Download presentation
Presentation is loading. Please wait.

1
Question What is the most common cause of failed reconstructions of the anterior cruciate ligament? Technical error Failure of graft incorporation Patient selection Significant reinjury Premature return to sport

2
Answer: L. Kroonen Though any of the given answers could cause graft failure, the cited article states that technical error is the leading cause % of failures are estimated to be caused by poorly placed tunnels. Anterior placement of the femoral tunnel is the most common error (when the resident stops at “resident’s ridge”). For the tibial side, the ideal placement is at the posteromedial portion of the ACL footprint, with the tunnel parallel and posterior to Blumensaat’s line. Failure of graft incorporation can be caused by avascularity, immunologic reactions or stress shielding from fixation devices. Allografts have been shown to incorporate less and over a longer time than autograft. Traumatic failure can be due to overly aggressive rehab or early return to sports, or a significant trauma to the knee after the graft has matured. Allen CR, Giffin JR, Harner CD: Revision anterior cruciate ligament reconstruction. Orthop Clin North Am 2003;34:79-98.
. For the tibial side, the ideal placement is at the posteromedial portion of the ACL footprint, with the tunnel parallel and posterior to Blumensaat’s line. Failure of graft incorporation can be caused by avascularity, immunologic reactions or stress shielding from fixation devices. Allografts have been shown to incorporate less and over a longer time than autograft. Traumatic failure can be due to overly aggressive rehab or early return to sports, or a significant trauma to the knee after the graft has matured. Allen CR, Giffin JR, Harner CD: Revision anterior cruciate ligament reconstruction. Orthop Clin North Am 2003;34:")
3
19. A patient who underwent anterior cruciate ligament reconstruction with a central one third bone-patellar-bone autograft 1 week ago now reports swelling of the right knee. Examination reveals that the patient is afebrile, has a large knee effusion, has limited range of motion, and cannot perform a straight leg raise. Radiographs show only routine postoperative changes. What is the next most appropriate step in management? 1 - Electrodiagnostic testing 2 - KT-2000 testing 3 - Compression dressing 4 - MRI 5 - Knee aspiration

4
Answer – M Harpe Joint effusion post ACL reconstruction occurs in about 12% of cases. In the early post-op period typically hemarthrosis is the cause. Late development typically arises from increased synovial fluid collection secondary to local inflammatory response. A severe effusion as in this patient’s case has been shown to cause inhibition of voluntary quadriceps contraction (ie. Noted inability to perform straight leg raise). Next best step in mgmt = #5 knee aspiration for both diagnostic and therapeutic purposes. This allows improved examination capability, decreases knee effusion related symptoms, and can be sent for lab analysis and culture to r/o infective association. #3 could be used as a supportive treatment option. #1,2 and 4 are not indicated based on circumstances provided. Mangrine/Noyes: Advanced weight bearing and range of motion after ACL reconstruction. Orthopedics 1992;15:
. Next best step in mgmt = #5 knee aspiration for both diagnostic and therapeutic purposes. This allows improved examination capability, decreases knee effusion related symptoms, and can be sent for lab analysis and culture to r/o infective association. #3 could be used as a supportive treatment option. #1,2 and 4 are not indicated based on circumstances provided. Mangrine/Noyes: Advanced weight bearing and range of motion after ACL reconstruction. Orthopedics 1992;15:")
5
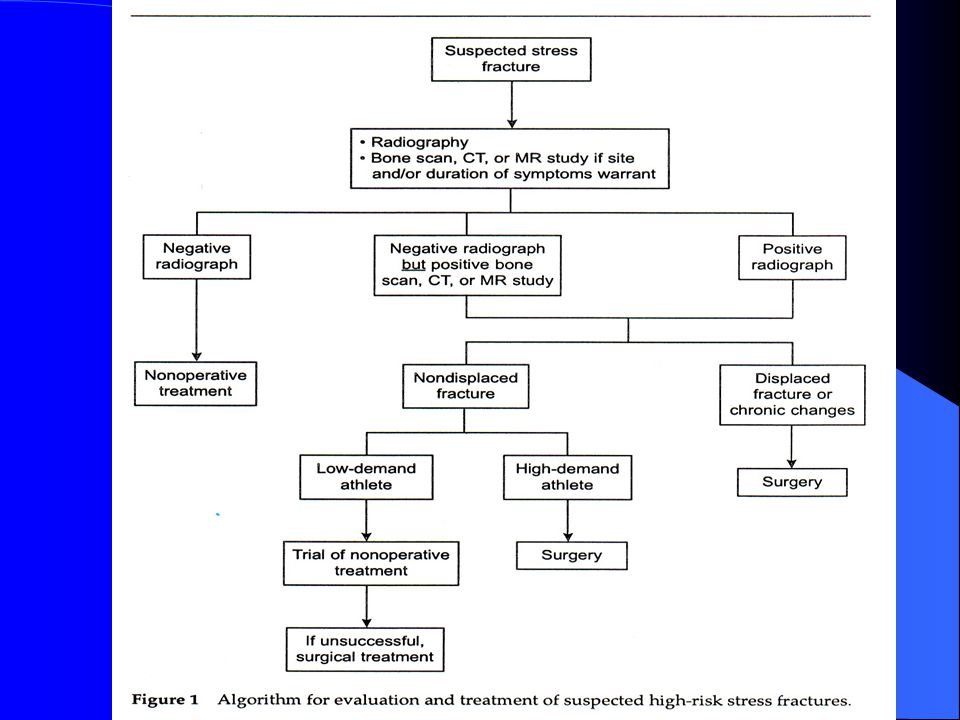
Joe Carney Question A 14 year old boy who is a cross-country runner reports a 6 week history of medial knee pain that has prevented him from training. Radiographs are normal. An MRI scan is shown in Figure 8. Management should consist of a knee brace home physical therapy followed by a return to running Protected weight bearing for 4 to 6 weeks Intramedullary rodding of the tibia referral to an orthopaedic oncologist

