Download presentation
Presentation is loading. Please wait.

1
MSK Revision Nerve Palsies

2
Tips … Have a plan and stick to it!! Rest – take regular breaks and get your sleep If you can easily turn it into an exam question Warwick have probably thought of it too! Ask if you need help…. ask anyone!

3
Covering… Nerve palsies Sensory innervation Hopefully:
Blood supply (arterial and venous) Clinical landmarks NOT covered: Anatomy Hand signs of disease Compartments Joints Shoulder – Dislocation, rotator cuff, pathologies Elbow – nurse maids, anatomy, tennis/golfer’s elbow Wrist – Carpal bones
 Clinical landmarks. NOT covered: Anatomy. Hand signs of disease. Compartments. Joints. Shoulder – Dislocation, rotator cuff, pathologies. Elbow – nurse maids, anatomy, tennis/golfer’s elbow. Wrist – Carpal bones.")
4
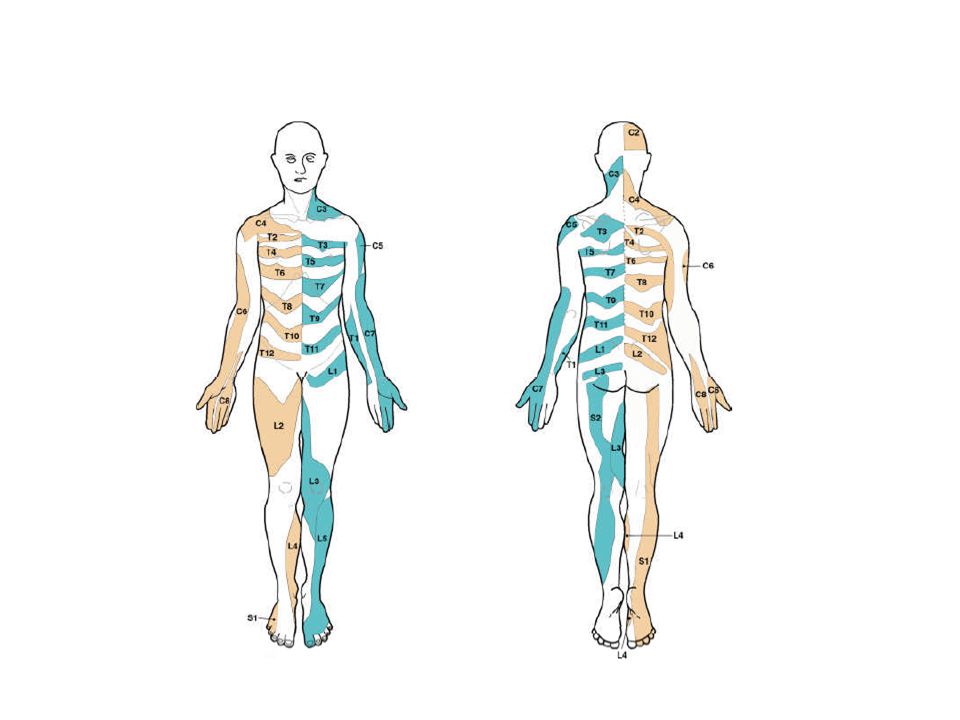
What is a dermatome? Area of skin innervated by a single spinal nerve Group of muscles innervated by a single nerve root A branching network of vessels or nerves Nerve cell cluster or a group of nerve cell bodies located in the peripheral nervous system

5
What is a dermatome? Area of skin innervated by a single spinal nerve - Dermatome Group of muscles innervated by a single nerve root - Myotome A branching network of vessels or nerves - Plexus Nerve cell cluster or a group of nerve cell bodies located in the peripheral nervous system – Ganglion

