89 patients (Lap vs open : 43 vs 46) 100% pre-operative localization
27
No recurrence in 6 months
Only the 4 patients with tumour cannot located intra-operatively remain symptomatic (tumour not resected)
")
28
Distal pancreatectomy Enucleation Number of patients 85 496 101
Whipple’s operation Distal pancreatectomy Enucleation Number of patients 85 496 101 Mortality (%) 3.5 0.4 Mobidity (%) 30.7 34.1 47 Mean blood lost (ml) 126 311 - Conversion rate (%) 8.75 12.1 23.3 Mean operation time (min) 371 229 132 Mean hospital stay 13.6 7.5 7.8 Pancreatic fistula / intra-abdominal collection and respiratory complications are most common cause of morbidity Results for laparoscopic distal pancreatectomy is more favourable compared with open Lack of survival analysis
 Mobidity (%) Mean blood lost (ml) Conversion rate (%) Mean operation time (min) Mean hospital stay Pancreatic fistula / intra-abdominal collection and respiratory complications are most common cause of morbidity. Results for laparoscopic distal pancreatectomy is more favourable compared with open. Lack of survival analysis.")
29
Represent early experience
Highly selected cases Indicating minimal invasive surgery is feasible Pancreatic fistula is still the most prevalent complication Lacking of long term results, e.g. survival, recurrence Heterogeneous disease

30
Laparoscopic arm (LDP): 773 (43%) Open arm : 1041 (57%)
Total n= 1814 (18 studies) Laparoscopic arm (LDP): 773 (43%) Open arm : 1041 (57%) Conversion rate : 0 – 30% (not reported in 4 studies) Among all pancreatic surgery, laparoscopic distal pancreatectomy seen getting more attention than others
 Laparoscopic arm (LDP): 773 (43%) Open arm : 1041 (57%) Conversion rate : 0 – 30% (not reported in 4 studies) Among all pancreatic surgery, laparoscopic distal pancreatectomy seen getting more attention than others.")
31
Operative parameters: Blood loss

32
Post operative recovery: Length of stay

33
Post operative complications: pancreatic fistula

34
Laparoscopic distal pancreatectomy has the advantage of:
Lower blood loss Faster recovery Comparable complication profile with open approach This technique is a reasonable approach in selected cancer patients Also commented on oncological clearance with only positivity of resection margin (4 studies only) 4.5% vs 8.8%– Not adequate to draw conclusion 10 of 18 studies excluded cases of malignant lesion / invasive ductal carcinoma Results maybe applicable to patients with insulinoma, that laparoscopic surgery could have benefits
 4.5% vs 8.8%– Not adequate to draw conclusion. 10 of 18 studies excluded cases of malignant lesion / invasive ductal carcinoma. Results maybe applicable to patients with insulinoma, that laparoscopic surgery could have benefits.")
35
Most extensive experience in published literature are from USA, Italy and South Korea
Focused on distal pancreatectomy What about robots?

36
1st 30 cases in University of Pittsburgh
Compared with 94 patient with laparoscopic distal pancreatectomy 0% conversion rate 100% R0 resection Median LN harvest (Lap vs Robot = 9 vs 19) Similar tumour size
 Similar tumour size.")
37
Notice a high rate of planned splenic resection on this initial cohort

38
v Better visualization, freedom of movement, stability
Preservation of spleen and splenic vessels 21/22 patient with successful splenic preservation 17 patient with splenic vessels preserved 1 patient developed post op splenic infarct Further expand the advantage minimal invasive surgery by improving rate of spleen preservation DP with splenic preservation has been documented to increase hospital stay – mainly due to splenic complications Splenic infarct in 1 paitent with splenic vessles sacrifies. Managed conservatively Robot confers additional advantage for splenic preservation

40
Open vs Laparoscopic / robotic Whipple’s operation
Open vs Laparoscopic / robotic distal pancreatectomy Longer operative time Decreased blood lost Shorter hospital stay Similar complication profile Improved rate of R0 resection Inlcuded few series up to 40 patients comparing… with results of …

41
Robotic pancreatic surgery
Literature in its infancy Small cohort available even for high volume centres Case selection bias Learning curve Long term results ?

42
Local ablative therapy
Percutaneous RFA ablation Stephan Limer et al. European Journal of Gastroenterology and Hepatology 2009, 21: EUS Guided ablation of insulinoma: a new treatment option Michael J. Levy et al. gastrointestinal Endoscopy, Vol 75, No.1;

43
Conclusion Insulinoma is benign most of the time, but causing significant biochemical disturbance that require surgical treatment Localization is of utmost importance in surgical success Laparoscopic surgery offers treatment with less trauma and similar safety profile Novel treatment for surgically unfit individuals

44
Conclusion Insulinoma is an ideal entity for minimal invasive pancreatic surgery Lesion are small and benign most of the time no concern for involved margin, lymphatic dissection Laparoscopic and robotic pancreatic surgery is feasible for management of pancreatic insulinoma

46
INSULINOMA

47
Insulinoma Subgroup of pancreatic neuroendocrine tumours (pNETs)
Commonest functional pNETs (25%) Incidence : 4 in 1,000,000 Unsuppressed production of endogenous insulin As part of genetic syndromes (5-8%) MEN I, VHL, NF I, TS
 Incidence : 4 in 1,000,000. Unsuppressed production of endogenous insulin. As part of genetic syndromes (5-8%) MEN I, VHL, NF I, TS.")
48
Presentation Whipple’s triad: Weight gain Other related syndromes
Fasting hypoglycaemia (< 2.2 mmol/L) Symptomatic hypoglycaemia (autonomic and neuroglycaemic symptoms) Relieve of symptoms after administration of glucose Weight gain Other related syndromes
 Symptomatic hypoglycaemia (autonomic and neuroglycaemic symptoms) Relieve of symptoms after administration of glucose. Weight gain. Other related syndromes.")
49
Biochemical diagnosis
Ref: A Fuller Understanding of Pancreatic Neuroendocrine Tumours Combined with Aggressive Management Improves Outcome. S.L.Ong et al. Pancreatology 2009;9:583–600 To rule out other causes of hypoglycaemia

50
Localization Non-invasive Ultrasounography Computed tomography
Magnetic resonance imaging Somatostatin receptor scintigraphy

51
Localization Invasive Endoscopic ultrasound +/- FNAC
Selective arteriography Transhepatic portal venous sampling +/- calcium stimulation Surgical exploration + intra-operative US (IOUS) Endoscopic ultrasound +/- FNAC
 Endoscopic ultrasound +/- FNAC.")
52
Ref: A Fuller Understanding of Pancreatic Neuroendocrine Tumours Combined with Aggressive Management Improves Outcome. S.L.Ong et al. Pancreatology 2009;9:583–600

53
WHO classification Ref: A Fuller Understanding of Pancreatic Neuroendocrine Tumours Combined with Aggressive Management Improves Outcome. S.L.Ong et al. Pancreatology 2009;9:583–600

54
Ref: L. Fernandez-Cruz et al
Ref: L.Fernandez-Cruz et al. Is laparoscopic resection adequate in patients with neuroendocrine pancreatic tumour. World Journal of Surgery (2008) 32:
 32:")
Similar presentations







 for Liver Tumour Dr Dai Wing Chiu Queen Mary Hospital.>")