7
Answer: protected weight bearing for 4 to 6 weeks
In patients with clinically suspected stress-related injuries that are radiographically negative, bone scintigraphy is more sensitive than magnetic resonance imaging as the initial imaging modality (per Broden JAAOS Vol 8 No. 6). MR does have a higher specificity and in this question the STIR image shows changes related to stress fracture with a transverse incomplete cortical fracture visible. Attached is Broden’s suggested algorithm for evaluation and treatment of suspected stress fractures. Because the patient is not a high demand athlete and the fracture is negative on radiographs, nondisplaced, and without chronic changes. Broden suggests nonoperative treatment. Nonoperative treatment consists of 1 to 6 weeks of limited weightbearing progressing to full weightbearing. This is followed by a phase of low-impact activity and once this is tolerated over prolonged periods high-impact exercises may be initiated.
. MR does. have a higher specificity and in this question the STIR image shows. changes related to stress fracture with a transverse incomplete. cortical fracture visible. Attached is Broden’s suggested algorithm. for evaluation and treatment of suspected stress fractures. Because the patient is not a high demand athlete and the fracture is. negative on radiographs, nondisplaced, and without chronic changes. Broden suggests nonoperative treatment. Nonoperative treatment. consists of 1 to 6 weeks of limited weightbearing progressing to. full weightbearing. This is followed by a phase of low-impact activity. and once this is tolerated over prolonged periods high-impact. exercises may be initiated.")
9
Question 46 Which of the following findings is considered a predisposing factor for an acute lateral patellar dislocation? Hypoplastic medial femoral condyle Dysplastic Vastus lateralis Patella baja Decreased Q angle Excessive internal rotation of the femur

10
Answer: C Dewing Acute lateral patellar dislocation is far more common than medial dislocation and is associated with weak vastus medialis, patella alta, increased Q angle, and excessive internal rotation of the femur with external tibial rotation. Mechanisms described include indirect injury and direct blow. Anatomic studies show associated avulsion of the medial patellofemoral ligament (MPFL) which is in Layer II of the medial knee structures and runs from the medial femoral epicondyle to the medial patella and VMO. It contributes at least half of the static stabilization of the patella. Associated chondral injury to the patellofemoral joint is common and can be suggested by fat droplets in knee aspirate. Some advocate acute repair of the MPFL, but most treat acute dislocation with non-operative bracing and PT. Re-dislocation rates are as high as 40% in some studies, making this a difficult problem.
 which is in Layer II of the medial knee structures and runs from the medial femoral epicondyle to the medial patella and VMO. It contributes at least half of the static stabilization of the patella. Associated chondral injury to the patellofemoral joint is common and can be suggested by fat droplets in knee aspirate. Some advocate acute repair of the MPFL, but most treat acute dislocation with non-operative bracing and PT. Re-dislocation rates are as high as 40% in some studies, making this a difficult problem.")
11
Bharam S, Vharas MS, Fu FH: Knee fractures in the athlete
Bharam S, Vharas MS, Fu FH: Knee fractures in the athlete. Orthop Clin North Am 2002;33: Halbrecht JL, Jackson DW: Acute dislocation of the patella, in Fox JM, Delpizzo W (eds): The patellofemoral joint. NY, NY, McGraw Hill, 1993, p.123
: The patellofemoral joint. NY, NY, McGraw Hill, 1993, p.123.")
12
Question A 25-year-old man underwent an uneventful anterior cruciate ligament reconstruction with a bone-patella-bone autograft 4 months ago. Examination now reveals a painless knee, no effusion, and range of motion from 10º to 120º. Results of a Lachman’s test are negative, and patella mobility is excellent. What is the most common cause for the loss of motion? Loss of graft fixation Femoral tunnel drilled too vertical Anterior femoral tunnel placement Anterior tibial placement Posterior tibial tunnel placement

13
Answer: M. Robinson Loss of motion following ACL reconstruction include infection, swelling, poor compliance with physical therapy, RSD, immobilization, impingement, scarring or capsulitis , and poor surgical technique. This patient has both loss of flexion and extension. Impingement is the result of an actual physical block in the intercondylar notch that is caused by scarring, a cyclops lesion, and anteriorly placed tibial tunnel, or an inadequate notchplasty. Loss of graft fixation is not correct with a negative Lachman. Femoral tunnel drilled too vertical causes persistent rotational instability. Anterior femoral tunnel placement (most common technical error) causes loss of flexion if tensioned in extension or laxity in extension if tensioned in flexion. Posterior tibial tunnel placement will cause excessive graft laxity in flexion and excessive graft tension in flexion. Anterior tibial tunnel placement causes both excessive tension in flexion and extension. See attached chart. Allen CR, Giffin JR, Harner CD: Revision anterior cruciate ligament reconstruction. Orth Clin North Am 2003;34: Howell SM, Taylor MA: Failure of reconstruction of the anterior cruciate ligament due to impingement by the intercondylar roof. JBJS 1993;75:
 causes loss of flexion if tensioned in extension or laxity in extension if tensioned in flexion. Posterior tibial tunnel placement will cause excessive graft laxity in flexion and excessive graft tension in flexion. Anterior tibial tunnel placement causes both excessive tension in flexion and extension. See attached chart. Allen CR, Giffin JR, Harner CD: Revision anterior cruciate ligament reconstruction. Orth Clin North Am 2003;34:79-98 Howell SM, Taylor MA: Failure of reconstruction of the anterior cruciate ligament due to impingement by the intercondylar roof. JBJS 1993;75:")
14
ACLR Tunnel Placement Tight Anterior Posterior Tunnel Femur Flexion
Extension Tibia + Impingement