6
The Upper Limb

7
Anterior compartment of the arm.
Biceps brachii – Flexion at the elbow, supination of the forearm (Short head: coracoid process of the scapula. Long head: supraglenoid tubercle) Brachialis – Flexion of the elbow (most powerful flexor) Coracobrachialis – Flexion at the elbow, flexion of the shoulder, ?abduction of the arm Posterior compartment of the arm: Triceps brachii – elbow extension Lateral, medial and middle heads. Anconeous – stabilises the elbow during movement Anterior compartment of the forearm: Pronator teres Flexor carpia radialis Palmaris longus Flexor digitorum superficialis Flexor digitorum profundus Flexor pollicis longus Median – interosseous nerve Pronator quadratus
 Brachialis – Flexion of the elbow (most powerful flexor) Coracobrachialis – Flexion at the elbow, flexion of the shoulder, abduction of the arm. Posterior compartment of the arm: Triceps brachii – elbow extension. Lateral, medial and middle heads. Anconeous – stabilises the elbow during movement. Anterior compartment of the forearm: Pronator teres. Flexor carpia radialis. Palmaris longus. Flexor digitorum superficialis. Flexor digitorum profundus. Flexor pollicis longus Median – interosseous nerve. Pronator quadratus.")
8
Axilary Nerve Musculocutaneous Median Nerve Radial Nerve Ulnar Nerve
(Long thoracic nerve) Musculocutaneous: C5-7Median: C6 - T1 Redial: C5 - T1 Ulnar: C8 & T1 Axillary*: C5 & 6 *Strictly speaking not part of the branches. But important nontheless
 Musculocutaneous: C5-7Median: C6 - T1. Redial: C5 - T1. Ulnar: C8 & T1. Axillary*: C5 & 6. *Strictly speaking not part of the branches. But important nontheless.")
9
Axillary Nerve (C5) Innervates: Deltoid Teres minor Vulnerable during:
Shoulder dislocation Fracture of the surgical neck of the humerus Intramuscular injection (Runs 5cm below the aromiom) Damage can result in: Paralysis of deltoid and teres minor Limb hang limp by side Loss of shoulder contour Sensory Loss over lateral shoulder (regimental badge area)
 Damage can result in: Paralysis of deltoid and teres minor. Limb hang limp by side. Loss of shoulder contour. Sensory Loss over lateral shoulder (regimental badge area)")
10
Musculotaneous nerve (C5 – 7)
Innervation BBC Biceps Brachii Brachialis Coracobrachialis Vulnerable during: ‘Stretch’ injury during dislocation Damage results in: Weakness of flexion Weakness of supination Sensory loss over the lateral forearm

11
Why in musculocutaneous nerve damage is it still possible to flex the elbow?
Flexion is still possible as the brachioradialis also performs this function and it is innervated by the radial nerve

12
Thenar wasting is a sign of damage to which nerve?
Ulnar nerve Median nerve Radial nerve Axillary nerve

13
Thenar wasting is a sign of damage to which nerve?
Ulnar nerve Median nerve Radial nerve Axillary nerve

14
Median nerve (C6 – T1) Innervates: Pronator teres
Flexor carpia radialis Palmaris longus Flexor digitorum superficialis Flexor digitorum profundus Flexor pollicis longus Pronator quadratus LOAF: Lumbricals 1 & 2 (Digits 2 & 3) Opponens pollicis Abductor pollicis brevis Flexor pollicis brevis Superficial Intermediate Deep Hand
 Opponens pollicis. Abductor pollicis brevis. Flexor pollicis brevis. Superficial. Intermediate. Deep. Hand.")
15
Median Nerve Injury Damage at the Elbow or proximal Can’t make fist with digits 2&3 (hand of ‘benediction’) No active flexion of IP joints of digits 2&3 Weaker flexion of digits 4&5 = No FDS but FDP from ulnar nerve No forearm pronation Weak wrist flexion that deviates to adduction (FCU = ulnar nerve) Plus damage seen with wrist injury below...... X X Damage at the Wrist Thenar wasting & opposition not possible Thumb laterally rotated & adducted Digits 2 & 3 lag in fist making as lumbricals 1 & 2 paralysed R G Tunstall 2014
 Plus damage seen with wrist injury below X. X. Damage at the Wrist. Thenar wasting & opposition not possible. Thumb laterally rotated & adducted. Digits 2 & 3 lag in fist making as lumbricals 1 & 2 paralysed. R G Tunstall")
16
Carpal Tunnel Syndrome
“Compression of the median nerve in the carpal tunnel” What are the symptoms a patient may complain of with carpal tunnel? Sensory loss in the lateral 3.5 digits Nocturnal pain in the lateral 3.5 digits Thenar wasting What conditions can increase the chance/are associated with carpal tunnel syndrome? Pregnancy Hypothyroidism What passes through the carpal tunnel? 4 tendons of flexor digitorum superficialis 4 tendons of flexor digitorum profundus Flexor policis longus Median nerve Describe the surface anatomy of the carpal tunnel. The canal starts at the distal wrist crease and passes distally by about 2cm

