Download presentation
Presentation is loading. Please wait.

1
1st TRIMESTER PREGNANCY FAILURE Shortened to emphasize medical student curriculum requirements
Carlos M. Fernandez, M.D Department of Obstetrics and Gynecology Advocate Illinois Masonic and Medical Center

2
Ultrasound diagnosis of intrauterine pregnancy

3
Diagnosis of IUP “Double decidual sign” at 4½ to 5 wks
Gestational sac + yolk sac at 5 wks (a definitive sign of IUP) GS + yolk sac + embryo at 5½ to 6 wks CRL >5 mm – fetal cardiac activity present Seeber BE and Barnhart KT. Obstet Gynecol 2006;107:
 GS + yolk sac + embryo at 5½ to 6 wks. CRL >5 mm – fetal cardiac activity present. Seeber BE and Barnhart KT. Obstet Gynecol 2006;107:")
4
Tips for Students Gestational age IUP=intrauterine pregnancy
Could include a live intrauterine pregnancy, a threatened abortion, an inevitable abortion, an incomplete abortion, or a missed abortion Does not include ectopic pregnancy, completed miscarriage, or a molar pregnancy Gestational age The age of the pregnancy in weeks since the last menstrual period About 2 weeks longer than the embryonic age

5
Tips for Students Try to memorize the gestational ages at which the markers of an intrauterine pregnancy appear…. But more importantly, you should understand what is required to confirm an intrauterine pregnancy This is how we rule out ectopic pregnancies and molar pregnancies If there is any possibility of an intrauterine pregnancy, you cannot give methotrexate or cytotecyou could cause an elective abortion

6
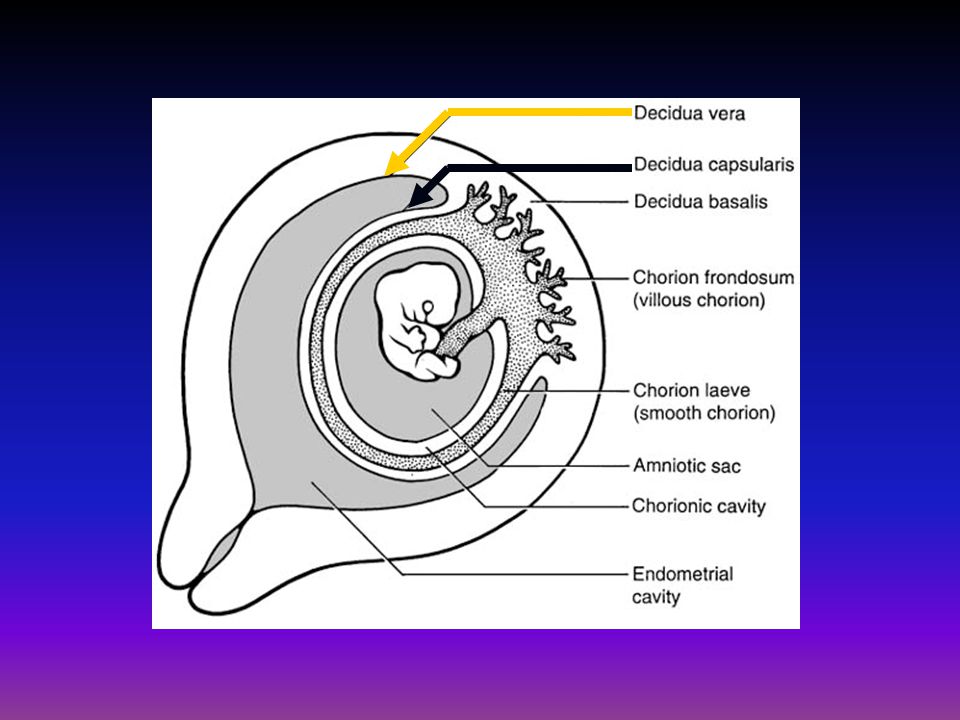
Gestational sac Double decidual sign
The first sign of an intrauterine pregnancy Gestational sac Double decidual sign