15
Question 68 A 12-year old boy sustains an injury to his knee while playing football. Examination reveals diffuse tenderness, a 2+ effusion, and restricted range of motion. He has 2+ laxity with valgus stress. Which of the following imaging studies will best aid in diagnosis? Bone scan MRI CT Bone age radiographs 5. AP and lateral radiographs with and without stress

16
Q 68 preferred response 5 Jim Harris
Based on hx, age and physical exam the issue here is MCL disruption vs. physeal fx. An argument can be made that MRI will answer this and tell us much more about all other soft tissue and bone structures of the knee. But gentle stress radiographs will adequately answer the acute clinical problem and are cheaper and faster than an MRI. Both cited sources recommend them. Perryman Orthop Clin North Am 2002 Garth Primary Care Orthopedics

17
Question A 42yo man has chronic anterior cruciate ligament-deficient knee. What variable has the greatest correlation with the future development of arthritis? 1- Patient age 2- Medial collateral ligament injury 3- Meniscal integrity 4- quadriceps atrophy of more than 25% compared with the opposite extremity 5- Isokinetic muscle deficit of more than 15% compared with the opposite extremity

18
Answer: 3- Meniscal Intregrity
Answer: 3- Meniscal Intregrity DTSchroder All excellent reviews on ACL deficient knees. The study cited by several of the references is a German multicenter trial of 328 patients with ACL injury with minimum of 15yrs f/u: that time from meniscectomy was the single strongest predictor in the ACL deficient knee for the development of OA. There has been some controversy as to the certainty of OA acceleration in the isolated chronic ACL deficient knee when evaluating some of the larger epidemiologic studies, with some suggesting worse OA with reconstruction. But there is little doubt from the literature the major impact of meniscectomy: the more resected, the worse the prognosis toward OA. When looking at pooled data from over 600 cases of chronic ACL deficiency, meniscal pathology approaches 83%(55% MMT, 12% LMT, and 16% combined). Overall, meniscal pathology is noted in 52% of acute ACL ruptures as well. Fairbanks first postulated the important role of the menisci but it was not until the late ’70’s and ’80’s that good studies not only determined meniscal function is important in the stability(not so much primary stabilization but secondary especially post horn of med meniscus), shock absorption/load transmission, and nutrition/lubrication, but the implications of meniscal damage in the face of ACL injury. Drongowski’s study showed no correlation with a bad outcome with meniscal pathology at 51months in 99/107 patients all treated nonoperatively, but f/u was by phone and no radiographic eval for OA changes made.
. Overall, meniscal pathology is noted in 52% of acute ACL ruptures as well. Fairbanks first postulated the important role of the menisci but it was not until the late ’70’s and ’80’s that good studies not only determined meniscal function is important in the stability(not so much primary stabilization but secondary especially post horn of med meniscus), shock absorption/load transmission, and nutrition/lubrication, but the implications of meniscal damage in the face of ACL injury. Drongowski’s study showed no correlation with a bad outcome with meniscal pathology at 51months in 99/107 patients all treated nonoperatively, but f/u was by phone and no radiographic eval for OA changes made.")
19
Caborn DN, Johnson BM: The natural history of the anterior cruciate ligament-deficient knee: A review. Clin sports Mmed 1993;12: (one of first reviews to link menical damage directly to OA) Clatworthy M, Amendola A: The anterior cruciate ligament and arthritis. Clin Sports Med 1999;18: (Most definitive review linking meniscal damage to OA) Drongowski RA, Coran AG, wojtys EM: Predictive value of meniscal and chondral injuries in conservatively treated anterior cruciate ligament injuries. Arthroscopy 1994;10: (Only nonreview article: suggests that functional outcome not affected by meniscal damage at index surgery)Thompson WO, Fu FH: The meniscus in the cruciate-deficient knee. Clin Sports Med 1993;12: (Biomechanical role of menisci)
 Clatworthy M, Amendola A: The anterior cruciate ligament and arthritis. Clin Sports Med 1999;18: (Most definitive review linking meniscal damage to OA) Drongowski RA, Coran AG, wojtys EM: Predictive value of meniscal and chondral injuries in conservatively treated anterior cruciate ligament injuries. Arthroscopy 1994;10: (Only nonreview article: suggests that functional outcome not affected by meniscal damage at index surgery)Thompson WO, Fu FH: The meniscus in the cruciate-deficient knee. Clin Sports Med 1993;12: (Biomechanical role of menisci).")
20
Question 99 Which of the following findings is typical in an acute burner injury (stinger)? 1. Isolated motor weakness 2. Lower extremity weakness 3. Ipsilateral motor and contralateral sensory symptoms 4. Bilateral arm symptoms 5. Unilateral arm symptoms