17
What make the roof of the carpal tunnel?
Extensor retinaculum Flexor retinaculum Biceps aponeurosis Carpal bones

18
What make the roof of the carpal tunnel?
Extensor retinaculum Flexor retinaculum Biceps aponeurosis Carpal bones

19
“Wrist drop” is a sign of damage to which nerve?
Axillary Median Radial Ulnar Musculocutaneous

20
“Wrist drop” is a sign of damage to which nerve?
Axillary Median Radial Ulnar Musculocutaneous

21
Radial Nerve (C5 – T1) What does the radial nerve supply? All of the posterior compartments of the arm and forearm PLUS brachioradialis Where is the radial nerve injured? Axilla – Shoulder dislocation, crutches, falling asleep over upper limb ‘Saturday night palsy’ Spiral groove - Humeral fracture (sleeping on the arm) Head/neck of the radius - #
 Head/neck of the radius - #")
22
What travels with the radial nerve in the radial groove?
Brachial artery Profunda brachii artery Axillary artery Cutaneous branch of the radial nerve

23
What travels with the radial nerve in the radial groove?
Brachial artery Profunda brachii artery Axillary artery Cutaneous branch of the radial nerve

24
X X X Radial Nerve Injury All function lost No elbow extension
Damage in axilla All function lost No elbow extension Wristdrop No digit extension Sensory loss on dorsolateral forearm & hand X X Damage in spiral groove Elbow extension preserved but weaker Wristdrop No digit extension Sensory loss on dorsolateral forearm & hand X Damage at radial head/neck Elbow extension normal Minimal wristdrop (ECR supplied earlier) No sensory loss - motor nerve R G Tunstall 2014
 No sensory loss - motor nerve. R G Tunstall")
25
Why do patient with wrist drop lose their power grip?
The wrist needs to be held in the neutral (anatomical) position by extensors in order to bring about a power grip. Lack of extensor action means wrist flexion occurs when FDP & FDS contract, thus rendering them mechanically unable to flex the digits tightly.
 position by extensors in order to bring about a power grip. Lack of extensor action means wrist flexion occurs when FDP & FDS contract, thus rendering them mechanically unable to flex the digits tightly.")
26
Explain why forearm supination is still possible in the damaged limb following radial nerve damage (2 marks)? Supination is brought about by two muscles, supinator (radial nerve innervated and therefore paralysed) and biceps brachii (musculocutaneous nerve innervated and therefore working).
 and biceps brachii (musculocutaneous nerve innervated and therefore working).")
27
Wasting of the 1st dorsal interosseous is a sign of damage to which nerve?
Axillary Median Ulnar Radial Musculocutaneous

28
Wasting of the 1st dorsal interosseous is a sign of damage to which nerve?
Axillary Median Ulnar Radial Musculocutaneous

29
Ulnar nerve C8 – T1 What does this nerve innervate?
Flexor carpi ulnaris Flexor digitorum profundus to digits 4 & 5 All intrinsic muscles in the hand EXCEPT thenar and lumbrical 1 & 2 Where can damage to this nerve occur? Medial epicondyle – fracture or compression Guyon’s canal – compression