7
First sign of IUP: double decidual sign
Earliest finding is the “double decidual sign” (arrows) seen around 4½-5 wks gestation initially eccentric in location It excludes pseudogestational sac (free fluid or blood within endometrium)
 seen around 4½-5 wks gestation. initially eccentric in location. It excludes pseudogestational sac (free fluid or blood within endometrium)")
9
Double-decidual sign ( 5 weeks' menstrual age)
Double-decidual sign ( 5 weeks' menstrual age). The decidua vera (dv) can be discerned from the decidua capsularis (dc) and chorion laeve surrounding the gestational sac. A small subchorionic hemorrhage(*) is present between the unopposed layers of decidua vera.
. The decidua vera (dv) can be discerned from the decidua capsularis (dc) and chorion laeve surrounding the gestational sac. A small subchorionic hemorrhage(*) is present between the unopposed layers of decidua vera.")
11
Gestational Sac (confirmed by double decidual sign)
Grows 1 mm per day Usually seen by 4 ½ to 5 weeks of gestation Discriminatory ß-hCG with TVUS (the level of ß-hCG above which you should be able to see a gestational sac on transvaginal ultrasound): Usually quoted ß-hCG IU/L At AIMMC, we use 1500 IU/L
: Usually quoted ß-hCG IU/L. At AIMMC, we use 1500 IU/L.")
12
Gestational Sac Discriminatory ß-hCG with transvaginal ultrasound :
ß-hCG IU/L Discriminatory ß-hCG with trans-abdominal ultrasound: ≥ 6500 ß-hCG IU/L Bhatt & Dogra, Radiol Clin N Am 45 (2007)
")
13
The gestational sac diameter is used to calculate gestational age
Long axis Short axis

14
Second sign of intrauterine pregnancy
Yolk sac

15
Second sign of IUP: Yolk Sac
First structure visualized within the gestational sac Round , bright ring A definitive sign of IUP Involutes after 11 weeks Can be seen half a week before normal embryo is seen When enlarged (“hydropic”), solid or duplicated, it is a very poor prognosis sign
, solid or duplicated, it is a very poor prognosis sign.")
16
Gestational sac and yolk sac (5 weeks' menstrual age)
Gestational sac and yolk sac (5 weeks' menstrual age). A normal yolk sac is visualized. The embryo is not identified. The decidua vera (dv) and decidua capsularis (dc) (double-decidual sign) are identified.
. A normal yolk sac is visualized. The embryo is not identified. The decidua vera (dv) and decidua capsularis (dc) (double-decidual sign) are identified.")
17
Third sign of intrauterine pregnancy
Fetal pole

18
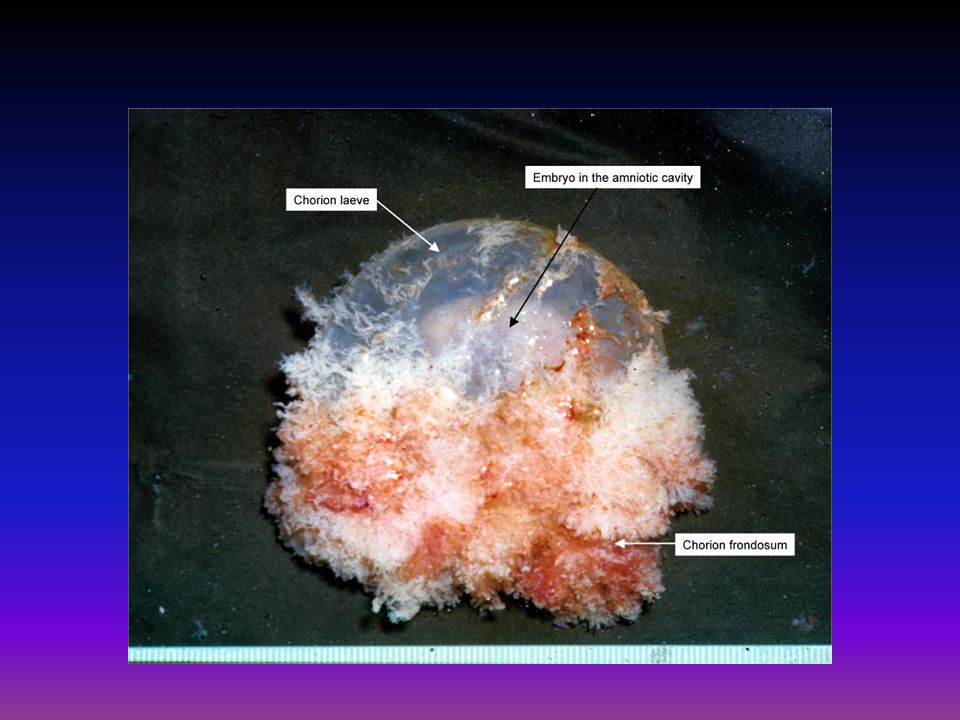
Third sign of IUP: GS + yolk sac + embryo
GS + yolk sac + fetal pole at 5½ to 6 wks The fetal pole (arrow) is better seen on the zoomed in image GS grows 1mm/day Embryo grows 1mm/day
 is better seen on the zoomed in image. GS grows 1mm/day. Embryo grows 1mm/day.")
19
Fourth sign of intrauterine pregnancy
Cardiac activtiy