21
Preferred response – 5 Chuck Craven
“Burners syndrome” aka traumatic upper extremity paresthesia, occurs frequently in contact sports. Amongst college defensive players, this syndrome occured with a 65% career frequency in one study. The syndrome is so named b/c of the pain, burning, or tingling an athlete experiences. Burners are related to the position of the brachial plexus and cervical nerve roots and their vulnerability to trauma during contact sports. The athlete experiences immediate pain, burning, or tingling that originates in the neck and extends down the arm in a non-dermatomal pattern. Weakness may be seen in the deltoid, SS, IS, and biceps muscles – it may be immediate or delayed. Burners are a result of brachial plexus traction or compression (see diagram) at the intervertebral foramen.
 at the intervertebral foramen.")
22
Clancy’s article talks about “brachial plexus axonotmesis”, a more severe form of a burner; they randomly define this as motor weakness +/- sensory changes, lasting more than 2 weeks. In their study of 13 patients with this syndrome, all had axon degeneration involving the biceps, deltoid and spinati muscles on EMG. All but one patient recovered fully. The return to competition guidelines based on this data included 1) full recovery on EMG and 2) normal motor strength. REFERENCES: Koffler KM, Kelly JD IV: Neurovascular trauma in athletes. Orthop Clin North Am 2002; 33: Sallis RE, Jones K, Knopp W: Burner-offensive strategy for an under-reported injury. Physician Sports Med 1992;20:47-55. Clancy WG Jr, Brand RL, Bergfield JA: Upper trunk brachial plexus injuries in contact sports. Am J Sports Med 1977; 5:

24
105. A patient undergoes repair of an avulsion fracture of the fibular head and posterior cruciate ligament reconstruction. One day after surgery, physical therapy for muscle strengthening and knee range of motion should consist of 1 – active flexion and extension in all arcs. 2 – active flexion from 0 to 90 deg and active extension from 90 to 0 3 – active flexion from 0 to 90 deg and no active extension 4 – no active flexion and extension in all arcs. 5 – no active flexion and active extension from 90 to 0

25
Answer – Deleted? No answer given Carter Maurer The answer to this question is most likely 5 (no active flexion, active extension 90 – 0). PCL reconstruction and posterolateral repair rehabilitation is designed to restore ROM and prevent stressing the graft. Exercises that cause posterior tibial translation (active hamstrings) are prohibited for usually 12 weeks. This eliminates answers 1,2, and 3. Differentiating 4 and 5 are difficult due to poor grammar and differences in practice tendencies. Some surgeons maintain the knee in locked extension with isometric quad exercises for the first 3 weeks postop (this could be answer 4). Answer 4 could also be read as no ROM restrictions which is not correct and thus 5 should be the correct answer Chen FS, Rokito AS, Pitman MI: Acute and Chronic Posterolateral Rotatory Instability of the Knee. JAAOS 2000;8: Veltri DM, Warrren RF: Isolated and Combined Posterior Cruciate Ligament Injuries. JAAOS 1993;67-75.
. PCL reconstruction and posterolateral repair rehabilitation is designed to restore ROM and prevent stressing the graft. Exercises that cause posterior tibial translation (active hamstrings) are prohibited for usually 12 weeks. This eliminates answers 1,2, and 3. Differentiating 4 and 5 are difficult due to poor grammar and differences in practice tendencies. Some surgeons maintain the knee in locked extension with isometric quad exercises for the first 3 weeks postop (this could be answer 4). Answer 4 could also be read as no ROM restrictions which is not correct and thus 5 should be the correct answer. Chen FS, Rokito AS, Pitman MI: Acute and Chronic Posterolateral Rotatory Instability of the Knee. JAAOS 2000;8: Veltri DM, Warrren RF: Isolated and Combined Posterior Cruciate Ligament Injuries. JAAOS 1993;")
26
Question A 45-year-old man who sustained a twisting injury to his flexed right knee while playing ice hockey now is unable to bear weight. Examination reveals a small knee effusion, negative results on a Lachman’s test, increased lateral opening of 2 mm to 3 mm, and 4/5 ankle dorsiflexion strength. Radiographs are shown in figures 31a and 31b. What is the next best course of action? – Elastic compression bandage – Long leg cast MRI – Closed reduction – Open reduction