30
Ulnar Nerve Injury Damage at the elbow or proximal No flexion of distal IP joint of Digits 4 & 5 = Lack of FDP Wrist abducts on flexion = Lack of FCU No digit ab-or adduction (except thumb abduction) Some clawing of digits 4 & 5 at rest = loss of lumbricals & interossei No clawing of digits 2 & 3 as lumbricals 1 & 2 OK Plus damage seen with wrist injury below..... X Damage at the wrist Loss of most intrinsic hand muscles Hypothenar & interosseous wasting Clawing of digits 4 & 5 worse in low lesion as FDP remains innervated and exacerbates IP joint flexion X R G Tunstall 2014
 Some clawing of digits 4 & 5 at rest = loss of lumbricals & interossei. No clawing of digits 2 & 3 as lumbricals 1 & 2 OK. Plus damage seen with wrist injury below..... X. Damage at the wrist. Loss of most intrinsic hand muscles. Hypothenar & interosseous wasting. Clawing of digits 4 & 5 worse in low lesion as FDP remains. innervated and exacerbates IP joint flexion. X. R G Tunstall")
31
Describe the resting appearance of someone with ulnar claw.
This is extension of the MCP and flexion of the corresponding IP joints Describe the ulnar paradox If you damage the ulnar nerve at the wrist you will get more clawing and more damage than if you damaged the ulnar nerve more proximally. The reason this happens is because if you damage the ulnar nerve at elbow you also paralyse the flexor digitorum profundus for digits 4 & 5 and therefore get far less clawing of digits 4 & 5. If you damage the ulnar nerve at the wrist the flexor digitorum profundus for digits 4 & 5 is still innervated and will produce greater clawing.

32
Where do you test for sensory loss following damage to the:
Axillary nerve Radial nerve Ulnar nerve Median nerve

33
Where do you test for sensory loss following damage to the:
Axillary nerve – Regimental badge area Radial nerve – First dorsal interosseous Ulnar nerve – Hypothenar eminance Median nerve – Thenar eminance

34
Winging of the scapula is a sign of damage to which nerve?
Axillary nerve Musculocutaneous nerve Long thoracic nerve Lateral cutaneous nerve of the

35
Winging of the scapula is a sign of damage to which nerve?
Axillary nerve Musculocutaneous nerve Long thoracic nerve Lateral cutaneous nerve of the

36
Long Thoracic Nerve (C5 – 7)
What muscle does this nerve supply? Which ribs does this muscle attach to? How can this nerve be damaged? What movements may a patient find difficult?

37
Long Thoracic Nerve (C5 – 7)
What muscle does this nerve supply? Serratus anterior Which ribs does this muscle attach to? Ribs 1 – 8 Inserts into medial border of the scapula How can this nerve be damaged? At risk during axillary surgery. This is because the LTN lies on the superficial layer of muscle as opposed to the deep layer as most other nerves are. What movements may a patient find difficult? Punching out Reaching out

38
What is a painful arc indicative of?
Supraspinatus impingement Calcific tendonosis Adhesive capsulitis Axillary nerve damage

39
What is a painful arc indicative of?
Supraspinatus impingement Calcific tendonosis Adhesive capsulitis Axillary nerve damage

40
Klumpke’s Palsy C8 – T1 Erb’s Palsy C5 – 6
Traction injury Cancer at lung apex**** Compession via cervical rib Ulnar nerve and Median nerve effected Erb’s Palsy C5 – 6 Stab wounds Iatrogenic Shoulder dystocia - Suprascapular Lateral pectoral Axillary Musculocutaneous Dorsal scapula

41
Erb’s Palsy Medially Rotated Shoulder: loss of supra and infraspinatis resulting in unopposed medial rotation from the sternal head of pec major Limp & loss of shoulder contour: Result of loss of deltoid Pronated forarm: Loss of biceps brachii Partial wrist drop: Loss of extensor carpi radialis