20
Fourth sign of IUP: GS + YS + embryo + cardiac activity
Double decidual sign +yolk sac+ fetal pole +cardiac activity Cardiac activity confirms a live intrauterine pregnancy (rules out a miscarriage) Cardiac activity is usually detected at 5 ½ to 6 weeks from last menstrual period CRL ≥5 mm – fetal cardiac activity present
 Cardiac activity is usually detected at 5 ½ to 6 weeks from last menstrual period. CRL ≥5 mm – fetal cardiac activity present.")
21
Bhcg and progesterone in early pregnancy

22
Serum concentrations of ß-hCG in 443 normal pregnancies
ß-hCG is first detected in maternal serum 6 to 9 days after conception. The levels rise in a logarithmic fashion, peaking 8 to 10 weeks after the last menstrual period, followed by a decline to a nadir at 18 weeks, with subsequent levels remaining constant until delivery Second International Standard ß-hCG Braunstein G D, et al. Am J Obstet Gynecol 1976; 126:

23
Serial ß-hCG The doubling time for a normal IUP is 2 days
ß-hCG peaks at ~10 weeks gestation It can get as high as 100,000 IU/L Doubling of ß-hCG is less reliable after 10 weeks gestation. At this time, pregnancy is better evaluated with U/S 15% of normal IUPs can demonstrate an abnormal rise of ß-hCG Kadar N, et al. Obstet Gynecol 1981;52:162-6

24
ß-hCG up to mIU/ml The minimal rise in ß-hCG for a viable pregnancy is 53% in 48 hours The minimal decline of a spontaneous abortion is 21-35% in 48 hours A rise or fall in serial ß-hCG values that is slower than this is suggestive of an ectopic pregnancy Seeber BE and Barnhart KT. Obstet Gynecol 2006;107:

25
Seeber BE and Barnhart KT. Obstet Gynecol 2006;107:339-413
Hypothetical illustration of the rise, or fall, of serial hCG values in women with an EP 53% 21-35% Seeber BE and Barnhart KT. Obstet Gynecol 2006;107:

26
Serum Progesterone Progesterone level of <10 ng/ml is consistent with an abnormal pregnancy Progesterone level of > 20 ng/ml is consistent with a normal pregnancy McCord ML, et al. Fertil Steril 1996; 66:513-16