28
Answer: Josh Bell The xrays demonstrate a dislocation of the proximal tibiofibular joint. The xrays do not project well but you should be able to make that diagnosis. (If they give you knee xrays on the test and you don’t see anything look for the patella and the tib-fib joint). Once you have the diagnosis of a dislocation it is fairly simple that a closed reduction should be attempted next and if that is not achieved than an open reduction can be performed. The injury most commonly occurs with violent twisting actions which can occur in high speed crashes as well as parachute landings, wrestling and judo. Patients often complain of lateral knee pain. Injury to the meniscus and lateral structures may be included in the differential diagnosis. Once the diagnosis has been made an attempted reduction should be attempted. This is done under local anesthesia or conscious sedation. The knee is flexed to degrees to relax the lateral structures and a direct force is placed on the fibular head in the direction to relocate the joint. Some authors recommend eversion, dorsiflexion and external rotation of the foot to relax EHL, EDL and peroneals. Parkes JC II, Zelko RR: Isolated acute dislocation of the proximal tibiofibular joint. JBJS Am 1973;55: Sekiya JK, Kuhn JE: Instability of the proximal tibiofibular joint. JAAOS 2003:11:
. Once you have the diagnosis of a dislocation it is fairly simple that a closed reduction should be attempted next and if that is not achieved than an open reduction can be performed. The injury most commonly occurs with violent twisting actions which can occur in high speed crashes as well as parachute landings, wrestling and judo. Patients often complain of lateral knee pain. Injury to the meniscus and lateral structures may be included in the differential diagnosis. Once the diagnosis has been made an attempted reduction should be attempted. This is done under local anesthesia or conscious sedation. The knee is flexed to degrees to relax the lateral structures and a direct force is placed on the fibular head in the direction to relocate the joint. Some authors recommend eversion, dorsiflexion and external rotation of the foot to relax EHL, EDL and peroneals. Parkes JC II, Zelko RR: Isolated acute dislocation of the proximal tibiofibular joint. JBJS Am 1973;55: Sekiya JK, Kuhn JE: Instability of the proximal tibiofibular joint. JAAOS 2003:11:")
29
Question 148 A Patient who underwent anterior cruciate ligament (ACL) reconstruction 2 years ago now reports instability and medial joint line pain. Examination reveals varus instability and increased external rotation at 30 degrees of flexion. Results of Lachman’s and posterior drawer tests are negative. Radiographs show a mechanical axis of 11 degrees of varus, with spurring of the medial tibial plateau. What is the next most appropriate step in treatment? Revision ACL reconstruction and PCL reconstruction 2. Distal femoral osteotomy 3. Distal femoral osteotomy and PCL reconstruction 4. High tibial osteotomy 5. High tibial osteotomy and posterolateral reconstruction
 reconstruction 2 years ago now reports instability and medial joint line pain. Examination reveals varus instability and increased external rotation at 30 degrees of flexion. Results of Lachman’s and posterior drawer tests are negative. Radiographs show a mechanical axis of 11 degrees of varus, with spurring of the medial tibial plateau. What is the next most appropriate step in treatment Revision ACL reconstruction and PCL reconstruction. 2. Distal femoral osteotomy. 3. Distal femoral osteotomy and PCL reconstruction. 4. High tibial osteotomy. 5. High tibial osteotomy and posterolateral reconstruction.")
30
Answer: Jared Foran The posterolateral complex consists of the popliteus, the popliteofibular ligament, lateral capsule, arcuate ligament, and the fabellofibular ligment. Chronic Grade 3 posterolateral complex knee injuries are often seen in association with tears of the ACL and/or PCL. Unrecognized or untreated, these injuries are a major cause of reconstruction failures of both the ACL and PCL. Clues that we are dealing with a posterolateral complex injury are: 1. history of ACL injury/repair, 2. varus instability, 3. positive dial test (i.e., increased external rotation of tibia on femur in 30 degrees of flexion, 4. genu varus on radiograph. 5. spuring of medial tibial plateau. Although not mentioned in the question, the posterolateral drawer test, external rotation recurvatum, and reverse pivot shift test may also be positive Continued…

31
…answer to 148 (continued)
…answer to 148 (continued) Patients with genu varus and chronic grade 3 posterolateral rotatory instability usually need an osteotomy to return their mechanical axis to the lateral compartment prior to repairs/reconstructions of the posterolateral structures. Failure to perform an osteotomy is associated with a resulting varus thrust gait and stretching of the repaired tissues over time. Medial opening wedge proximal tibial osteotomy is perferred over lateral closing wedge proximal tibial osteotomy, so that the posterior capsule and oblique popliteal ligament complex can be tightened up. Following the osteotomy, the posterolateral complex repair is tailored to the patient’s deficits. If there is injury to the fibular head and associated structures, biceps tenodesis or allograft reconstruction is used in an attempt to reproduce the normal function of the FCL, popliteus/popliteofibular ligament complex, or to create a soft-tissue sling to inhibit varus opening or external rotation. Arent EA (Ed): OKU: Sports Mediine 2. Rosemont, IL, AAOS, 1999, pp Noyes FR, Munns SW, Andriacchi TP, Mayhall, MT: The double varus and triple varus anterior cruciate ligament insufficient knee: Gait analysis and surgical correction. Trans Am Orthop Soc Sports Med 1985; 11:41.
 Patients with genu varus and chronic grade 3 posterolateral rotatory instability usually need an osteotomy to return their mechanical axis to the lateral compartment prior to repairs/reconstructions of the posterolateral structures. Failure to perform an osteotomy is associated with a resulting varus thrust gait and stretching of the repaired tissues over time. Medial opening wedge proximal tibial osteotomy is perferred over lateral closing wedge proximal tibial osteotomy, so that the posterior capsule and oblique popliteal ligament complex can be tightened up. Following the osteotomy, the posterolateral complex repair is tailored to the patient’s deficits. If there is injury to the fibular head and associated structures, biceps tenodesis or allograft reconstruction is used in an attempt to reproduce the normal function of the FCL, popliteus/popliteofibular ligament complex, or to create a soft-tissue sling to inhibit varus opening or external rotation. Arent EA (Ed): OKU: Sports Mediine 2. Rosemont, IL, AAOS, 1999, pp Noyes FR, Munns SW, Andriacchi TP, Mayhall, MT: The double varus and triple varus anterior cruciate ligament insufficient knee: Gait analysis and surgical correction. Trans Am Orthop Soc Sports Med 1985; 11:41.")
32
Question 161 What pattern of arthritis develops following nonsurgical treatment of an isolated posterior cruciate ligament injury? Patellofemoral 2. Patellofemoral and medial 3. Patellofemoral and lateral Medial Lateral