42
Erb’s Palsy Medially Rotated Shoulder: loss of supra and infraspinatis resulting in unopposed medial rotation from the sternal head of pec major Limp & loss of shoulder contour: Result of loss of deltoid Pronated forarm: Loss of biceps brachii Partial wrist drop: Loss of extensor carpi radialis Suprascapula Lateral Pectoral Axillary Musculocutaneous Dorsal Scapula

43
Klumpke’s Palsy C8 – T1 How does Klumpke’s Palsy present (3 marks)? Paralysis & wasting of ALL small muscles of hand Clawing of digits 2-5 at rest due to unopposed action of extensors on MCP joint & long flexors on IP joints Anaesthesia = medial elbow, forearm & arm

44
Horner’s Syndrome What are the signs of Horner’s syndrome? Ptosis – Droopy eyelid Miosis – Constricted pupil Enophtalmos – Sunken eyes Anhydrosis – Lack of sweating Red flush skin - Vasodilation What are the causes of Horner’s syndrome? Pancoast tumour Tumour of skull base Lymphadenopathy Iatrogenic Trauma

45
What are the anatomical boundaries of the anatomical snuff box?
Ventro-lateral: abductor pollicis longus & extensor pollicis brevis Dorso-medial: Extensor pollicis longus Floor :formed by the scaphoid and trapezium What are the contents of the anatomical snuff box (3 marks)? Radial artery Cutaneous branch of the radial nerve Cephalic Vein
 Radial artery. Cutaneous branch of the radial nerve. Cephalic Vein.")
47
What should pain in the anatomical snuff box arouse suspicion of?
Superficial radial nerve damage De Quervain’s Scaphoid fracture Ulnar nerve damage

48
What should pain in the anatomical snuff box arouse suspicion of?
Superficial radial nerve damage De Quervain’s Scaphoid fracture Ulnar nerve damage

49
What is the most common method of fracturing your scaphoid?
Falling on an outstretched arm What is a big concern in fractures of the scaphoid, explain why this is so anatomically. A fraccture of the scaphoid may result in avascular necrosis, however this is more common in the proximal 1/3 as blood supply is retrograde from branches of the radial artery supplying the distal part of the bone first and then the more proximal part.