27
Spontaneous abortion: background, etiology

28
Spontaneous abortion or miscarriage
Spontaneous abortion is a fetal loss before 20 weeks gestation 80% of miscarriages occur in the first trimester (first twelve weeks) Biochemical pregnancy: A woman has a positive pregnancy test, but does not miss a period (her period might come a few days late) The pregnancy has miscarried very early (~3wks gestation) Ferri: Ferri's Clinical Advisor 2012, 1st ed.
 Biochemical pregnancy: A woman has a positive pregnancy test, but does not miss a period (her period might come a few days late) The pregnancy has miscarried very early (~3wks gestation) Ferri: Ferri s Clinical Advisor 2012, 1st ed.")
29
Normal first-trimester pregnancy
Miscarriage Diagram representing placentation in (a) a normal first‐trimester pregnancy and (b) miscarriage. Note trophoblast plugging of maternal spiral arteries and trophoblast invasion of the decidua and superficial myometrium in the central area of the normally developing placenta (a). By contrast, in the miscarriage (b) there is a shallow trophoblastic invasion and the plugs are loose, allowing premature entry of maternal blood (arrows). © This slide is made available for non-commercial use only. Please note that permission may be required for re-use of images in which the copyright is owned by a third party. Trophoblast plugging of maternal spiral arteries with invasion of the decidua and superficial myometrium in the central area of the normally developing placenta There is a shallow trophoblastic invasion and the plugs are loose, allowing premature entry of maternal blood (arrows)
 a normal first‐trimester pregnancy and (b) miscarriage. Note trophoblast plugging of maternal spiral arteries and trophoblast invasion of the decidua and superficial myometrium in the central area of the normally developing placenta (a). By contrast, in the miscarriage (b) there is a shallow trophoblastic invasion and the plugs are loose, allowing premature entry of maternal blood (arrows). © This slide is made available for non-commercial use only. Please note that permission may be required for re-use of images in which the copyright is owned by a third party. Trophoblast plugging of maternal spiral arteries with invasion of the decidua and superficial myometrium in the central area of the normally developing placenta. There is a shallow trophoblastic invasion and the plugs are loose, allowing premature entry of maternal blood (arrows)")
30
Background Miscarriage is the most common serious pregnancy complication affecting approximately 30% of biochemical pregnancies and 11–20% of clinically recognized pregnancies The diagnosis of miscarriage is made most commonly by trans-vaginal ultrasound (TVS) assessment After a diagnosis of miscarriage, half of women undergo significant psychological effects Cecilia Bottomley, Tom Bourne. Diagnosing miscarriage. Best Practice & Research Clinical Obstetrics & Gynecology 2009; 23:463-77
 assessment. After a diagnosis of miscarriage, half of women undergo significant psychological effects. Cecilia Bottomley, Tom Bourne. Diagnosing miscarriage. Best Practice & Research Clinical Obstetrics & Gynecology 2009; 23:")
31
Etiology Approximately 50–60% of first-trimester spontaneous abortions have karyotype abnormalities Igor N Lebedev, Nadezhda V Ostroverkhova, Tatyana V Nikitina, Natalia N Sukhanova and Sergey A Nazarenko. Features of chromosomal abnormalities in spontaneous abortion cell culture failures detected by interphase FISH analysis. European Journal of Human Genetics 2004; 12:513–20

32
Etiologies The most frequent type of chromosomal abnormalities detected are: Autosomal trisomies ─ 52 % Monosomy X ─ 19 % Polyploidies ─ 22 % Other ─ 7 % Hsu, LYF. Prenatal diagnosis of chromosomal abnormalities through amniocentesis. In: Genetic Disorders and the Fetus, 4th ed, Milunsky, A (Ed), The Johns Hopkins University Press, Baltimore p.179
, The Johns Hopkins University Press, Baltimore p.179.")
33
Classification of miscarriage

34
Clinical classification of spontaneous abortion
Laifer-Narin SL. Ultrasound for Obstetrics Emergencies. Ultrasound Clin ; 6: Type Definition Threatened abortion Vaginal bleeding during the first 20 weeks of pregnancy and no evidence of cervical dilation. <50% of threatened abortions will progress to loss of pregnancy. Missed abortion Intrauterine demise of the embryo without either vaginal bleeding or expulsion of the products of conception. Includes both an embryo with no heart tones (>7mm) or an empty gestational sac (>20mm). Incomplete abortion Vaginal bleeding with dilation of the cervix and partial expulsion of products of conception. Complete abortion Vaginal bleeding with expulsion of all of the products of conception. Inevitable abortion Abortion in progress with cervical dilation but the products of conception have not been expelled.
 or an empty gestational sac (>20mm). Incomplete abortion. Vaginal bleeding with dilation of the cervix and partial expulsion of products of conception. Complete abortion. Vaginal bleeding with expulsion of all of the products of conception. Inevitable abortion. Abortion in progress with cervical dilation but the products of conception have not been expelled.")
35
Threatened Abortion Pregnant patient who is symptomatic with:
Vaginal bleeding Mild abdominal cramps Closed cervical os Complication affecting 16-25% of pregnant patients Increases her chance of spontaneous abortion, but <50% progress to pregnancy loss Chung TKH. Aust N Z J Obstet Gynaecol 1999; 39:

36
Differential Diagnosis of Threatened Abortion
Undetermined or physiologic (implantation related) Ectopic pregnancy Sub-chorionic bleed, found in ~20% of threatened Ab Gestational trophoblastic disease (molar pregnancy) Impending spontaneous miscarriage Cervix, vaginal or uterine pathology
 Ectopic pregnancy. Sub-chorionic bleed, found in ~20% of threatened Ab. Gestational trophoblastic disease (molar pregnancy) Impending spontaneous miscarriage. Cervix, vaginal or uterine pathology.")
37
Ultrasound diagnosis of miscarriage
This section is too in-depth for most medical students; read it for background, but you don’t necessarily have to memorize! Ultrasound diagnosis of miscarriage

38
Comparison of international criteria
Different organizations use different cutoffs to diagnose miscarriage… Comparison of international criteria

39
TVS features of pregnancy failure
Levine D. Radiology 2007; 245: Non visualization of the yolk sac by the time the mean sac diameter is 13 mm, or Non visualization of the embryo by the time the mean sac diameter is 20 mm, or Non visualization of cardiac activity by the time the embryo is 5 mm in length (~7wks gestation). Specificity for diagnosis of nonviable pregnancy is 100%
. Specificity for diagnosis of nonviable pregnancy is 100%")
40
Mean sac diameter greater than 20 mm and no embryonic contents, or
How to define miscarriage using ultrasound-comparing and contrasting national guidelines Royal College of Obstetricians and Gynaecologists. The Management of Early Pregnancy Loss. Green-Top Guideline No. 25. October 2006 Miscarriage: Mean sac diameter greater than 20 mm and no embryonic contents, or Embryo crown-rump length > 6 mm with no heart beat, or If sac remains empty after at least one week or still no cardiac activity 1 week after initial ultrasound

41
Transvaginal Ultrasound Gestational sac > 20 mm
How to define miscarriage using ultrasound-comparing and contrasting national guidelines The Institute of Obstetricians and Gynaecologists Royal College of Physicians of Ireland Transvaginal Ultrasound Embryo > 7 mm No cardiac activity Miscarriage Gestational sac > 20 mm No embryo or yolk sac

42
What is the evidence to support the cut-offs used to diagnose miscarriage?
UOG 2011 November, Jeve Y et al. Systematic review of ultrasound diagnosis of miscarriage Problems: studies are 15–20 years old, small study numbers, and various cut-off values used (4–6mm for CRL, 13–25mm for MSD), making pooling of data impossible Best (most specific) criteria appeared to be MSD > 25mm with a missing embryo or MSD > 20mm with a missing yolk sac These criteria had a 95% CI of 0.96–1.00, therefore up to 4 out of 100 diagnoses of early fetal demise may be wrong. A single incorrect diagnosis of miscarriage is one too many A confidence interval (CI) is a particular kind of interval estimate of a population parameter and is used to indicate the reliability of an estimate.
, making pooling of data impossible. Best (most specific) criteria appeared to be MSD > 25mm with a missing embryo or MSD > 20mm with a missing yolk sac. These criteria had a 95% CI of 0.96–1.00, therefore up to 4 out of 100 diagnoses of early fetal demise may be wrong. A single incorrect diagnosis of miscarriage is one too many. A confidence interval (CI) is a particular kind of interval estimate of a population parameter and is used to indicate the reliability of an estimate.")
43
Prospective multicenter study 1060 patients of IPUV Conclusions
Abdallah Y, et al. Limitations of current definitions of miscarriage using mean gestational sac diameter and crown–rump length measurements: a multicenter observational study. Ultrasound Obstet Gynecol 2011; 38: 497–502 Prospective multicenter study 1060 patients of IPUV Conclusions In order to minimize the risk of a false-positive diagnosis of miscarriage the following cut-off could be introduced Empty gestational sac or sac with a yolk sac but no embryo seen with MSD >25 mm Embryo with an absent heartbeat and CRL > 7 mm

44
Summary Summary Significant interobserver variability may be associated with a misdiagnosis of miscarriage This could result in interventions (D&C, misoprostol use) that could harm a viable pregnancy Current national guidelines should be reviewed to avoid inadvertent termination of wanted pregnancy Large prospective studies with agreed reference standards are urgently required
 that could harm a viable pregnancy. Current national guidelines should be reviewed to avoid inadvertent termination of wanted pregnancy. Large prospective studies with agreed reference standards are urgently required.")
Similar presentations

 of less than 5 mm located within the thickened,>")













 Dr Kamel Elbadry MD (Sheffield University), FRCOG MD (Sheffield University), FRCOG Consultant Obstetrician and Gynaecologist.>")



>")