33
Answer: 2 The purpose of the retrospective study by Strobel was to gain more information on the likelihood of developing cartilage lesions in posterior cruciate ligament (PCL)-deficient knees using arthroscopy records of 181 patients with a nonsurgically treated acute or chronic PCL injury. Their results showed that PCL insufficiency significantly increased the risk of developing medial femoral condyle and patellar cartilage degeneration over time. Of patients whose PCL deficiency was present for more than 5 years, 77.8% showed degenerative cartilage lesions of the medial femoral condyle and 46.7% showed cartilage degeneration of the patella. After 1 year of PCL insufficiency, the number of medial femoral cartilage lesions increased threefold (13.6% v 39.1%). With the presence of combined PCL/posterolateral insufficiency the amount of medial femoral degeneration was significantly increased (36.6% v 60.6%). Strobel MJ, Weiler A, Schulz MS, et al: Arthroscopic evaluation of articular cartilage lesions in posterior ligament deficient knees. Arthroscopy 2003;19: Ramesh M, O’Byrne JM, McCarthy N, Jarvis A, Mahalingham K, Cashman WF: Damage to the superior gluteal nerve after the Hardinge approach to the hip. J Bone Joint Surg Br 1996;78: Andrew Pennock

34
Question 165 A 13-year-old boy who plays football reports a 3-month history of medial knee pain that is increased with external rotation of the lower extremity. Knee radiographs are normal. What is the best course of action? Physical therapy 2. Medial collateral ligament brace 3. Three-phase bone scan 4. MRI of the knee AP and frog-lateral radiographs of the pelvis

35
Andrew Pennock Answer: 5
In the study by Matava 16% of pt’s presenting with SCFE had a chief complaint of distal thigh or knee pain. Pt’s presenting with thigh or knee pain were more likely to be misdiagnosed and undergo unnecessary or uninformative radiographs. Therefore, surgeons taking care of pediatric pt’s must keep a high index of suspicion of SCFE when a pt presents with knee or thigh pain. Matava MJ, Patton CM, Luhmann S, et al: Knee pain as the initial symptom of slipped capital femoral epiphysis. J pediatr Orthop 1999;19: Loder RT, Aronsson DD, Dobbs MD, et al: Slipped capital femoral epiphysis. Instr Course Lect 2001;50:

36
Question A high ankle sprain caused by an external rotation mechanism of injury primarily involves which of the following ligaments? Posterior talofibular 2. Anterior talofibular 3. Calcaneofibular 4. Anterior inferior tibiofibular 5. Posterior inferior tibiofibular

37
Talac Answer: 4 Clanton TO, Paul P. Syndesmosis injuries in athletes
Talac Answer: 4 Clanton TO, Paul P. Syndesmosis injuries in athletes. Foot Ankle Clin Sep;7(3): The key to syndesmosis injuries is early recognition of the injury pattern and appropriate treatment. The clinician must be wary of the ankle sprain that is slow to heal. Radiographic criteria should be examined closely when considering the diagnosis; if surgery is warranted, attention to the health of the soft tissue envelope is key. Late repairs or reconstructions never have as favorable an outcome as the properly repaired acute injury. Postoperative rehabilitation should be monitored closely and care should be taken to avoid early return to activity that could result in reinjury or damage to the surgical repair or reconstruction
: The key to syndesmosis injuries is early recognition of the injury pattern and appropriate treatment. The clinician must be wary of the ankle sprain that is slow to heal. Radiographic criteria should be examined closely when considering the diagnosis; if surgery is warranted, attention to the health of the soft tissue envelope is key. Late repairs or reconstructions never have as favorable an outcome as the properly repaired acute injury. Postoperative rehabilitation should be monitored closely and care should be taken to avoid early return to activity that could result in reinjury or damage to the surgical repair or reconstruction.")
38
Question The most common bone bruise pattern resulting from an acute tear of the anterior cruciate ligament is the central third of the medial femoral condyle and the medial tibial plateau medial femoral condyle and the lateral tibial plateau medial femoral condyle and the posterior third of the medial tibial plateau. 4. lateral femoral condyle and the medial tibial plateau 5. lateral femoral condyle and the posterior third of the lateral tibial plateau.

39
Answer: 5 HENTZEN. Graf et al
Answer: HENTZEN Graf et al. performed magnetic resonance imaging on the knees of 98 consecutive patients with clinically diagnosed anterior cruciate ligament injuries. They found 48% with focal signal abnormalities consistent with the diagnosis of a "bone bruise." Seventy-one percent of the magnetic resonance images taken within 6 weeks of injury demonstrated a bone bruise, whereas no scans done longer than 6 weeks after injury showed a bruise. Also significant was the tendency for lesions to be located in the lateral compartment. In the sagittal plane, lesions were most likely to be in the middle third of the lateral femoral condyle and the posterior third of the lateral tibial plateau. In 31 patients evaluated arthroscopically, there was no correlation between the presence or location of a bone bruise and articular alterations or meniscal tears observed at surgery. Graf BK, Cook DA, De Smet AA, Keene JS. "Bone bruises" on magnetic resonance imaging evaluation of anterior cruciate ligament injuries. Am J Sports Med 1993; 21:220-3 Johnson DL, Bealle DP, Brand JC Jr, et al. The effect of a geographic lateral bone bruise on knee inflammation after acute ACL rupture. Am J Sports Med 2000; 28:152-5 Lahm A, Erggelet C, Steinwachs M, et al. Articular and osseous lesions in recent ligament tears: arthroscopic changes compared with magnetic resonance imaging findings. Arthroscopy 1998; 14:

40
Question In laboratory studies testing the strength of anterior cruciate ligament grafts, what graft construct has the highest tensile strength? mm bone-patella-bone allograft mm bone-patella-bone autograft mm Achilles tendon allograft 4. doubled semitendinosus allograft 5. quadrupled semitendinosus autograft