50
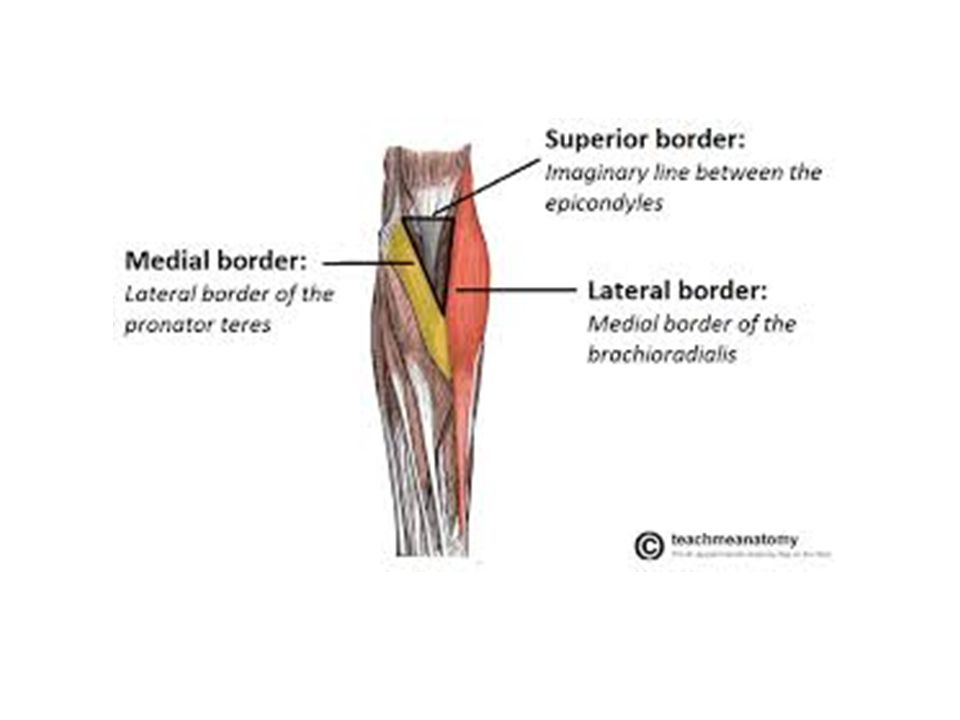
What are the borders of the cubital fossa?
Lateral: Brachioradialis Medial: Pronator Teres Superior Border: Inter-epicondyle line Roof: Aponeurosis of biceps What are the contents of the cubital fossa from lateral to medial (3 marks)? Biceps Tendon Brachial Artery Median Nerve Which veins are accessed in this area (3 marks)? Cephalic Basilic Median cubital vein
 Biceps Tendon. Brachial Artery. Median Nerve. Which veins are accessed in this area (3 marks) Cephalic Basilic Median cubital vein.")
52
What are the borders of the axilla?
Anterior: Pectoral Muscles - Anterior Axillary fold Posterior: Subscapularis and scapula, Posterior Axillary fold (Lat dorsi and teres major) Medial: Serratus Anterior and lateral thoracic wall Lateral: Intertubercular groove What are the names of the axillary lymph nodes? Central Humeral Apical Pectoral Subscapular (NOTE: Think CHAPS)
 Medial: Serratus Anterior and lateral thoracic wall. Lateral: Intertubercular groove. What are the names of the axillary lymph nodes Central. Humeral. Apical. Pectoral. Subscapular. (NOTE: Think CHAPS)")
54
An F1 is performing an injection in a patient’s butt!
To ensure that the needle is placed in a safe area they draw a vertical line through highest point of crest and another line from PSIS to the greater trochanter and inject into the upper outer quadrant of the patient's gluteal region. What nerve is the Dr trying to avoid by employing this method? Pudendal nerve Superior gluteal nerve Inferior gluteal nerve Sciatic nerve

55
An F1 is performing an injection in a patient’s butt!
To ensure that the needle is placed in a safe area they draw a vertical line through highest point of crest and another line from PSIS to the greater trochanter and inject into the upper outer quadrant of the patient's gluteal region. What nerve is the Dr trying to avoid by employing this method? Pudendal nerve Superior gluteal nerve Inferior gluteal nerve Sciatic nerve

56
What are the nerve roots of the sciatic nerve?
L4 – S3

57
Which nerve do you suspect is damaged based on the following observation of a patient’s gait?
“Gait in which trunk lurches back on heel strike to prevent it from toppling forward” Inferior gluteal nerve Superior gluteal nerve Sciatic nerve Femoral nerve

58
Which nerve do you suspect is damaged based on the following observation of a patient’s gait?
“Gait in which trunk lurches back on heel strike to prevent it from toppling forward” Inferior gluteal nerve Superior gluteal nerve Sciatic nerve Femoral nerve

59
A 35 year old male tears his medial collateral ligament during a football match. What else might be damaged and with what consequence? A 17 year old female is hit by a moving car on the lateral side of her knee. Why is she at risk of foot drop? A 76 year old man presents to you with a deep laceration to the region behind his medial malleolus. Examination reveals that crude flexion-extension movement of his toes is possible, but they splay whilst weight-bearing and he is unable to curl/scrunch his toes up. Why? A 56 year old male suffers a supracondylar fracture of the femur. 30 minutes later the pain is considerably worse and the back of his thigh is swollen, and he was loosing sensation in, and functioning of, his leg and foot. What might be damaged and with what consequence?

Similar presentations








>")

>")