41
Answer: 5. J. Hall The referenced articles conclude:
Answer: J. Hall The referenced articles conclude: 9 or 10 mm BTB graft 120% of native ACL strength 14mm BTB graft % of native ACL strength Single Semtendinosus graft 70% of native ACL strength Double Semitendinous graft 140% of native ACL strength Quadrupled Semitendinousus graft 250% of native ACL strength No mention was made of achilles tendon grafts (answer 3). In regards to BTB allograft vs autograft (answers 1,2) all of the cadaveric grafts tested would have been autografts when placed into the patients they came from, and allografts when placed into someone else; either way, the initial tensile strength would presumably have been the same. There is some evidence that after 2 years allografts have a higher failure rate, possibly because of late tensile failure (Malek and AAOS annual meeting 1993). Chen L, Cooley V, Rosenberg T: ACL reconstruction with hamstring tendon. Orthop Clin North Am 2003;34:9-18 Hamner DL, Brown CH Jr, Steiner ME, Hecker AT, Hayes WC: Hamstring tendon grafts for reconstruction of the anterior cruciate ligament: Biomechanical evaluation of the use of multiple strands and tensioning techniques. J Bone Joint Surg Am 1999;81:
. In regards to BTB allograft vs autograft (answers 1,2) all of the cadaveric grafts tested would have been autografts when placed into the patients they came from, and allografts when placed into someone else; either way, the initial tensile strength would presumably have been the same. There is some evidence that after 2 years allografts have a higher failure rate, possibly because of late tensile failure (Malek and AAOS annual meeting 1993). Chen L, Cooley V, Rosenberg T: ACL reconstruction with hamstring tendon. Orthop Clin North Am 2003;34:9-18 Hamner DL, Brown CH Jr, Steiner ME, Hecker AT, Hayes WC: Hamstring tendon grafts for reconstruction of the anterior cruciate ligament: Biomechanical evaluation of the use of multiple strands and tensioning techniques. J Bone Joint Surg Am 1999;81:")
42
Question A patient who underwent anterior cruciate ligament (ACL) reconstruction with a central one third bone-patellar tendon-bone autograft 6 months ago now reports anterior knee pain. Examination reveals that the incisions are well healed, there is no effusion, quadriceps girth is decreased 1 cm compared with the contralateral side, knee range of motion is from 0 to 130 deg with mild patellofemoral crepitation and compression pain, and the KT-1000 side-to-side difference is 1 mm. What is the next most appropriate step in management? 1. Electromyography 2. Arthroscopy 3. Revision ACL reconstruction 4. MRI 5. Physical therapy

43
Answer: J. Hall We are given a history of anterior knee pain 6 months after ACL reconstruction. The 1mm side to side difference rules out graft failure and therefore need for revision (answer 3). There is normal range of motion, so no to answers 2 and 4. There is no evidence given for nerve damage, a very rare complication of ACL surgery, and therefore no need for an EMG (answer 1). For BTB ACL reconstructions “the development of anterior knee pain has been associated with less aggressive rehabilitation methods” when compared to Hamstring ACL reconstructions (Freedman). Freedman KB, D’Amato MJ, Nedeff DD, Kaz A, Bach BR Jr: Arthroscopic anterior cruciate ligament reconstruction: A meta-analysis comparing patellar tendon and hamstring tendon autografts. Am J Sports med 2003;31:2-11 Arendt EA (ed): Orthopaedic Knowledge Update: Sports Medicine 2. Rosemont, IL, American Academy of Orthopaedic Surgeons, 2000, pp
. There is normal range of motion, so no to answers 2 and 4. There is no evidence given for nerve damage, a very rare complication of ACL surgery, and therefore no need for an EMG (answer 1). For BTB ACL reconstructions the development of anterior knee pain has been associated with less aggressive rehabilitation methods when compared to Hamstring ACL reconstructions (Freedman). Freedman KB, D’Amato MJ, Nedeff DD, Kaz A, Bach BR Jr: Arthroscopic anterior cruciate ligament reconstruction: A meta-analysis comparing patellar tendon and hamstring tendon autografts. Am J Sports med 2003;31:2-11 Arendt EA (ed): Orthopaedic Knowledge Update: Sports Medicine 2. Rosemont, IL, American Academy of Orthopaedic Surgeons, 2000, pp")
44
Question A 19 y.o. woman felt a pop as she hyperextended her knee during a football game 6 months ago. She now reports a valgus thrust with walking. Examination reveals hyperextension and increased external rotation at 30 degrees. The Lachman’s test reveals a firm end point, and results of the posterior drawer test are negative. Management should consist of 1. reconstruction of the posterolateral corner. 2. Reconstruction of the anterior cruciate ligament Reconstruction of the posterior cruciate ligament A hinged knee brace Physical therapy for biceps femoris strengthening. Scott Ball

45
Answer – 1 The question describes a posterolateral corner injury and those need surgery. Mechanism of injury is usually knee hyperextension combined with a varus stress. Components of a posterolateral injury include disruption of the popliteus tendon, the arcuate ligament complex (partial or complete), and the LCL and lateral capsular ligament. These are usually avulsed distally. Physical exam findings: The patient may show an apparent increased tibia vara with a lateral thrust. The dial test is performed with the patient prone. External rotation of the leg is checked at 30 degrees and 90 degrees. With posterolateral corner injuries there is increased external rotation noted at 30 degrees. A side to side difference of greater than 10 degrees is considered positive. This is the exam finding described in this question. With the external rotation / recurvatum test grab both of the patient’s big toes and hold the legs up off the exam table. The involved side will fall into varus, hyperextension, and external rotation. Lastly, do your neuro exam because peroneal nerve injuries are found in 15% of patients. Radiographic findings include the arcuate sign which refers to an avulsion fracture of the proximal fibula seen on plain xrays. On MRI, there may be a bone contusion to the medial femoral condyle in addition to avulsion of the LCL with or without a fibular avulsion fracture. Briefly, surgical treatment should be done early because this is the only way to perform an anatomic repair. In chronic cases, repair is not possible so reconstruction is the only option (as in this patient). Scott Ball

46
Question A 17-year-old soccer player struck his head on an opposing player’s knee, resulting in an episode of altered consciousness in the first period of a game. The athlete may return to play in the same game if the 1. only neurologic deficits are motor deficits 2. only neurologic deficits are sensory deficits period of loss of consciousness lasts less than 2 minutes 4. patient reports on a headache without motor or sensory loss signs and symptoms resolve within 15 minutes or less at rest and with exercise

47
Answer: Fricka This question deals with concussions in sports and the ability to return to play. The referenced paper provides these guidelines. Every athlete with a concussion should be evaluated by a physician. Return to play classifications Same day Signs and symptoms cleared within 15 minutes or less at rest and exertion Normal neurologic examination No documented loss of consciousness Delayed return to play (Not the same day) Signs and symptoms did not clear in 15 at rest or with exertion Documented loss of consciousness Any deterioration in physical or mental status after the initial trauma warrants transport to emergency facility for neuro consult and imaging Wojtys EM, Hovda D, Landry G, Boland A, Lovell M, McCrea M, Minkoff J. Current concepts. Concussion in sports. Am J Sports Med Sep-Oct;27(5):
 Signs and symptoms did not clear in 15 at rest or with exertion. Documented loss of consciousness. Any deterioration in physical or mental status after the initial trauma warrants transport to emergency facility for neuro consult and imaging. Wojtys EM, Hovda D, Landry G, Boland A, Lovell M, McCrea M, Minkoff J. Current concepts. Concussion in sports. Am J Sports Med Sep-Oct;27(5):")
48
Question When harvesting hamstring grafts for an anterior cruciate ligament reconstruction, what nerve can be injured as it passes superficially to the gracilis tendon at the posteromedial joint line? 1. Peroneal 2. Femoral Saphenous 4. Tibial Sciatic

49
Answer: This is a straightforward anatomy question and the 2 references illustrate the question’s point well. To expose the semi-tendinous and gracilis tendons one must divide the sartorius fascia and the saphenous nerve exits from underneath this fascia. The illustration show how close it is to the underlying hamstring tendons. To help minimize risk to this nerve the case report recommends knee flexion and hip external rotation to allow the nerve to fall posterior out of the way from the tendon passer for harvesting. Solman CG Jr, Pagnani MJ. Hamstring tendon harvesting. Reviewing anatomic relationships and avoiding pitfalls. Orthop Clin North Am Jan;34(1):1-8. Bertram C, Porsch M, Hackenbroch MH, Terhaag D. Saphenous neuralgia after arthroscopically assisted anterior cruciate ligament reconstruction with a semitendinosus and gracilis tendon graft. Arthroscopy Oct;16(7):763-6.
:1-8. Bertram C, Porsch M, Hackenbroch MH, Terhaag D. Saphenous neuralgia after arthroscopically assisted anterior cruciate ligament reconstruction with a semitendinosus and gracilis tendon graft. Arthroscopy Oct;16(7):")
50
Question A 21-year-old woman who plays softball injured her knee while sliding into second base. An AP radiograph shows a lateral chip fracture adjacent to the lateral joint line. What structure of the knee has most likely been injured? Iliotibial band Popliteus tendon Lateral collateral ligament Anterior cruciate ligament Posterior cruciate ligament Klane White

51
Answer: 4 The Segond fracture is indicative of an ACL injury % of the time. This is a small, vertical avulsion fracture at the lateral aspect of the proximal tibia, just distal to the tibial plateau, typically yielding an elliptical fracture fragment. There is some discrepancy in the literature about which soft tissue structure is actually avulsed. Candidates include the lateral collateral ligament, the lateral meniscotibial ligament and the posterior insertion of the iliotibial band. In terms of this question, the actual ligament injured is the ACL, while IT band and LCL are the possible ligaments avulsed, but not necessarily injured, making ACL the best answer. The mechanism of injury is thought to be flexion, varus and internal rotation of the tibia. Klane White

52
Klane White Segond fractures were found in close to 10% of the ACL injuries reported in the study by Hess et al. In a control group of 133 knees with internal derangements of the knee other than an ACL injury, there was only one patient with an equivocal chip fracture of the lateral tibial plateau. Fracture of the anterior tibial spine and impaction of the lateral femoral condyle are also indicative of ACL injury or insufficiency.

53
Klane White Rreferences: Hess T et al. (1994) Lateral tibial avulsion fractures and disruptions to the anterior cruciate ligament: A clinical study of their incidence and correlation. Clin. Orthop. 303: Kezdi-Rogus PC et al. (1994) Radiologic case study: Plain film manifestations of ACL injuries. Orthopoaedics 17:
 Lateral tibial avulsion fractures and disruptions to the anterior cruciate ligament: A clinical study of their incidence and correlation. Clin. Orthop. 303: Kezdi-Rogus PC et al. (1994) Radiologic case study: Plain film manifestations of ACL injuries. Orthopoaedics 17:")
Similar presentations




>")
















